Living with diabetes – how clinicians can support psychological wellbeing

Diabetes type 1
Diabetes type 2
Psychological distress is common in people living with diabetes, but not routinely addressed in clinical practice. Managing psychological and physical health is the responsibility of all diabetes clinicians. Supporting psychological wellbeing requires a person-centred approach to management, including sensitive and nuanced communication, regular assessment of psychological health and an understanding of potential barriers to the self-management of diabetes.
Correction
A correction for this article was published in the November 2022 issue of Endocrinology Today. The online version and the full text PDF of this article (see link above) have been corrected.
- Poor psychological wellbeing is common in people with diabetes, but often not addressed as part of routine diabetes care.
- Supporting psychological wellbeing can improve diabetes self-management.
- Asking about psychological health is as important as enquiring about physical health.
- People with diabetes want to be asked about their emotional health, and for their healthcare professionals to understand their experiences.
- Person-centred care supports the psychological wellbeing of people living with diabetes.
‘Think about how discouraging it is to fail at something you really wanted to do. Then consider what it must feel like to have diabetes and be failing at something you never, ever, wanted to do in the first place.’
Joan Williams Hoover, 19881
Living with diabetes can be tough. Self-managing diabetes often requires difficult lifestyle changes. The effort is greater still if taking insulin, as moment-to-moment awareness and consideration are necessary to avoid high or low blood glucose levels (BGLs). Even when the best care is taken and the most changes or sacrifices are made, ‘perfect’ health behaviour may not translate into ‘perfect’ BGLs. This can be demotivating. Nonbehavioural (i.e. out of direct control) factors, such as health changes, emotional state, medications, physical activity, stress or variable insulin absorption, can also affect blood glucose levels. All this occurs under the spectre of possible future complications.
Diabetes distress refers to the emotional burden of living with diabetes – the constant awareness, decision-making and potential sacrifices that are needed for optimal BGL range. It can impact profoundly on diabetes self-care and lead to poorer quality of life. For these reasons, psychological health in people with diabetes should be regarded as equally important to physical health.
Prioritising the psychological care of people living with diabetes was raised 40 years ago.1,2 However, evidence suggests that many people with diabetes still do not receive the psychological support they need for optimal functioning. This article outlines the common psychological challenges for people living with diabetes and presents practical strategies and resources for clinicians to help support the psychological wellbeing of people with diabetes.
Psychological distress in people living with diabetes
There is extensive evidence that psychological distress is common in people with diabetes. The Diabetes Management and Impact for Long-term Empowerment and Success (MILES) studies provide a snapshot of the psychological, behavioural and social aspects of living with diabetes in Australia.3 Severe diabetes distress was reported by nearly 25% of participants with type 1 diabetes and 20% of those with type 2 diabetes who were treated with insulin. People with diabetes also have a reduced quality of life in many domains and are at increased risk for psychological conditions such as depression, eating disorders and anxiety.3-5 These factors have a bidirectional relationship with diabetes distress, each worsening the impact of the other, and leading to deterioration of diabetes self-care.4
Psychological distress is not routinely addressed
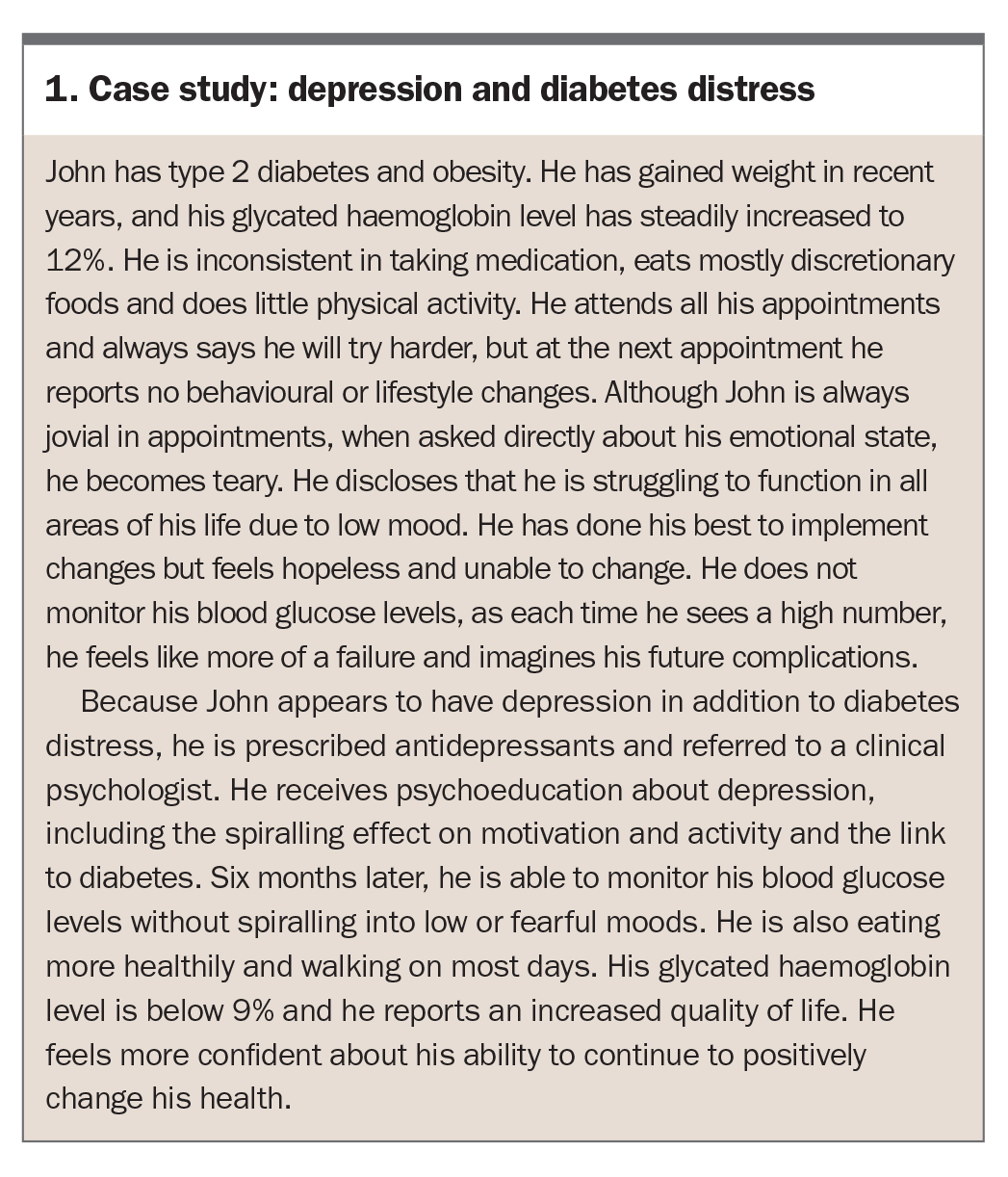
Numerous studies have shown that, although psychological distress is common in people with diabetes, it is not routinely addressed in clinical practice. For example, the multinational Diabetes Attitudes Wishes and Needs (DAWN) study found that diabetes-related distress and depression were prevalent and linked to suboptimal diabetes self-management.6 However, only 3.3% of people with diabetes had received psychological treatment for diabetes-related problems within the five years before the survey. Strategies were implemented to raise awareness in healthcare professionals; however, person-centred diabetes care and psychosocial support remained low ten years later.7 A case study of a person with depression and diabetes distress is presented in Box 1.
{kind=link}
Treatment of psychological distress improves outcomes
The lack of routine attention to psychological wellbeing in diabetes is concerning. It is a missed opportunity for improved health. Evidence suggests that attending to psychological factors as part of diabetes treatment can improve psychological wellbeing, metabolic outcomes and quality of life.8,9
Supporting psychological wellbeing in people living with diabetes
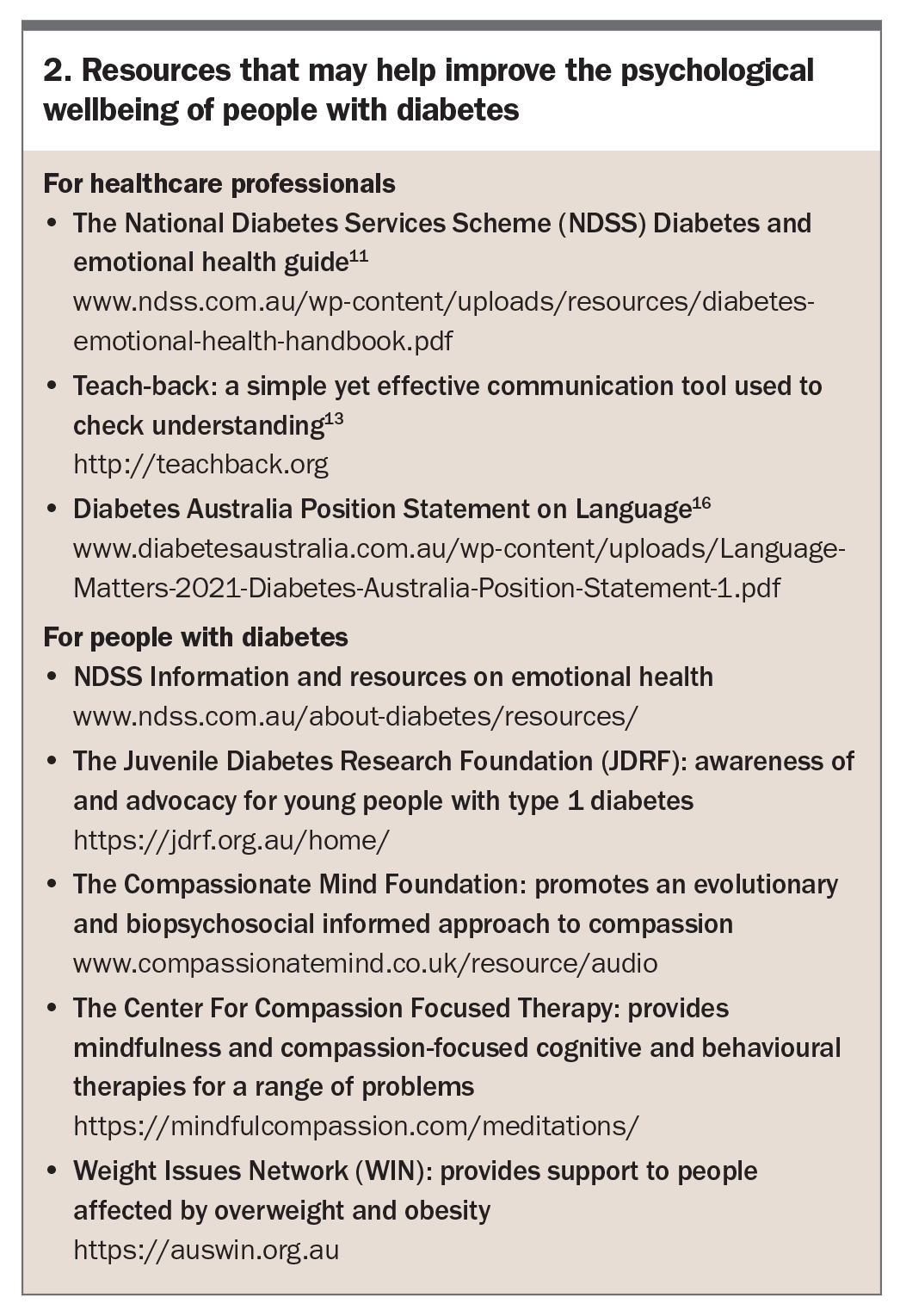
Diabetes clinicians play a role in supporting the psychological wellbeing of all people with diabetes.5,10 The National Diabetes Services Scheme (NDSS) Diabetes and emotional health guide includes comprehensive information for the assessment and management of psychological distress, and for the appropriate referral to mental health specialists. It is available for free download (www.ndss.com.au/wp-content/uploads/resources/diabetes-emotional-health-handbook.pdf).11
Clinicians will encounter barriers while supporting the psychological wellbeing of people with diabetes. Some of these can be reduced by clinician behaviours and attitudes. A stance of person-centred care is necessary, with the aim of integrating the person’s preferences, values, beliefs, culture and abilities into the process of decision-making. The resulting treatment plan is more likely to be appropriate and meaningful. Following are some areas where clinicians can upskill to support the psychological wellbeing of people living with diabetes. Resources for helping to improve psychological wellbeing of people living with diabetes are summarised in Box 2.
{kind=link}
Communication
A frequent barrier to person-centred care is communication – a surprisingly complex skill. Good communication ensures optimal exchange of information, so that important topics are broached, and both parties have the same understanding of what has been said.
Check understanding of a consultation
At its most basic level, good communication involves checking that both parties agree on what has occurred in a consultation. In the DAWN 2 study, about half the clinicians surveyed reported that they had asked how diabetes affects the lives of people with diabetes. However, only about a quarter of people with diabetes reported they had been asked.7 This is not surprising, as both parties in an outpatient consultation have poor recall of decisions made, and clinicians can recall details that were not present.12
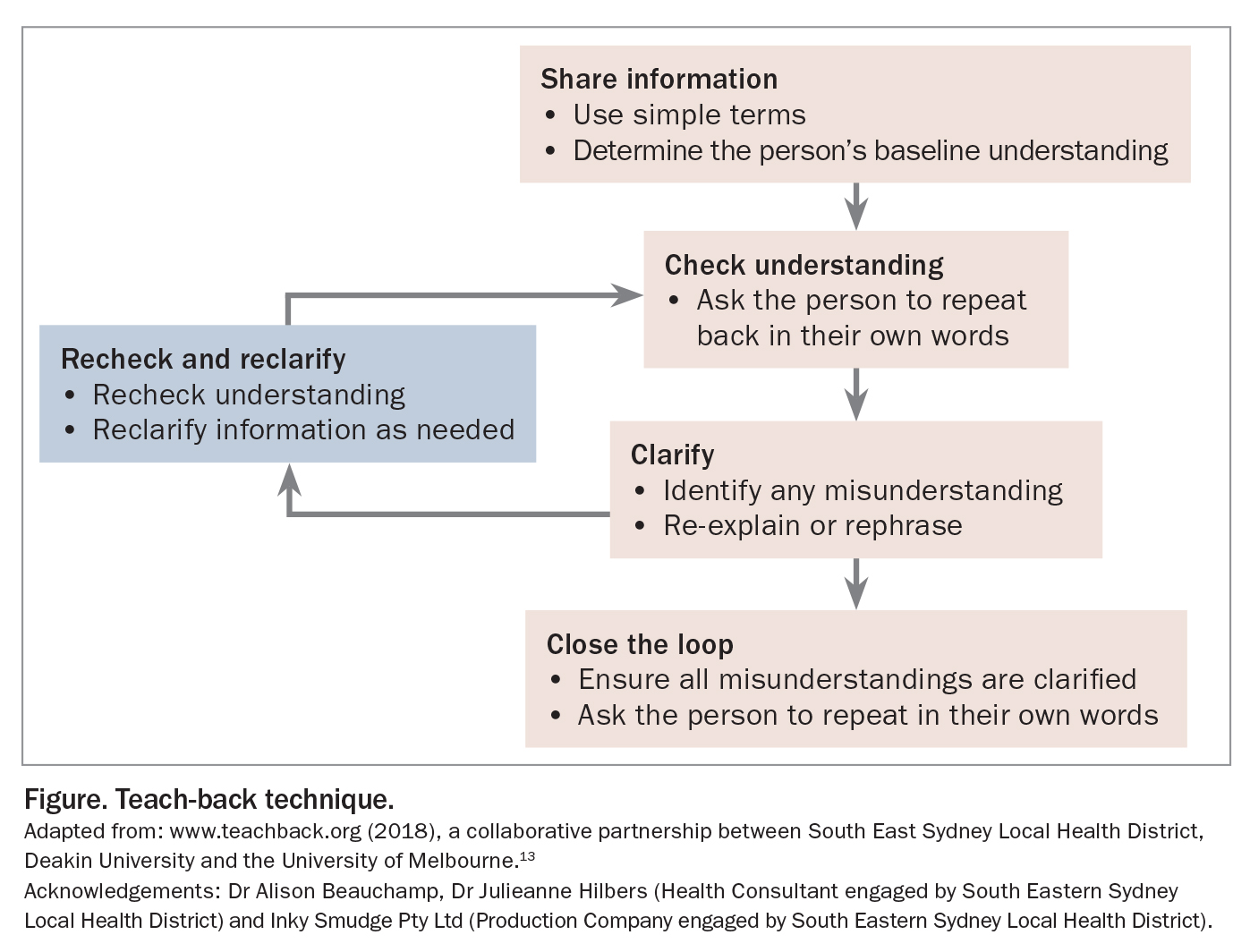
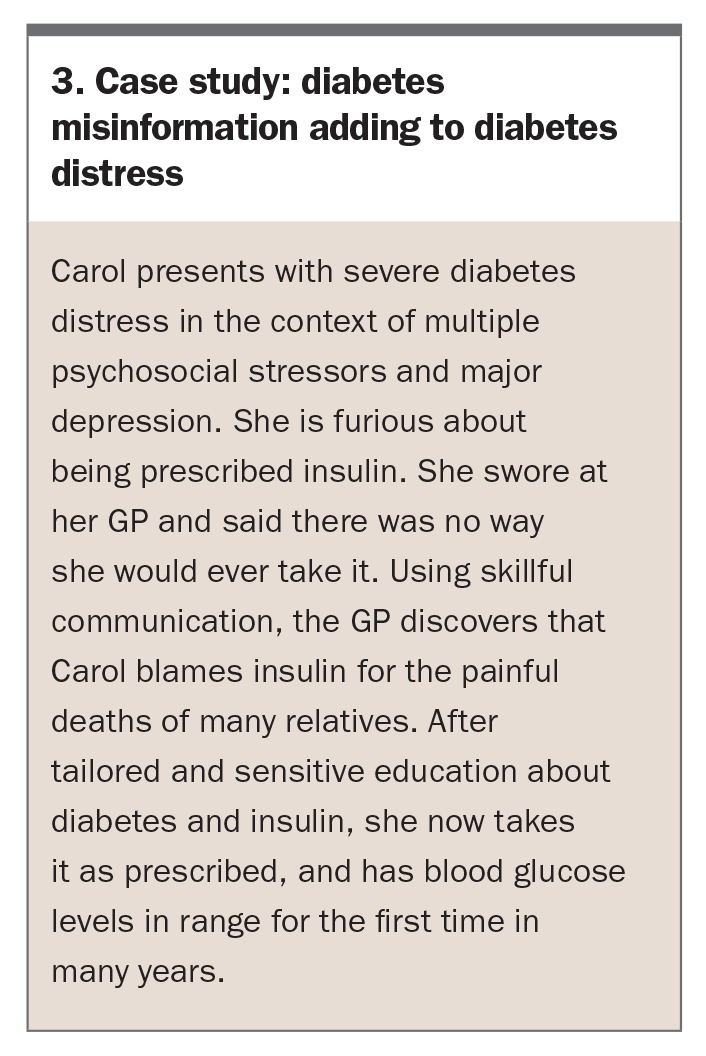
A mismatch in understanding of what occurred in a consultation can compound psychological distress. To increase clarity, clinicians may consider the teach-back technique, which focuses on delivering bite-sized pieces of information using simple language and seeking clarification of understanding from the other party before the end of a consult.13 Teach-back has been shown to be effective in improving health-related outcomes. A summary of the steps is presented in the Figure.13 A case study of misinformation contributing to diabetes distress is presented in Box 3.
{kind=link}
{kind=link}
Notice own biases and responses
At a more complex level, good communication involves a shift in mindset to become more aware of one’s own biases, beliefs and reactions.14 This helps to create a safer environment and promotes the discussion of sensitive topics, such as feelings of sadness or failure that can drive counterproductive behaviour. Discussing emotional barriers can be the first step in negotiating change with a person with diabetes. Clinicians can empower themselves to communicate better by engaging in professional development and training that includes active skill acquisition strategies (such as role play) rather than simply didactic teaching.15
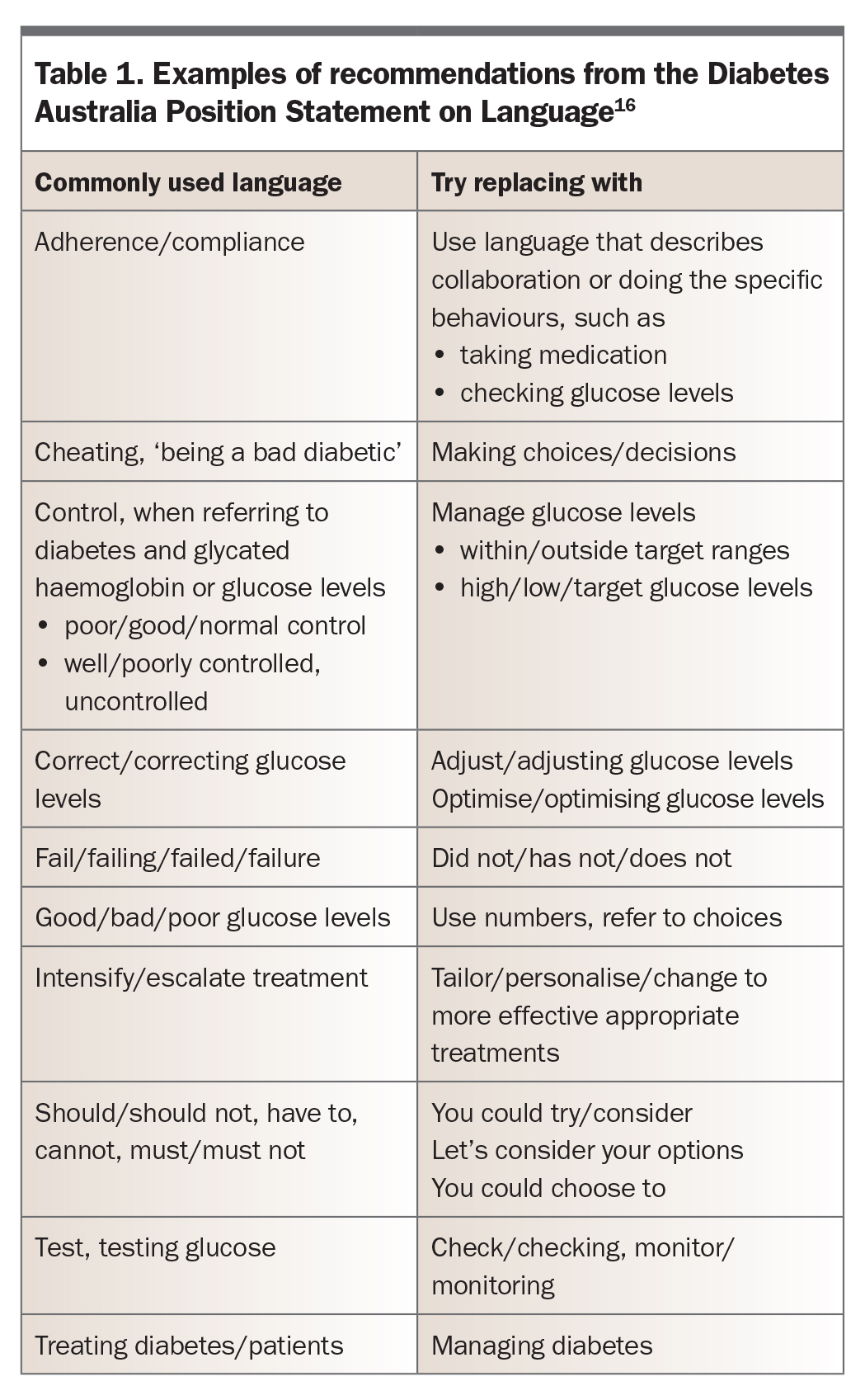
Use language with care
Using sensitive language is crucial to optimal communication.16 Poorly chosen language can create a power imbalance, promote a sense of failure and strengthen unhelpful assumptions about diabetes management, for example, that BGL is directly within ‘control’ of the individual. On the other hand, well-chosen language can strengthen rapport, build hope and increase the person’s willingness to continue to try during difficult times. Examples of recommendations on language use from the Diabetes Australia Position Statement on Language are presented in Table 1.16
{kind=link}
Understand and attend to diabetes distress
Assess and address distress regularly
Clinicians should ask about the psychological wellbeing of each individual at every consultation, regardless of whether they believe psychological distress is present or not. Many people will not offer this information if not directly asked, and most people with diabetes welcome questions about their emotional state and coping.17 Detecting and addressing distress early prevents exacerbation of diabetes distress and potential reduction in self-care, quality of life and mood. It is equivalent to routine screening for diabetes complications to prevent worsening of harm.
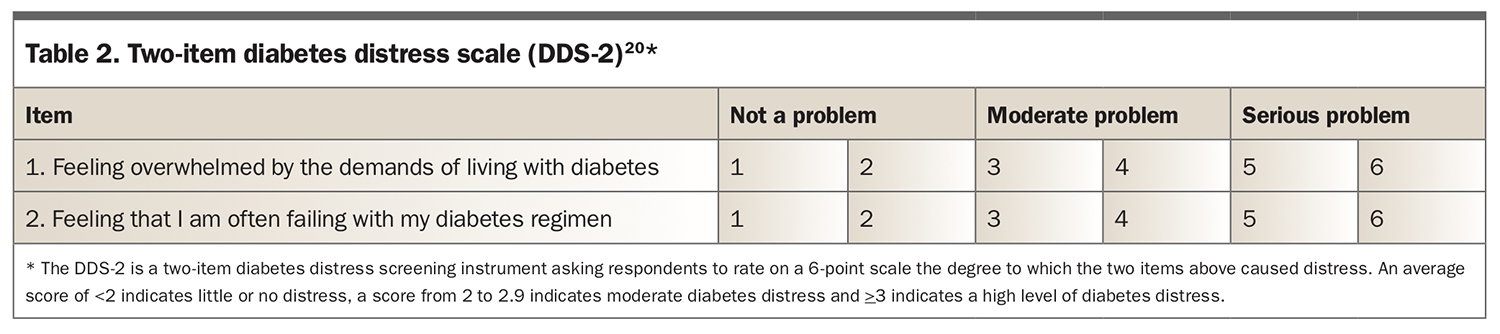
Questionnaires such as the Problem Areas In Diabetes (PAID) Scale or the Diabetes Distress Scale (DDS) can be used to help integrate screening for psychological wellbeing into usual practice.18,19 Quicker methods include short written screeners, such as the two-item DDS (Table 2) or the one-item PAID measure.20,21 Alternatively, clinicians can ask about changes in mood since the last visit, new barriers to self-management of diabetes or even ask, ‘What is driving you crazy about your diabetes?’.5,22 If the screening process suggests the presence of diabetes distress, a person-centred discussion of management options, including guidance with a specific intervention, more frequent appointments for a given period or referral to a diabetes clinician skilled in working with people with diabetes distress, should be undertaken. Any solutions should feel realistic and achievable to the person with diabetes. Brochures on various emotional health topics such as diabetes distress, depression and how to get support from a psychologist are available from the NDSS (www.ndss.com.au/about-diabetes/resources/).
{kind=link}
Be aware of common themes of diabetes distress
Although areas of struggle vary between people with diabetes, several themes of distress are recurring. Items on the PAID and DDS questionnaires can be a guide to frequent areas of concern.18,19 In the Diabetes MILES-2 study, sources of diabetes distress varied widely, but common causes included difficulties with food and eating, or fear of hypoglycaemia.3 The most reported problem areas were:
- worry about the future and the possibility of serious complications (28% and 17% in those with type 1 and type 2 diabetes, respectively)
- feelings of guilt and anxiety when individuals get off track with their diabetes management (23% and 16% in those with type 1 and type 2 diabetes, respectively).
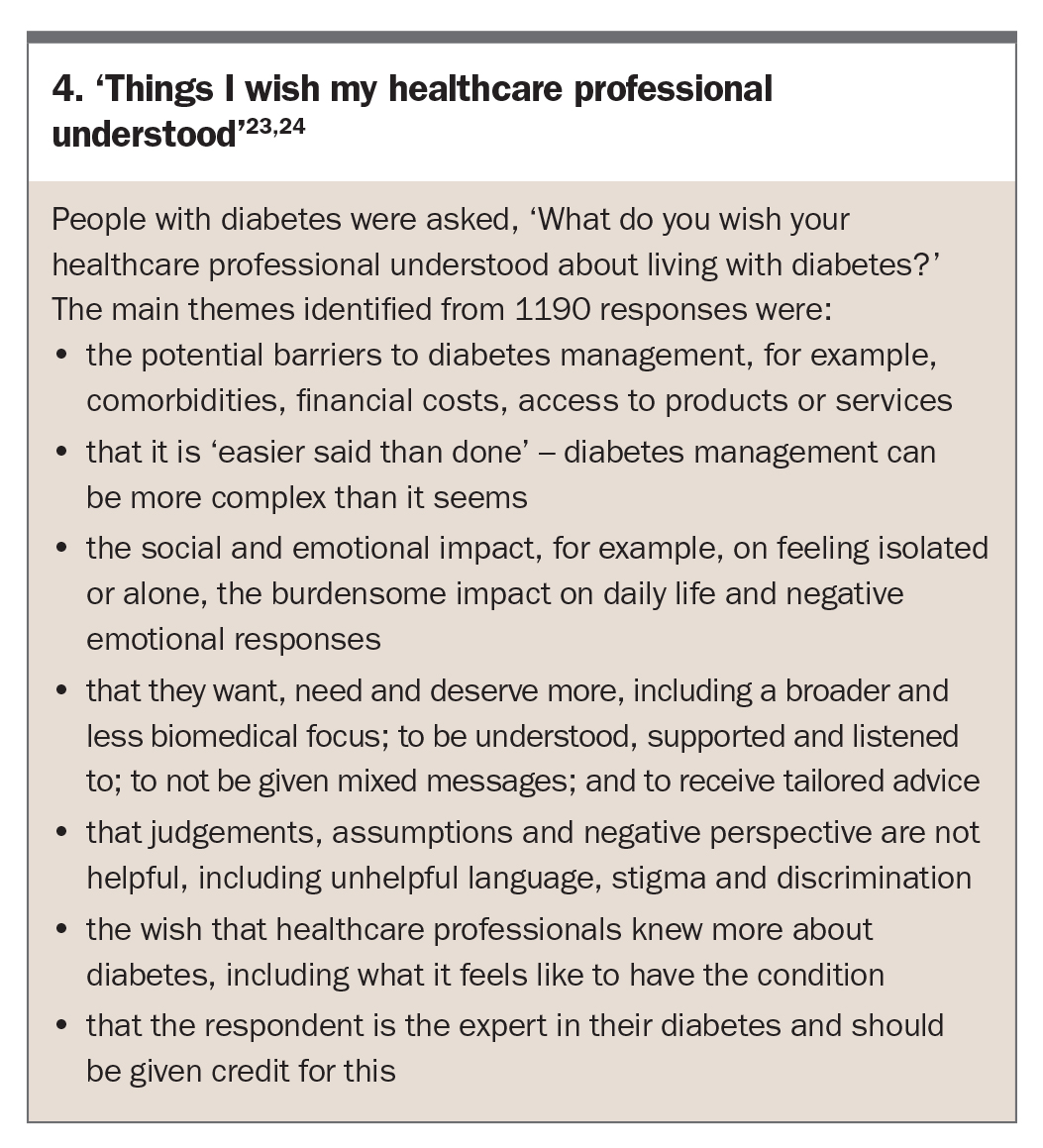
Results of this study also suggested that clinicians are often perceived to lack understanding regarding the burden of diabetes. Responses to ‘What do you wish your health professional understood about living with diabetes?’ identified themes suggesting that many people with diabetes would appreciate an increase in person-centred care (Box 4).23,24
{kind=link}
A common theme of distress for people living with obesity is the stigma, blame and weight bias often experienced from within the healthcare system. It is important to use sensitive language and be explicit that they are not to blame for the disease. Rather it is a problem of physiology with complex multifactorial triggers and a large genetic component; it is chronic and relapsing; and lifetime health support is needed. This can help people manage the condition in a realistic and sustainable way.25
Understand the potential benefits of shared experience
Peer support can be invaluable for some individuals with diabetes. It can be a relief to discover shared challenges of living with diabetes and ‘normalise’ common difficulties. Peer networks can also be a great source of support for self-management. They can facilitate knowledge of and access to skills and resources.26
Shared medical appointments can be an efficient way to provide treatment while facilitating peer networking.27,28 Groups such as state diabetes organisations or the juvenile diabetes research foundation (JDRF) often have existing support groups, and various organisations run walking groups. Weight issues network (WIN) provides support to people affected by overweight and obesity (Box 2). Social prescribing, involving referral to community activities to support social, emotional or practical needs, could be considered, with some studies suggesting it can lead to a reduction in healthcare usage.29,30
Setting expectations
Give hope (counter fear-based messaging)
Fear-based messaging about diabetes is common in the media, which focus on complications that can occur, rather than the benefits of a particular behaviour.31 This can lead many people with diabetes to feel hopeless and give up on self-care, particularly if friends or family members with diabetes have experienced complications. Providing up-to-date information on ways to improve long-term health can promote hope, and includes:
- providing information about published clinical trials with inspiring outcomes
- giving (deidentified) examples of how others managed to improve their health
- providing information on the Kellion Victory Medal, given to those who have lived with diabetes for 50 years or more.22
Be realistic
People can place high value on their clinicians’ predictions, and it can be devastating when a specific event does not eventuate.32 Clinicians should focus on collaboratively setting realistic and sustainable goals based on behaviours that are under the person’s direct control (e.g. increasing activity, taking medication) and avoid setting goals that cannot be directly controlled (e.g. outcomes such as weight or BGLs).
Counter guilt and anxiety about getting off track
Coaching people with diabetes to understand that setbacks are normal can reduce relapse. Individuals can learn to treat ‘failures’ as a necessary part of the process of change, and learn from them.33 Helping individuals ‘take a long view’ and understand health as a sum of many small actions rather than focusing on one action or mistake can remove the pressure to be perfect each time.34 Learning self-compassion skills can help people to cope with setbacks, and many resources are available, including free audio practices, online resources and self-help books (Box 2).35,36
Use diabetes technology wisely
Set up the use of technology to maximise the chance of a successful outcome. This includes careful assessment of barriers to consistent and appropriate technology use, such as excessive anxiety, unrealistic expectations, disempowerment or poor health literacy, lack of financial capacity, lack of technical knowhow or poor executive functioning. Skill training may help in reducing barriers to consistent technology use.37 Monitor the use of technology and provide alternatives when it is not helping or is making things worse. The aim is to avoid a negative experience, which may reduce the chances of future positive uptake.
Conclusion
For people living with diabetes, good psychological health is a foundation for optimal self-care. Psychological and physical wellbeing should be viewed as equally important. Improving physical and psychological outcomes can improve quality of life, supporting people with diabetes to thrive. The behaviour of clinicians can impact greatly on how a person feels about their diabetes and affect their self-care. All diabetes clinicians can, and should, play an important role in supporting the psychological wellbeing of people with diabetes. ET
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.