Pancreas and islet transplantation in diabetes. Who is eligible?

Diabetes type 1
Diabetes type 2
Pancreas and islet transplantation offer recipients greatly improved quality of life and the possibility of a cure of diabetes. Both are associated with reduced mortality and diabetes-complications risks but they have very different suitability criteria. Suitable patients should be considered for assessment with consideration of the long-term burden of immunosuppression on the patient.
- Pancreas and islet transplants offer eligible patients with type 1 diabetes improved quality of life.
- Whole pancreas transplantation in Australia is usually performed with a kidney transplant (simultaneous kidney-pancreas transplant; SKPT).
- SKPT has a high long-term success rate and improves kidney-transplant outcomes.
- Islet transplantation is a less invasive procedure suitable for select people with type 1 diabetes who have good renal function, and is very successful at ameliorating severe, recurrent hypoglycaemia.
- Both forms of transplantation require long-term immunosuppression, and the potential side-effects of these must be considered for each patient.
- If a patient is interested in having and may be suitable for a transplant, consider referring them for assessment.
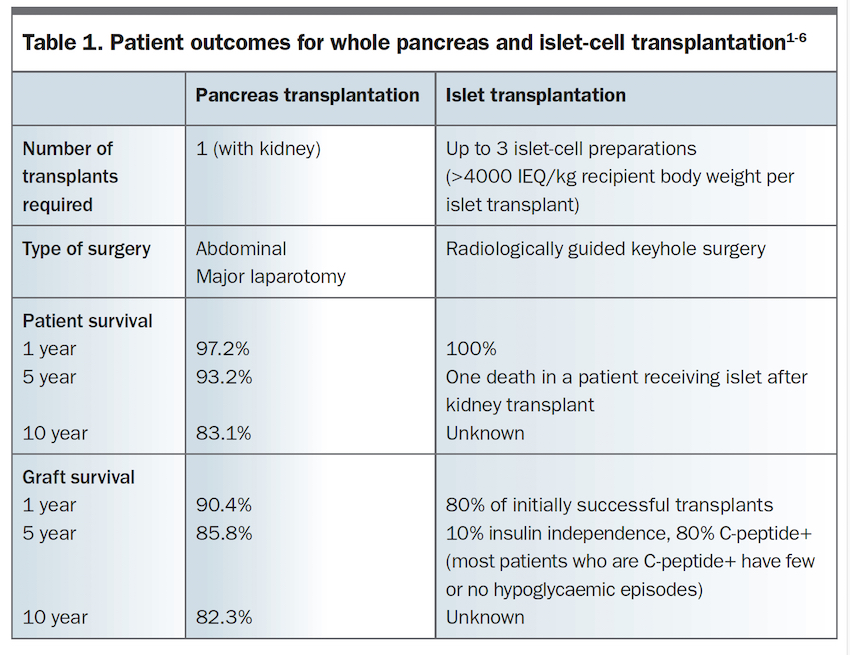
Type 1 diabetes is a life-long condition that has increased risk of microvascular and macrovascular complications. Pancreas transplantation offers superior long-term control of blood glucose levels (BGL) by replacing the beta-cells lost in type 1 diabetes and is usually performed together with kidney transplantation. This therapy, called simultaneous kidney-pancreas transplantation (SKPT), offers both cure of diabetes and renal replacement therapy, with potential for an insulin- and dialysis-free life for patients. It can result in greatly improved quality of life, decreased acute and chronic complications associated with type 1 diabetes and kidney disease, and better long-term function of transplanted kidneys. In addition, patient life span and kidney-graft survival are extended and diabetes complications usually cease to progress, or may even improve slowly (Table 1).1-6 Pancreas transplantation has been traditionally offered only to patients with type 1 diabetes; however, SKPT has been performed in highly-selected, insulin-sensitive people with type 2 diabetes, with good outcomes.7,8
{kind=link}
In Australia and New Zealand, pancreas transplant numbers (99% SKPT) have increased over time.1-5 Patient survival is excellent; for those transplanted during or after 2010, one-year survival is greater than 97% and five-year survival is 93.2%.1,2 For comparison, the Australia and New Zealand Dialysis and Transplant Registry reports show people with kidney transplants over the same timeframe had a one-year mortality rate of 3% and five-year mortality of 9 to 11%.6 These figures, however, are likely underestimated as they include people without diabetes whose outcomes are usually significantly better. People requiring dialysis had mortality rates of 15.5 to 16.2 per 100 person years, which is over seven times higher than seen in transplant recipients.
Since 2000, islet-cell transplantation has been an alternative beta-cell replacement therapy available to select patients with type 1 diabetes with good kidney function who are particularly difficult to treat using conventional insulin replacement therapies due to their severe hypoglycaemic unawareness. Because in islet-cell transplantation only the islets of Langerhans are given, they can be infused into the liver, and the procedure is much less invasive than SKPT.
The Collaborative Islet Transplant Registry is a global group that influences clinical islet-cell transplant programs on a global level. The Registry has helped to standardise clinical islet-cell transplant programs, and success rates are improving with time. Selection of suitable donors and improvements in surgical technique and immunosuppression are contributing factors to the increasing success rates. Five-year islet-recipient survival is approaching 100% as there appears to be only one reported death.9 This contrasts quite markedly with the more than 3% mortality rate in people with severe hypoglycaemic unawareness referred for consideration of islet-cell transplantation, despite their relatively young age.10 The outcome data are summarised in Table 1.
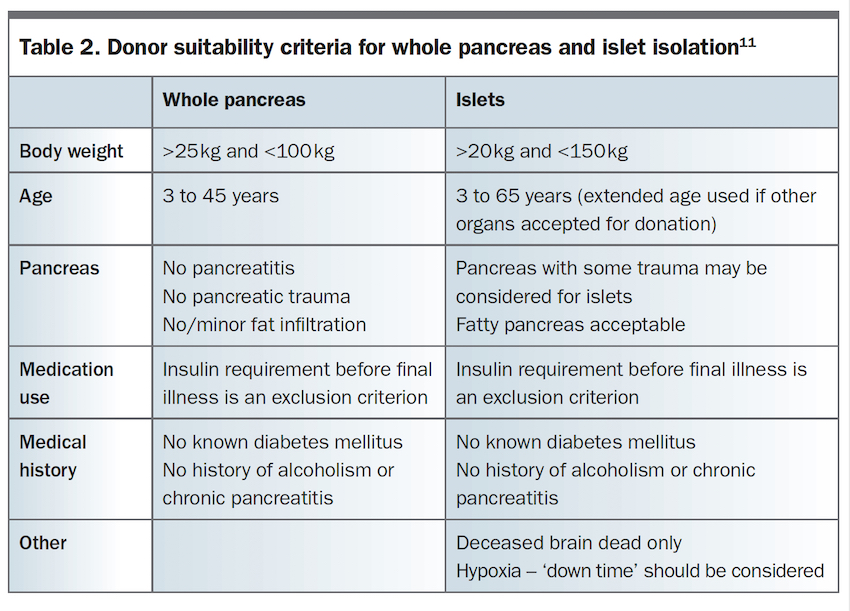
The current donor and recipient eligibility criteria guidelines in Australia for pancreas and islets are available in the Transplantation Society of Australia and New Zealand clinical guidelines and are summarised in Table 2 and Table 3.11 Careful donor selection for both pancreas and islet-cell transplantation is partly responsible for the improved outcomes over time. However, although donor organ availability is a major limiting factor for both whole pancreas and islet-cell transplantation, it is important to note that a wider range of both donors and recipients are suitable for islet-cell transplantation. Patient suitability to whole pancreas or islet-call transplantation is outlined in the Flowchart.
{kind=link}
{kind=link}
The growing need for donor organs and established standardised protocols for the use of pancreas transplantation is being increasingly recognised and was addressed in 2019 at the First World Consensus Conference on Pancreas Transplantation in Pisa, Italy. This conference was held to delineate some global guidelines for the use and allocation of organs, pancreas transplantation surgery and patient follow up after surgery.
Organ allocation
Organ compatibility
There are four main considerations in the allocation of any organ: blood group (ABO) compatibility, crossmatching, presence of donor specific antibodies (which can increase the risk of graft failure) and minimal variation in human leukocyte antigen between the donor and recipient. Currently, most transplant centres require all four considerations to be met for most recipients before an organ is allocated for transplant. Anecdotal evidence from the few ABO incompatible transplants suggests outcomes are similar to ABO compatible transplants. Positive T-cell and/or B-cell complement dependent cytotoxic crossmatch and significant human leukocyte antigen mismatching result in worse outcomes with more acute cellular rejection and/or antibody mediated rejection.12,13
Recipient factors
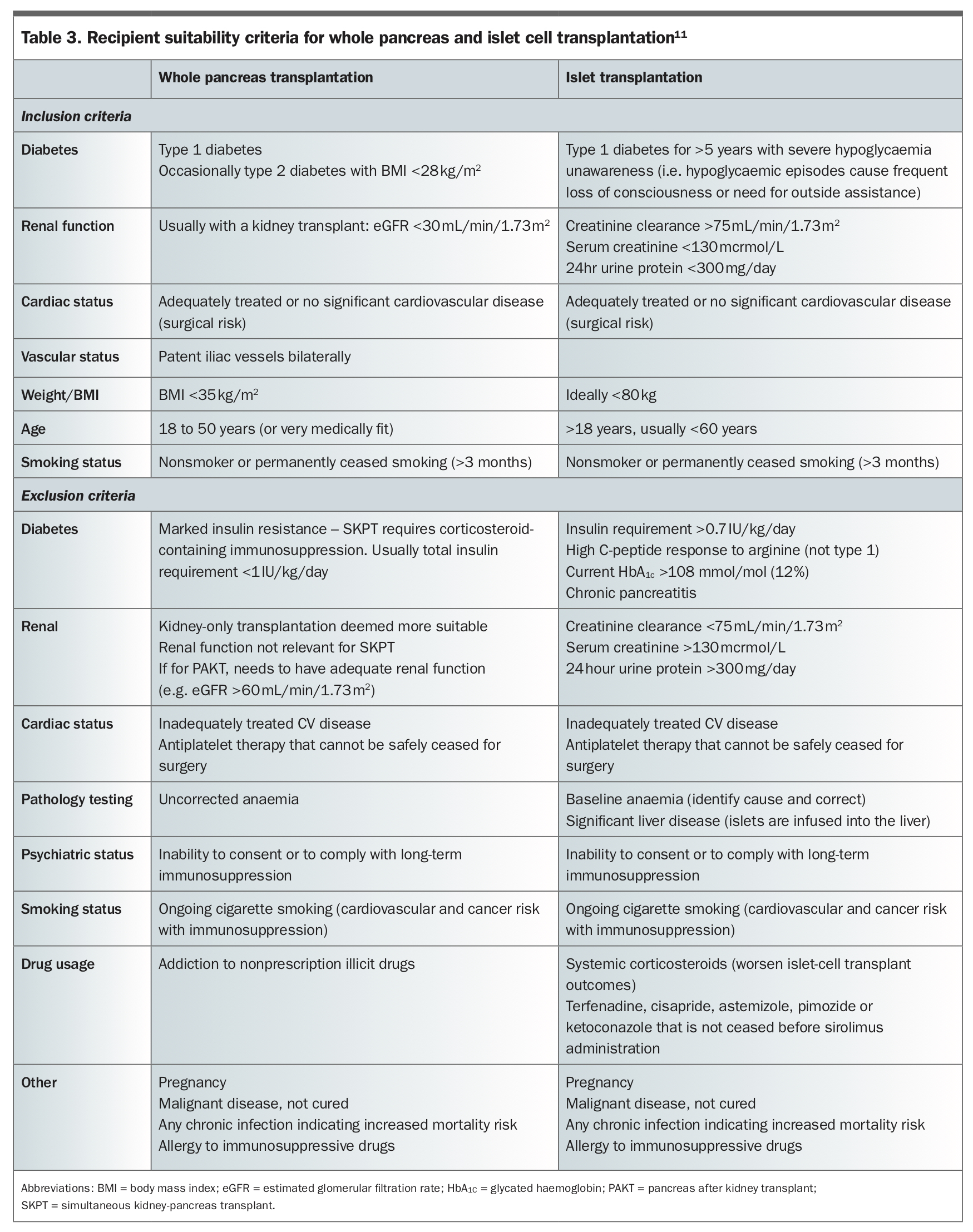
Recipient eligibility is critical to the undertaking of any organ transplant. Increasing age, obesity and number of comorbidities increase the risks for potential transplant recipients. The recipient eligibility and exclusion criteria for whole pancreas and islet-cell transplantation are summarised in Table 3. SKPT is a major abdominal surgical procedure and patient eligibility should be assessed accordingly. It is important to note that some of the exclusion criteria are treatable, and the patient may be reconsidered after treatment, for example, after correction of cardiovascular disease or after smoking cessation.
Surgery
Although pancreas surgery has improved significantly in recent years, pancreas transplantation is major surgery with a moderate surgical complication rate compared with other transplants.14 Consequently, there is a significant increase in mortality in the first few months after SKPT, but by one year, transplant recipients have lower overall mortality, which continues to improve.
Pancreas transplant after kidney transplant (or PAKT) is not commonly performed in Australia. Retrospective SKPT and PAKT data suggest that PAKT is associated with better kidney function compared with that in people who receive only a kidney.15 Worldwide, preference is given to performing an SKPT over PAKT because PAKT requires two separate surgical procedures and there is increased risk associated with rejection of kidney and pancreas allografts from two separate donors.16
Islet-cell transplantation continues to show improvements in long-term outcomes for patients, with a five-year insulin independence approaching 70% in some transplant centres. Islets are currently transplanted into the recipient’s liver via the portal vein. Surgical and radiological advances in recent years have seen a shift from performing minor abdominal surgery to using radiologically guided keyhole surgery for this transplant, reducing the risk of surgical complications and decreasing recovery time for the patient.17
Immunology and immunosuppression
Pancreas transplantation is highly immunogenic, which is likely enhanced by the heightened immune response of the recipient due to their diabetic autoimmunity.18 It is not safe to monitor grafts by repeat biopsy. However, because kidney grafts are monitored by biopsy and less invasively by blood tests and urinalysis, having an SKPT allows easier monitoring of immune rejection, which in most recipients appears consistent for two organs from the same donor.
In addition, advances in and refinement of immunosuppressive regimens have been tailored to support the pancreas, with the preference towards the use of the non-nephrotoxic and nondiabetogenic induction drugs thymoglobulin, alemtuzumab or basiliximab followed by a combination of tacrolimus and mycophenolate for maintenance.19 This has also improved graft survival for islet-cell transplantation and the side-effect profiles for recipients.16,20 Together, the development of surgical techniques and the improvements in the use of immunosuppressant agents correlates to better patient outcomes.
Islet-cell transplant recipients receive steroid-free immunosuppression, and a number of current trials are running worldwide to test new regimens for improved outcomes and side-effect profiles. As with all transplantation therapies, the burden of immunosuppression on the patient must be considered before acceptance for transplantation.
Australia and New Zealand transplant centres
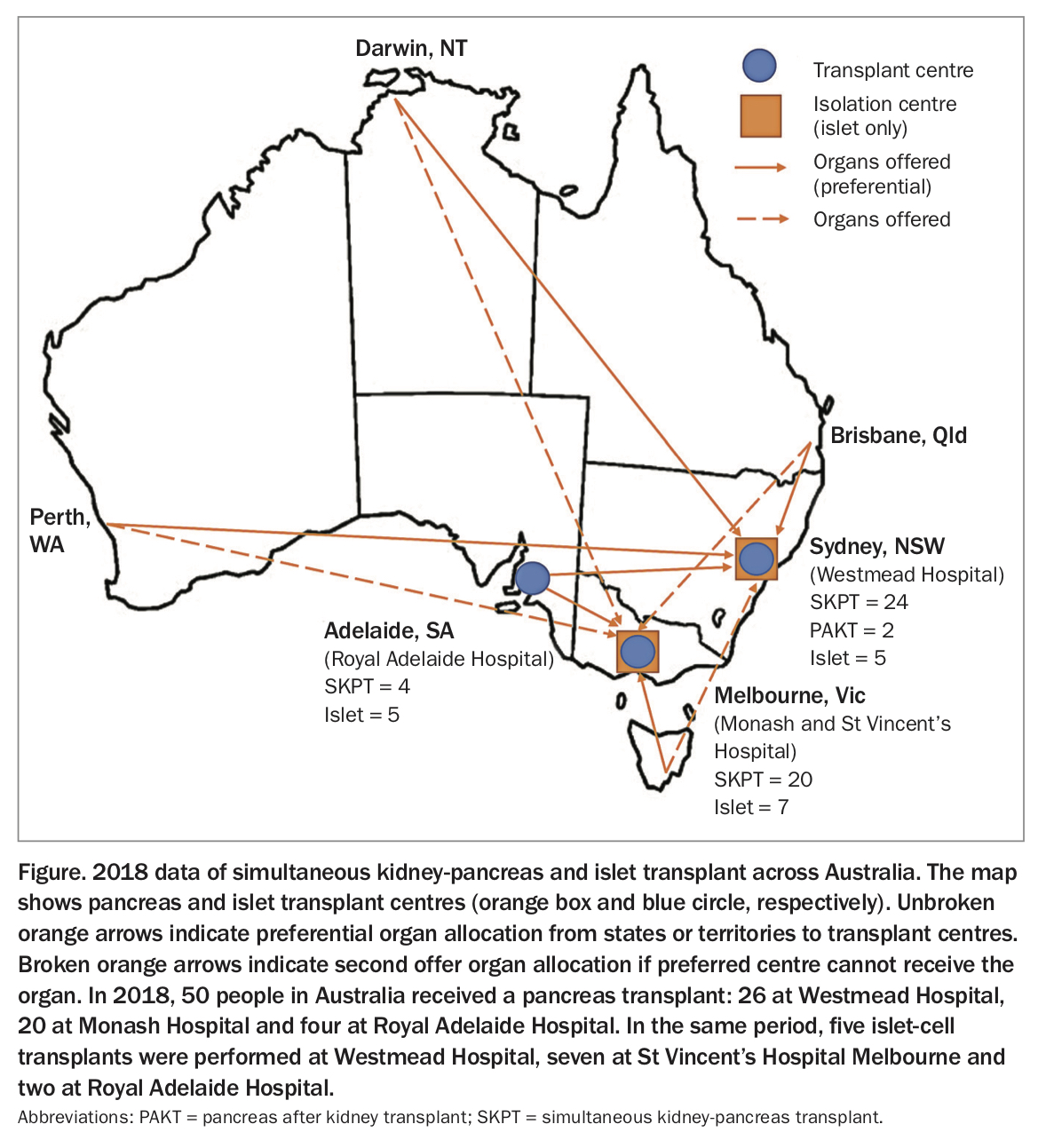
Whole pancreas transplants are performed at Westmead Hospital, New South Wales; Monash Hospital, Victoria, The Royal Adelaide Hospital, South Australia, and in New Zealand. Islets are isolated and transplanted at Westmead Hospital and as part of the Tom Mandel Islet Transplant Program at St Vincent’s Hospital Melbourne, Victoria, and are also transplanted at the Royal Adelaide Hospital. These Australian centres each accept out-of-area referrals, including from interstate where the state or territory does not have that particular transplant service, as illustrated in the Figure. If potentially suitable patients with diabetes are interested in pancreas or islet-cell transplantation and are capable of providing informed consent and of taking regular immunosuppression to maintain the transplant (Flowchart), we recommend referring them to the relevant centre for assessment.
{kind=link}
Conclusion
The number of pancreas and islet-cell transplants in Australia and New Zealand have increased over the past decade with excellent patient survival rates, and quality of life after successful pancreas or islet-cell transplantation is markedly improved for recipients. Suitability criteria for each transplant differ and these, along with long-term immunosuppression side effects, should be taken into consideration in patients who may be considering or suitable for such surgery. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.