Type 1 diabetes – a guide to current technologies

Glucose monitoring and insulin delivery devices can improve glucose levels and engagement, and provide convenience for people living with type 1 diabetes. Advances in continuous glucose monitoring (CGM) and insulin pump therapy have improved the management of type 1 diabetes, and recent changes to eligibility criteria allow all people with type 1 diabetes to access subsidies for CGM. An appropriate device should be selected in consultation with a qualified clinician and education provided on troubleshooting and risks.
- Current glucose monitoring and insulin delivery technologies can improve care in people living with type 1 diabetes.
- Continuous glucose monitoring (CGM) allows for real-time blood glucose information, potentially improving blood glucose levels and reducing the risk of hypoglycaemia.
- Since 1 July 2022, subsidised CGM is available to all people with type 1 diabetes.
- Automated insulin pump therapy can reduce nocturnal and severe hypoglycaemia and improve glycaemic targets.
- Identifying suitable candidates for insulin pump therapy is important to optimise the benefits.
Continuous glucose monitoring (CGM) and insulin pump therapy are the latest diabetes technologies to revolutionise management of type 1 diabetes. Monitoring blood glucose levels in people with diabetes allows glycaemic aberrations to be recognised and corrected, for example, through triggering and guiding insulin dose correction, detecting and treating hypoglycaemia and assisting in analysing the impact of carbohydrate intake and physical activity. This article provides an update on the latest diabetes technologies including CGM devices and insulin pumps.
Historically, glucose monitoring for people with diabetes required self-monitoring of blood glucose levels by finger prick testing to assess day-to-day glucose fluctuations, and glycated haemoglobin (HbA1c) testing to estimate chronic metabolic control. The development of CGM devices has removed barriers to glucose monitoring and is associated with improved glycaemic levels, hypoglycaemia risk and quality of life.1,2 Recognising its benefits, the Australian Government introduced a CGM subsidy in April 2017 for select groups of individuals with type 1 diabetes.3 As of 1 July 2022, eligibility for subsidised CGM has been expanded to include all people with type 1 diabetes.4 CGM is now recommended over self-monitoring of blood glucose alone for all adults with type 1 diabetes.5
Insulin pumps provide a continuous delivery of subcutaneous short-acting insulin to reduce the burden of frequent insulin injections, allow for flexible dosing and help calculate insulin bolus doses. Technological advancements have allowed for insulin pumps to function as hybrid closed-loop systems in conjunction with CGM devices and provide automated basal insulin delivery, reducing hypoglycaemia and improving time in glycaemic range.
Continuous glucose monitoring
A continuous glucose monitor is a wearable device that provides a measure of interstitial fluid (ISF) glucose levels. The three main components of a CGM device are: a disposable filament sensor inserted into the subcutaneous tissue below the skin, a transmitter attached to the sensor and a receiver that receives displays and stores data sent from the transmitter via Bluetooth.6 The device (consisting of sensor and transmitter) can be worn on the abdomen, arm or buttocks, depending on the device type. There are three forms of CGM.
- Retrospective, in which blinded data is collected for a short period then downloaded to review trends in glycaemic data, does not provide real-time data and is typically only used by healthcare professionals.
- Real-time (rt-CGM), which provides immediately available sensor glucose data, allows the user to set alarms for hyper- and hypoglycaemia, and can detect the direction and rapidity of change in blood glucose levels.
- Intermittently scanned or flash (is-CGM), which displays sensor glucose data only when scanned using a reader device. A flash device can store data and alert for low and high blood glucose levels for eight hours from the last scan.
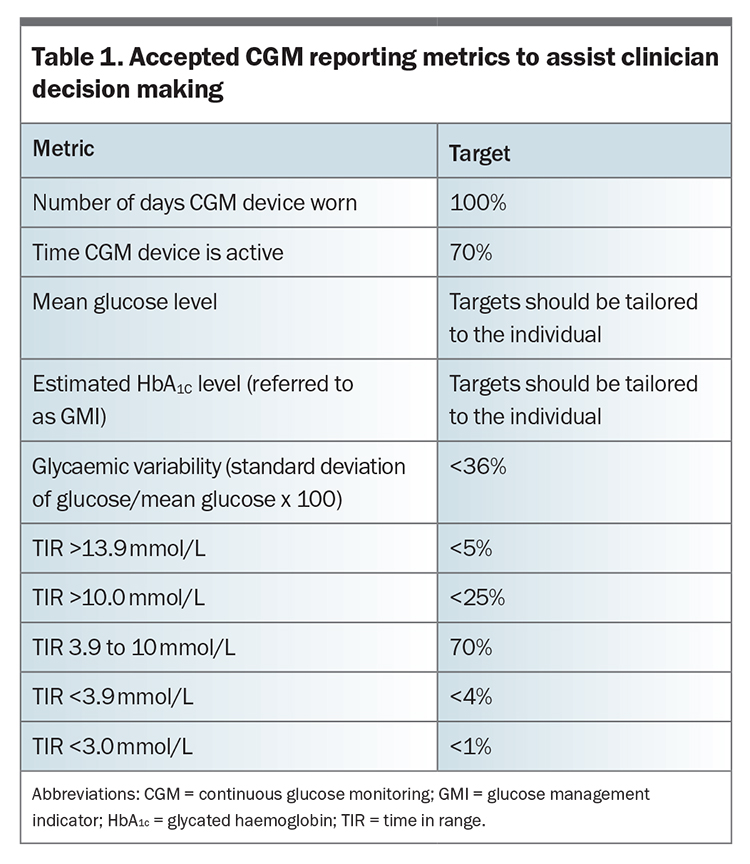
Continuous glucose monitors provide more clinically meaningful and uninterrupted glucose monitoring data compared with finger prick glucose testing, which provides a single static reading only. Use of CGM provides an ambulatory glucose profile (AGP) report that summarises CGM data over multiple days of wear. Data recorded over 14 days have been found to correlate well with data recorded over three months for mean glucose levels, time in range (TIR) and hyperglycaemia.7 Internationally accepted metrics for reporting CGM data are provided in the AGP and supplement regular HbA1c testing.8 TIR (% time spent in the target glucose range of 3.9 to 10.0 mmol/L) is a key CGM-based measure of glycaemic levels. Consensus guidelines recommend a TIR target of above 70% for optimal glycaemic outcomes.7,9 Other CGM-based reportable measures and targets are detailed in Table 1.7,10
{kind=link}
Accessing CGM devices
Although the use of CGM devices improves HbA1c and glycaemic levels in adults with type 2 diabetes treated with insulin, currently only people with type 1 diabetes are eligible to apply for subsidised CGM through the National Diabetes Services Scheme (NDSS).11-13 Each CGM device must be registered by a credentialled diabetes educator or endocrinologist. CGM devices are fully subsidised for healthcare card holders, women planning or during pregnancy and people aged under 21 years; however, all others contribute a copayment of the equivalent of $32.50 each month (at the time of article publication). When registering individuals with diabetes with the NDSS, clinicians must carefully consider whether the person has type 1 or type 2 diabetes, as incorrect diagnosis impacts their ability to access the CGM subsidy.
What are the benefits and drawbacks of CGM?
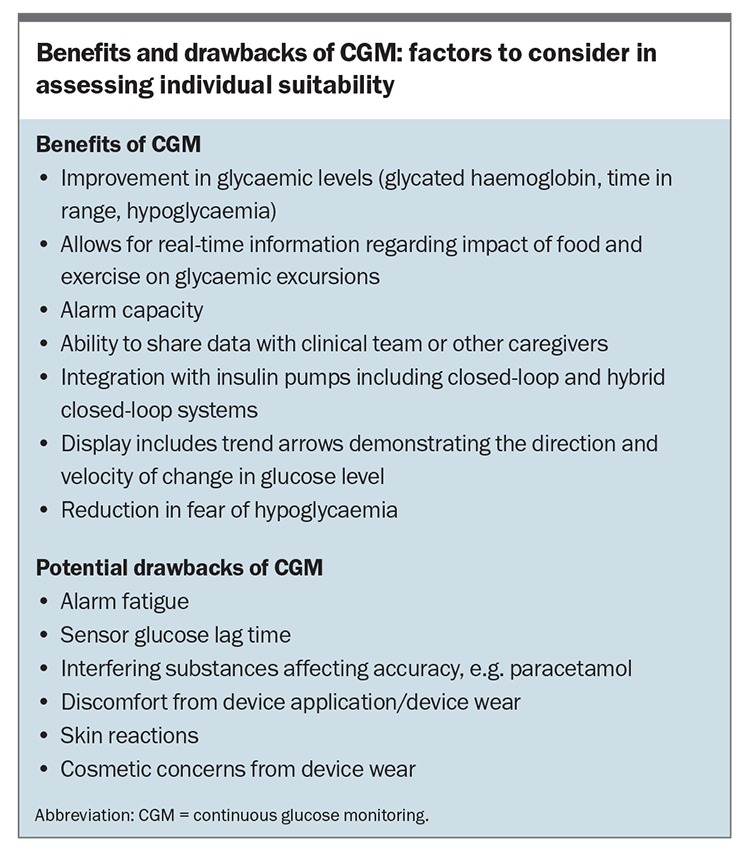
CGM can assist individuals with the day-to-day aspects of managing diabetes and as a tool to improve glycaemic levels. Demonstrated metabolic benefits include a reduced risk of hypoglycaemia and improved TIR and HbA1c levels.14 HbA1c reductions with CGM in real-world and clinical trials were similar and, on average, were reduced by 0.6%.15 Although some studies have not shown a decrease in severe hypoglycaemia, CGM device users did have a reduction in ketoacidosis in real-world studies.3 Individual perceived benefits of CGM include reduced fear of hypoglycaemia among children with type 1 diabetes and their parents and improved quality of life.16,17 Benefits and drawback of CGM are summarised in the Box.
{kind=link}
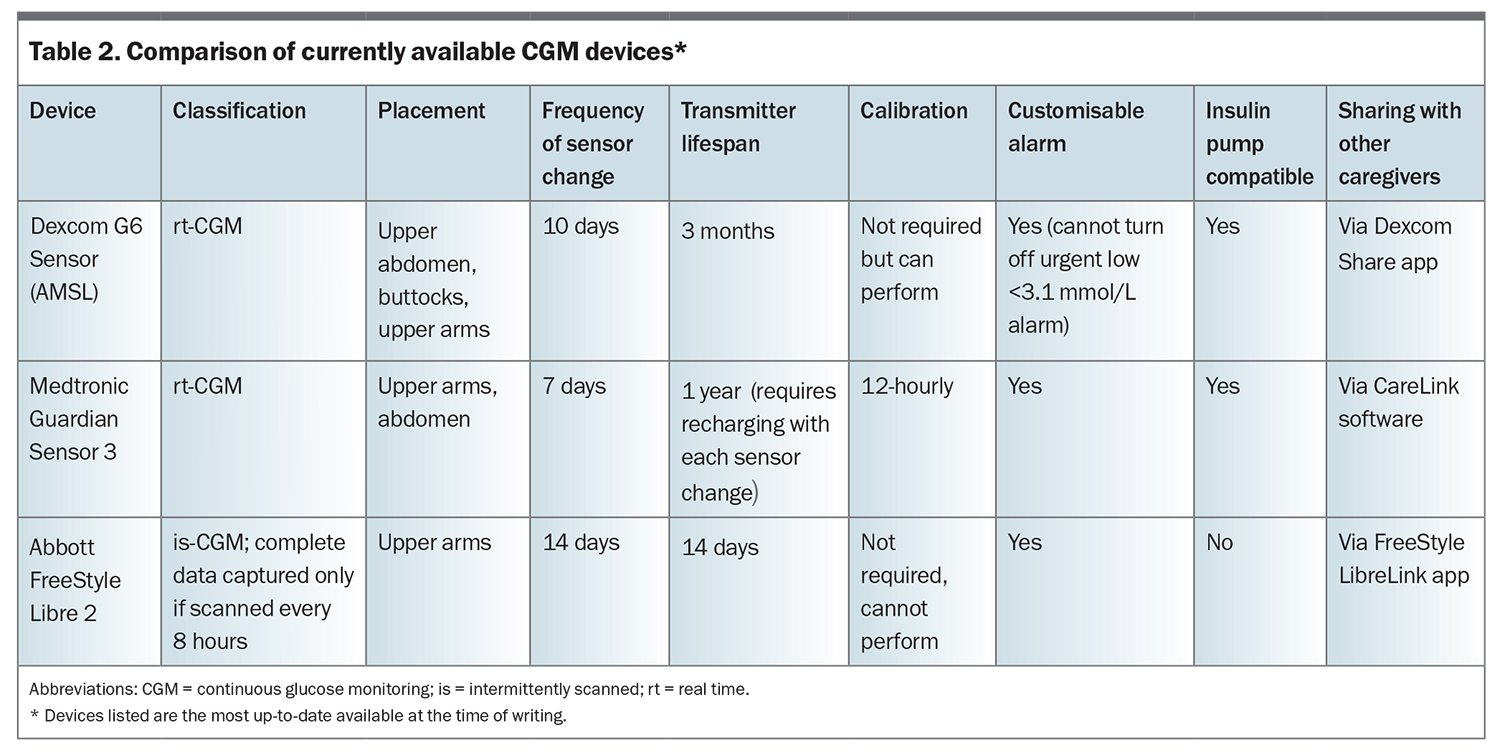
Three main CGM device options are currently available for individual use (Table 2). The ideal option depends on how well the features suit the needs and circumstances of the individual with diabetes. The choice of device should be made by the person living with diabetes in consultation with their endocrinologist or credentialled diabetes educator.
{kind=link}
CGM lag-time
ISF glucose levels correlate closely with blood glucose levels. However, there are some differences between ISF and blood. Blood glucose values represent the whole-body sum of metabolic processes, including glucose uptake by all tissues and postdigestion glucose release, whereas ISF glucose levels represent local level glucose only. Glucose concentrations in the ISF are impacted by local conditions, such as local circulation level, which affects glucose diffusion from the blood into the ISF, and local metabolism of glucose by active tissues.18 A potential time lag occurs in the correlation of ISF to blood glucose values as glucose is drawn from the bloodstream into the interstitial compartment in the subcutaneous space.19
When blood glucose levels are stable, there is minimal physiological lag time and no significant difference should be seen between finger-prick glucose levels and CGM levels.20 When glucose levels change rapidly (e.g. during exercise, during or after a hypoglycaemic episode or after eating), there may be a lag in equilibrium between glucose in the ISF compartment and that in the blood. The subsequent lag time between blood and sensor glucose values is variable (typically five minutes). People with diabetes and clinicians must be aware of this potential lag when using CGM to make treatment decisions and avoid overtreatment of hyper- or hypoglycaemia.
Troubleshooting CGM issues
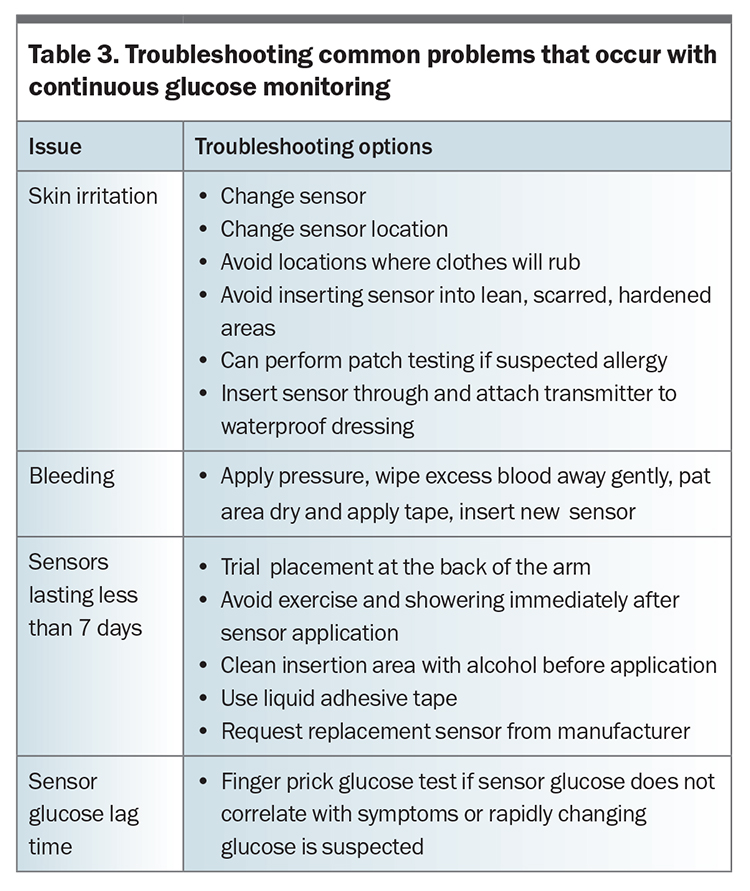
The most common issues arising from CGM use relate to skin irritation, bleeding at the insertion site, sensor failure, sensor glucose lag time or mismatch between finger stick glucose and sensor glucose. These issues can be managed using simple troubleshooting steps outlined in Table 3.
{kind=link}
Insulin pumps
Insulin pump devices allow continuous delivery of subcutaneous short-acting insulin and consist of the following three main components.
- The insulin pump device, which has a display, battery and insulin reservoir. Insulin dosing and delivery rates can be programmed into this device.
- An infusion set that attaches to the skin with a subcutaneous cannula for insulin delivery.
- Thin plastic tubing connecting the insulin reservoir of the pump to the infusion set.
Insulin pumps have come a long way since the large backpack-like early prototypes of the 1960s and the first wearable insulin pump in 1976.21 Technological advancements have allowed them to become more compact and easier to program to the individual’s needs, adding to their convenience and appeal. Tubeless options are also available, with insulin reservoirs attached directly to subcutaneous cannulas, which can connect directly to a mobile phone.22 Individuals considering initiating insulin pump therapy should discuss their preferences with an endocrinologist or credentialled diabetes educator.
What are the benefits of insulin pumps?
Insulin pumps allow for improved glycaemic levels when switching from multiple daily injections, with clinically significant reductions in HbA1c levels of −0.3 to −1.1% reported.23 Insulin pumps also allow for ease of insulin delivery including:8
- flexible dosing, which more closely resembles physiological insulin delivery and is useful for people who exercise regularly, have varying daily schedules (e.g. shift workers) or to address the dawn phenomenon, where increased insulin delivery is needed before dawn and on rising
- the ability to calculate insulin boluses, including preprogramed calculations that help administer the correct bolus dose at mealtimes or for hyperglycaemic corrections, which helps prevent excess dosing by taking into account previous bolus doses administered (‘insulin on board’)
- availability of electronic data on insulin dosing and glucose levels throughout the day, which are stored and can be accessed on the device. This replaces the need to keep a manual insulin diary and helps identify potential dosing issues, which can assist with interpretation of blood glucose readings at physician consultations.
Automated insulin pump systems
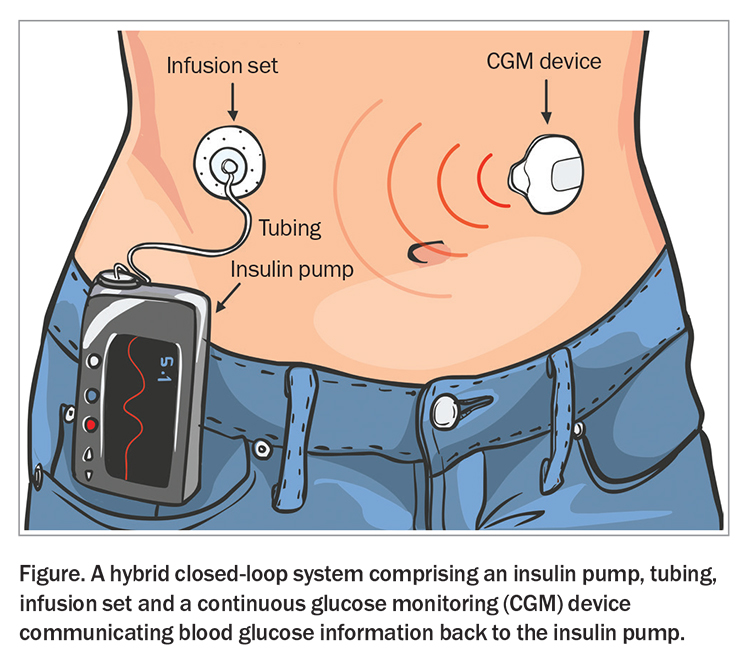
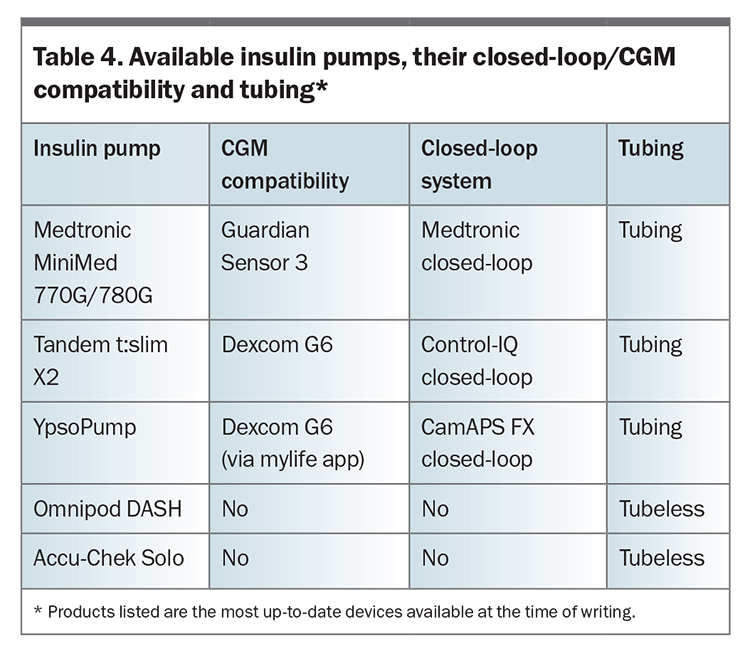
In recent years there have been vast improvements in insulin pump technologies and capabilities. Although CGM devices and insulin pumps can function as standalone devices, newer insulin pumps can function as a hybrid closed-loop system that allows the pump to directly interact with a CGM device, automatically altering the basal insulin delivery according to a programmed algorithm in response to ambient glucose levels (Figure). For instance, if the CGM device detects a rising blood glucose level above that of an individual’s preprogramed glucose target, the pump increases the amount of insulin being delivered to return their blood glucose level to within the target range. Conversely, if the person’s blood glucose is trending downward and they are at risk of hypoglycaemia, the pump can temporarily reduce or suspend the insulin being delivered to prevent a hypoglycaemic event. This can reduce the amount of severe and nocturnal hypoglycaemia, and improve TIR.24-26 Available insulin pumps, their closed-loop/CGM compatibility and tubing type are listed in Table 4.
{kind=link}
{kind=link}
Who is the best candidate for insulin pump therapy?
Although there are multiple benefits of insulin pumps, not all people with type 1 diabetes will be suitable for the device. Some people find it burdensome to wear an insulin pump and set, particularly those in physical occupations or environments unsuitable for insulin pump use. Out-of-pocket costs also need to be considered and include the cost of the pump device (particularly for those without private health insurance coverage) and running costs (the cost of consumables). Other considerations when identifying candidates for pump therapy include willingness to use the device and to follow up regularly with appropriately trained health professionals.
Although automated insulin pump systems may improve blood glucose levels, they still require the person with diabetes to monitor their carbohydrate intake, administer insulin bolus for meals and change their infusion sets every two to three days. Additionally, there are risks of malfunction, most commonly through infusion set occlusion. Therefore, it is important that pump users are educated on how to identify, troubleshoot and solve such issues to prevent progression to diabetic ketoacidosis secondary to insulin deficiency. Ketosis can occur two to four hours after interruption of insulin supply as pumps only use short-acting insulin. Common problems and troubleshooting strategies are listed in Table 3.
Conclusion
Advancements in diabetes technology, coupled with improved accessibility from government subsidies, have contributed to improved quality of life and glycaemic levels in people living with type 1 diabetes. The choice of device should be made in consultation with the individual’s diabetes specialist, with careful assessment of the benefits and drawbacks, and taking into account the person’s lifestyle and preferences. Appropriate education should be provided to individuals and clinicians on risks and troubleshooting common issues associated with the chosen device. ET
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.