Chronic kidney disease and type 2 diabetes: a guide to screening, diagnosis and slowing progression

Kidney diseases
Diabetes type 2
It is important to screen for, diagnose and aggressively manage chronic kidney disease in people with type 2 diabetes because diabetic kidney disease is a major cause of morbidity and mortality. Progression of diabetic kidney disease can be delayed and prevented by aiming for tight glycaemic control and by using blockers of the renin-angiotensin system and, if appropriate, sodium-glucose cotransporter 2 inhibitors. It is also important to aggressively address cardiovascular risk factors.
- Diabetic kidney disease (DKD) can be screened for by measuring the albumin to creatinine ratio in an early morning spot urine collection and by measuring the serum creatinine level to allow for estimation of glomerular filtration rate.
- Yearly screening for DKD should commence in patients at the time of their diagnosis of type 2 diabetes.
- A diagnosis of DKD should be made if repeat testing confirms an elevated albumin to creatinine ratio (>2.5 mg/mmol in men or >3.5 mg/mmol in women) and/or the estimated glomerular filtration rate is less than 60 mL/min/1.73m2.
- Progression of DKD can be delayed by aiming for good glycaemic (general HbA1c target <7% or 53 mmol/mol) and blood pressure (general target <140/90 mmHg) control. A tighter blood pressure target of less than 130/80 mmHg may be appropriate in patients with macroalbuminuria (proteinuria).
- Blockers of the renin-angiotensin system at maximally tolerated doses and, if appropriate, sodium-glucose cotransporter-2 inhibitors can be used to slow the progression of DKD.
- Cardiovascular risk factors should be treated aggressively in patients with DKD.
Chronic kidney disease (CKD) in people with type 2 diabetes is a heterogeneous group of disorders. The development and progression of CKD is usually driven by hyperglycaemia and the associated metabolic disorders of diabetes. However, it is also important to exclude nondiabetic kidney disease in patients with diabetes, especially in the absence of diabetic retinopathy, if there is a short duration of diabetes and in the presence of clinical features to suggest glomerulonephritis. CKD in patients with diabetes has traditionally been referred to as diabetic nephropathy but this is a term that should be reserved for people with progressive albuminuria. There is now growing appreciation that renal impairment can develop in patients with diabetes in the absence of increasing albuminuria and any other nondiabetes-related causes of CKD. The term diabetic kidney disease (DKD) is therefore now preferred to describe the presence of CKD in patients with diabetes.1
It is important to screen for, diagnose and aggressively manage CKD in patients with type 2 diabetes as DKD is a major cause of morbidity and mortality. It not only remains the leading cause of end stage kidney disease (ESKD) in Australia but is also a major risk factor for the development of cardiovascular disease.1-3 Despite this, the progression of DKD can be significantly delayed in people with type 2 diabetes with good metabolic control and the use of blockers of the renin-angiotensin system (RAS) and sodium-glucose cotransporter-2 (SGLT-2) inhibitors.
Screening and staging of diabetic kidney disease
Screening for DKD entails measuring the albumin to creatinine ratio (ACR) in an early morning spot urine collection and measuring serum creatinine levels to allow for estimation of glomerular filtration rate (eGFR). Yearly screening for DKD should commence in patients when they are diagnosed with type 2 diabetes. A diagnosis of DKD should only be made if repeat testing confirms an elevated ACR (>2.5 mg/mmol in men or >3.5 mg/mmol in women) and/or the eGFR is less than 60 mL/min/1.73 m2. It should also be appreciated that the urinary ACR has an individual coefficient of variation of 30 to 40%, so if an abnormal ACR value is found, one or more tests should be performed over the next three months. At least two out of three measurements should be abnormal before making a diagnosis of persistent microalbuminuria.
Albuminuria may fluctuate with factors that have no causal relation to the development of DKD. These factors may include concurrent urinary tract infections and febrile illnesses, exercise, drugs, weight fluctuations, uncontrolled hypertension and the presence of cardiovascular disease. As the definition of CKD entails the presence of persistent markers of kidney damage (for at least three months), a repeat eGFR should also be obtained to confirm the presence of DKD. A persistent value of less than 60 mL/min/1.73 m2 in the absence of albuminuria suggests the diagnosis of DKD if nondiabetes-related causes of CKD are excluded, as discussed below.
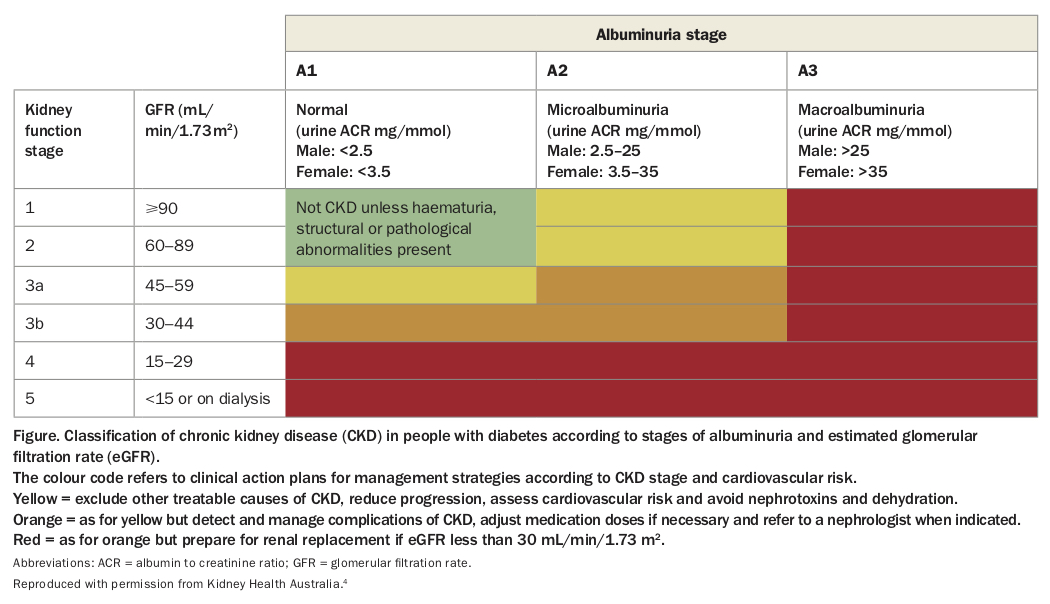
Using the ACR and eGFR results in a person with diabetes, clinicians are encouraged to stage DKD using a two-dimensional composite ranking system (the so-called heat map) based on renal and cardiovascular risk (Figure).4 Most guidelines now actively discourage the use of the term microalbuminuria and instead suggest assigning albuminuria to three categories. These categories are: A1, normal to mildly elevated; A2, moderately increased (instead of microalbuminuria); and A3, severely increased (instead of macroalbuminuria or proteinuria). GFR is generally divided into five categories with a subdivision of stage 3 into stages 3a and 3b to reflect the increased risk for cardiovascular disease that has been reported when eGFR declines below 45 mL/min/1.73 m2.2,4,5
{kind=link}
Other causes of kidney disease in patients with diabetes
Kidney disease in a patient with diabetes may not always be due to diabetes. The following factors should alert the clinician to the possibility of other aetiologies:
- absence of retinopathy
- diabetes of less than five years’ duration
- acute kidney injury rather than gradual progression to CKD
- presence of haematuria or other systemic disease
- presence of the nephrotic syndrome (albuminuria >3g, low serum albumin level, oedema and symptoms such as frothy urine).
Among these factors, absence of retinopathy and short duration of diabetes are the strongest predictors of nondiabetic kidney disease. If a nondiabetic aetiology is suspected, it is essential to exclude reversible causes of kidney disease. Investigations may include a midstream specimen of urine, renal tract ultrasound, measurement of serum autoantibodies and immunoglobulins and a renal biopsy. A medication review of potential nephrotoxins should also be performed.
Treatment of diabetic kidney disease
The aim of treatment of DKD is to delay the progression of renal disease and to reduce overall cardiovascular risk. GPs have a crucial role in this pursuit, via active monitoring and treatment of hyperglycaemia, hypertension and dyslipidaemia. Targets for treatment need to be tailored for each patient taking into account age, burden of comorbidities, life expectancy and current pharmacotherapy.
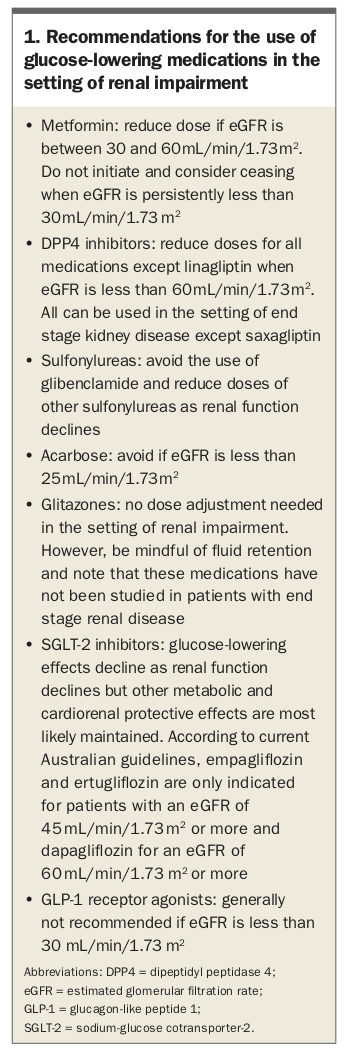
Intensive glycaemic management (HbA1c <7% or <53 mmol/mol) delays development and progression of albuminuria with recent evidence also showing that it slows the rate of GFR decline and retards progression to ESKD.6,7 However, it should be noted that many glucose-lowering medications require a dose adjustment in the setting of CKD as outlined in Box 1.8
{kind=link}
Moderate blood pressure control, aiming for a general target of less than 140/90 mmHg is associated with a slowing of progression of DKD. However, more aggressive blood pressure control (<130/80 mmHg) may be appropriate in some patients, especially in those with macroalbuminuria/proteinuria, provided they can be achieved without significant side effects of treatment.8
RAS blockers such as angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs) are recommended as first-line therapy for patients with diabetes and either hypertension or albuminuria or both. ACE inhibitors and ARBs slow progression from normoalbuminuria to microalbuminuria in patients with hypertension; however, it still remains controversial as to whether this effect has some independence from the effect of improved blood pressure control. There is no evidence to support the use of RAS blockade for primary prevention of DKD in normotensive, normoalbuminuric patients with diabetes. To date, RAS blockers have only been shown to slow progression to ESKD in patients with macroalbuminuria/proteinuria and an eGFR of less than 60 mL/min/1.73 m2.8-10
In general, ACE inhibitor and ARBs have similar renal benefits but their combination does not offer any additional renal protection and may be harmful. The use of mineralocorticoid receptor blockers such as spironolactone or eplerenone in combination with RAS blocking agents is a useful approach to help manage resistant hypertension, to reduce proteinuria and, most likely, to offer cardiovascular protection. However, the benefits versus the risks, especially that of hyperkalaemia, of mineralocorticoid receptor blocking therapy in long-term clinical trials in patients with CKD and type 2 diabetes have not been evaluated.8
SGLT-2 inhibitors have recently been shown to offer cardiorenal protection in patients with type 2 diabetes on top of the normal standard of care including the use of RAS inhibiting agents.11-15 SGLT-2 inhibitors reduce glucose and blood pressure levels and promote uric acid excretion but their renal protective mechanisms are most likely via alterations in intrarenal haemodynamics and a reduction in intraglomerular pressure.16 Currently, empagliflozin and ertugliflozin are only indicated for patients with an eGFR of 45 mL/min/1.73 m2 or more and dapagliflozin for an eGFR of 60 mL/min/1.73 m2 or more, but it is likely that these recommendations will be reviewed in the near future.
Glucagon-like peptide 1 (GLP-1) receptor agonists and fenofibrate most likely reduce albuminuria but to date have not been shown to retard eGFR loss and progression to ESKD in dedicated trials involving patients with type 2 diabetes and CKD.17,18
Acute increases in serum creatinine levels and a subsequent decrease in eGFR are often seen in patients after the introduction of an RAS blocking agent or an SGLT-2 inhibitor, due to their reversible effects on intrarenal haemodynamics. These acute decreases in eGFR stabilise and are translated into a subsequent amelioration of renal function decline and protection from progression to ESKD. However, if the acute rise in serum creatinine level exceeds 30% after starting an RAS blocker or an SGLT-2 inhibitor, then the use of these agents should be revaluated. It is also recommended to check patients for an increase in serum potassium level after the initiation of an RAS blocker. In addition, serum creatinine levels usually temporarily rise after the introduction of fenofibrate due to a reversible effect of creatinine handling by the renal tubules.
There are no specific lipid targets in patients with diabetes and CKD. However, we would encourage the use of statins in patients with diabetes and pre-ESKD to achieve the general lipid goals as recommended by the RACGP and Diabetes Australia guidelines, General Practice Management of Type 2 diabetes.5,19 These goals are an LDL-cholesterol level of less than 2.0 mmol/L, HDL-cholesterol level of 1.0 mmol/L or more and triglyceride level of less than 2.0 mmol/L.5,19 For patients with ESKD, a reasonable approach is to continue statin therapy if the person is already taking a statin, but not to commence one de novo after commencing dialysis as the initiation of a statin in this setting has not been shown to offer cardiovascular protection. Most recent studies have not supported the use of aspirin.20
The importance or avoiding or quitting smoking to reduce the development and progression of renal and cardiac disease should be emphasised to all people with type 2 diabetes. Avoiding excess sodium intake helps to control blood pressure in patients who are hypertensive but optimal sodium intake targets still remain controversial. High dietary protein intakes (>20% of total daily calories) have been associated with high levels of albuminuria and accelerated renal function loss and therefore may best be avoided. However, it is worth nothing that long-term studies have not been conducted on the value of protein restriction on the progression of DKD.
Sick-day management
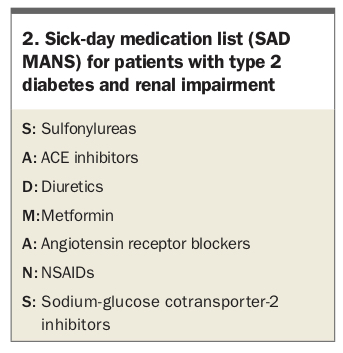
GPs can play an important role in reinforcing the principles of sick-day management, especially those related to medication use, in patients with diabetes and CKD. The acronym SAD MANS is a useful way to focus attention on medications that may have reduced clearance and an increased risk of adverse effects in patients with CKD (Box 2). Some medications need a dose adjustment or need to be withheld, especially in the setting of acute illness that can result in dehydration and acute renal failure.
{kind=link}
Most guidelines now support the use of metformin in patients with an eGFR as low as 30 mL/min/1.73 m2, although not at maximum recommended doses.21 There is also a growing appreciation of temporarily withholding SGLT-2 inhibitors if patients are unwell or need to fast for a prolonged period of time.
When to refer
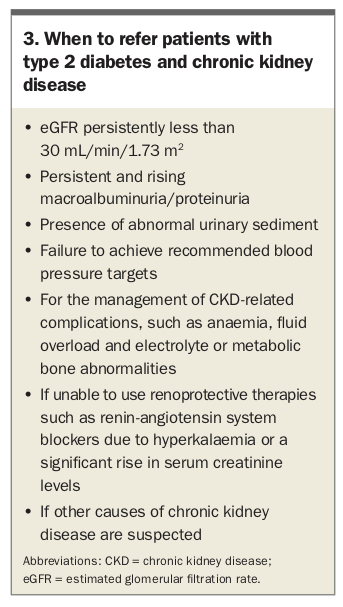
GPs are encouraged to refer patients with diabetes and CKD to an appropriate specialist if nondiabetic kidney disease is suspected, if there are difficulties managing specific complications of CKD (e.g. anaemia, fluid overload, resistant hypertension or electrolyte or metabolic bone abnormalities), if eGFR is persistently below 30 mL/min/1.73 m2, or for other situations, as summarised in Box 3.
{kind=link}
Summary
Screening people with diabetes for early markers of DKD and initiating measures to retard the progression of kidney disease are part of routine clinical practice. In addition, it is necessary to measure, assess and aggressively manage cardiovascular risk factors. Focusing on glycaemic, lipid and blood pressure management, managing lifestyle factors (such as following a healthy diet, avoiding weight gain and stopping smoking) and undertaking regular exercise still remain the cornerstone of management of patients with DKD. The use of RAS blocking agents and SGLT-2 inhibitors have also been shown to slow the progression of DKD to ESKD and provide cardiovascular protection. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.