Managing people with diabetes during Ramadan

Diabetes type 1
Diabetes type 2
Fasting in people with diabetes can disrupt glucose homeostasis, and drug regimens often require modification to prevent complications such as hypoglycaemia and hyperglycaemia.
Diabetes is one of the most important public health challenges in the 21st century. Globally, the number of people with diabetes has doubled over the past 20 years rising to more than 400 million in 2015.1 Fasting during Ramadan is one of the five pillars of Islam, and all healthy adult Muslims are obliged to refrain from eating and drinking from sunrise to sunset during this lunar month. Although exemptions from fasting exist for people with serious medical conditions, including diabetes, many still choose to fast. Fasting in people with diabetes can cause disruption of normal glucose homeostasis and lead to hypoglycaemia, hyperglycaemia, diabetic ketoacidosis, dehydration and thrombosis. This article discusses the most common acute presentations of people with diabetes who fast during Ramadan with two clinical case scenarios.
Case 1
Ali is a 57-year-old man who has had type 2 diabetes for the past 20 years. He has taken a premixed insulin (aspart 30% and aspart protamine 70%) 20 units at breakfast and 20 units at dinner for the past five years. He also takes a slow-release preparation of metformin 2 g daily and gliclazide 60 mg daily. He is a regular patient at your clinic and today he visits you for follow up about his blood glucose control. His last HbA1c measurement six months ago was 5.4% (36 mmol/mol). During the consultation, you notice Ali is sweating profusely with shaky hands. His pulse rate is 112 beats per minute. He admits that he is fasting for Ramadan and had his last meal at 4 am that morning before sunrise; it is now 5 pm. He took his usual dose of insulin 20 units at the sunset meal (iftar) and 20 units at the sunrise meal (suhoor).
What should you do first in this situation?
{kind=link}
How can Ali prevent subsequent hypoglycaemic episodes over the next 24 hours and beyond?
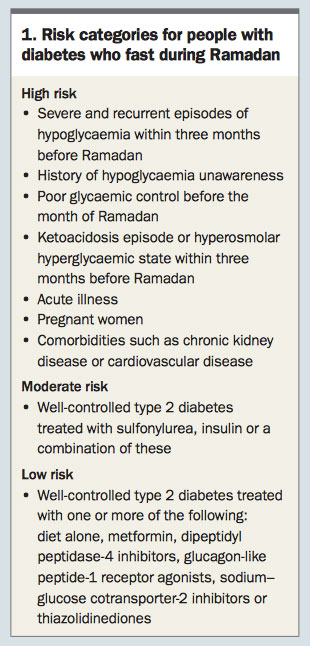
In future, Ali should be encouraged to frequently monitor his capillary BGLs during fasting hours and to break his fast whenever his BGL falls below 3.9 mmol/L, above 16.6 mmol/L or symptoms develop. There is a misconception held by some Muslim communities that finger-prick testing during fasting hours might invalidate fasting. This needs to be clarified and the patient assured that finger-prick testing does not interfere with fasting.3 Patients at high risk of hypoglycaemia should be actively discouraged from fasting (Box 1).4
Ali understands your concerns but says that he wants to fast for the remaining days of Ramadan.
What further modifications in Ali’s medications should be carried out to avoid another hypoglycaemic event?
Ali asks you about exercising during Ramadan and how he should alter his diet. What do you recommend?
What is the best type or regimen of insulin for use in people during Ramadan that is associated with a lower risk of hypoglycaemia?
Case 2
Mona, a 19-year-old woman, was diagnosed with type 1 diabetes at the age of 15 years. She presents to your general practice with insidious onset of polyuria and polydipsia associated with malaise, nausea and vomiting for the past five hours. She complains of diffuse abdominal pain and loss of appetite. Her usual medication includes glargine 24 units at night with lispro 6 units before each meal. On further questioning, she admits that she is currently fasting for the month of Ramadan. Due to the change in her dietary habits, she deliberately reduced her dose of glargine to 12 units and took lispro only before iftar thinking that she needed less insulin during Ramadan. On examination, she looks ill with dry skin and laboured breathing.
What other signs would you look for on examination?
What are the immediate tests that you should order?
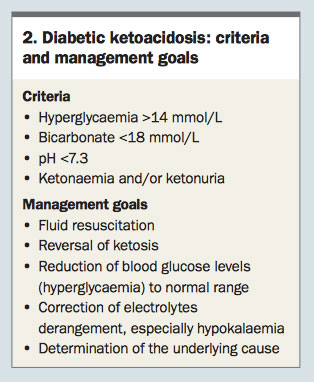
What are the criteria for diagnosis of DKA?
{kind=link}
How should Mona be managed in hospital?
After resolution of DKA, what should you advise Mona in case she wanted to continue fasting for the rest of Ramadan?
Summary
Islamic rules exempt Muslims who are sick from fasting during Ramadan. People with an acute illness such as flu can postpone fasting to other days when their illness is resolved. People with chronic illness, such as diabetes, chronic kidney disease or heart disease, and the elderly are not obliged to fast but are able to compensate by donating to a charity as atonement. Fasting for Ramadan is safe in people with diabetes at low or moderate risk of developing acute complications such as hypoglycaemia or hyperglycaemia. Patients who choose to fast should be warned of the serious consequences of complications such as hypoglycaemia and hyperglycaemia. They should also be educated before Ramadan on suitable exercise and dietary modifications. Drug modification is necessary to suit the dietary restriction during the daytime. Patients should be advised to break their fast early if they are feeling unwell and should be encouraged to monitor their BGLs more frequently while fasting. GPs should be familiar with these issues and offer appropriate advice to patients given the high number of people with diabetes in Australia who participate in the Ramadan fast. Finally, a post Ramadan GP follow up is recommended.ET
References
-
World Health Organization (WHO). Global report on diabetes WHO Geneva. Geneva: WHO Press; 2016.
-
American Diabetes Association Standards of Medical Care in Diabetes–2010. Diabetes Care 2010; 33(Supp 1): S11-S61.
-
International Diabetes Federation and the DAR International Alliance. Diabetes and Ramadan: practical guidelines. Brussels, Belgium: International Diabetes Federation; 2016. Available online at:
-
www.idf.org/guidelines/diabetes-in-ramadan and www.daralliance.org (accessed March 2017).
-
Hui E, Bravis V, Hassanein M, et al. Management of people with diabetes wanting to fast during Ramadan. BMJ 2010; 340: c3053.
-
Pathan MF, Sahay RK, Zargar AH, et al. South Asian Consensus Guideline: use of insulin in diabetes during Ramadan. Indian J Endocrinolo Metab 2012; 16: 499-502.
-
Savage M, Dhatariya K, Kilvert A, et al. Joint British Diabetes Societies guideline for the management of diabetic ketoacidosis. Diabetic Med 2011; 28: 508-515.
COMPETING INTERESTS: None.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.