Metabolic bone disease in people with chronic kidney disease

Dr Guo is a Renal Registrar in the Department of Nephrology, Monash Health, Melbourne. Dr Damasiewicz is a Nephrologist at Monash Health and in the Department of Medicine, Monash University, Melbourne. Dr Aleksova is an Endocrinologist at Monash Health and St Vincent’s Health and a Postdoctoral Research Fellow in the Department of Medicine, Monash University and the Metabolic Bone Research Group, Hudson Institute of Medical Research, Melbourne Vic.
Bone diseases
Kidney diseases
Patients with chronic kidney disease (CKD) have an increased risk of fracture compared with the general population, which is associated with increased morbidity and mortality. Multidisciplinary and individualised treatment is required based on clinical, biochemical and imaging parameters to optimise bone health in these patients.
- Fractures in patients with chronic kidney disease (CKD) are common compared with age-matched cohorts without CKD and are associated with greater morbidity and mortality. Risk factors for fractures include those present in the general population and those specific to patients with CKD.
- Fracture risk assessment remains challenging. Diagnostic tools include imaging techniques to evaluate altered bone mass or microarchitecture, biochemistry and histomorphometry to evaluate the underlying bone turnover state.
- Management of bone health in patients with CKD includes nonpharmacological strategies, correction of the underlying biochemical disturbances associated with CKD mineral and bone disorder and consideration of use of antiosteoporosis therapies.
- Patients who require antiosteoporosis therapies need to undergo specialist management, including individualised assessment of fracture risk, bone turnover, renal function, comorbidities and potential medication adverse reactions.
Patients with chronic kidney disease (CKD) stages 3 to 5D have an increased risk of fracture, driven by mineral metabolism derangements and skeletal abnormalities, which are described by the Kidney Disease Improving Global Outcomes (KDIGO) organisation as CKD mineral and bone disorder (CKD-MBD). Patients with CKD also have concurrent risk factors for age-related osteoporosis. Both CKD-MBD and osteoporosis reduce bone mass and alter bone quality, resulting in up to a 20-fold increase in fractures compared with age-matched patients without CKD, and are associated with a high morbidity and mortality.1,2
Histopathological classification of bone changes associated with CKD-MBD, which are collectively termed renal osteodystrophy, focus on the assessment of bone turnover, volume and mineralisation. Although these changes occur with overlapping pathologies, they are broadly divided into high and low bone turnover states but occur parallel to those related to osteoporosis.
New evidence supporting noninvasive techniques to assess bone mass and quality, as well as increased, off-label use of antiosteoporosis therapies in patients with CKD stages 3 to 5D, have provided important new data guiding clinical practice. This article discusses the challenges in the management of bone health in people with CKD-MBD, providing important updates from recent guidelines.
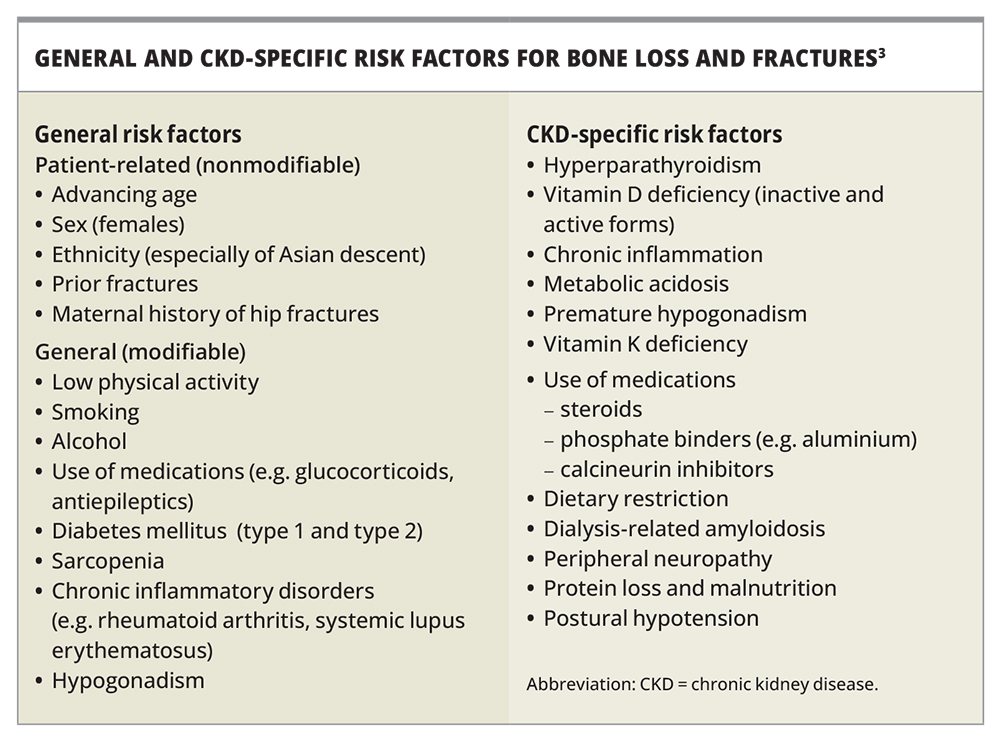
Pathophysiology and risk factors for bone fragility in patients with CKD
Patients with CKD have risk factors in addition to those for osteoporosis that further increase their risk of fracture (Box).3 The mineral derangements are complex and progress with declining renal function. Phosphate retention occurs early with nephron dropout, stimulating fibroblast growth factor-23 (FGF-23), derived from osteocytes, to promote renal excretion of phosphate, and thus maintain serum phosphate. This homeostatic mechanism initially normalises serum phosphate levels but consequently results in reduced calcitriol synthesis and hence reduced gastrointestinal absorption of dietary calcium and phosphorus, resulting in hypocalcaemia.4,5 Secondary hyperparathyroidism ensues to combat these disturbances but, if untreated, the parathyroid glands may become autonomous from constant stimulation, leading to maladaptive tertiary hyperparathyroidism with simultaneous hyperphosphatemia, further elevations in FGF-23 levels and calcitriol deficiency.4-7
{kind=link}
These mineral aberrancies stimulate abnormalities in bone and mineral metabolism, which impact bone turnover, mineralisation and volume. High bone turnover states are predominantly seen in patients with predialysis CKD with significantly elevated parathyroid hormone (PTH) levels, whereas those with low bone turnover disease (adynamic bone disease and osteomalacia) can have more variable PTH and bone turnover values. However, both high and low bone turnover can occur across all stages of CKD and the underlying bone histology can change with CKD progression.8,9 Both high and low turnover states lead to an increased risk of fracture in people with CKD, likely owing to the disruption of the bone mineral matrix and microarchitecture, with cortical bone integrity the predominant defect observed in these patients.10,11
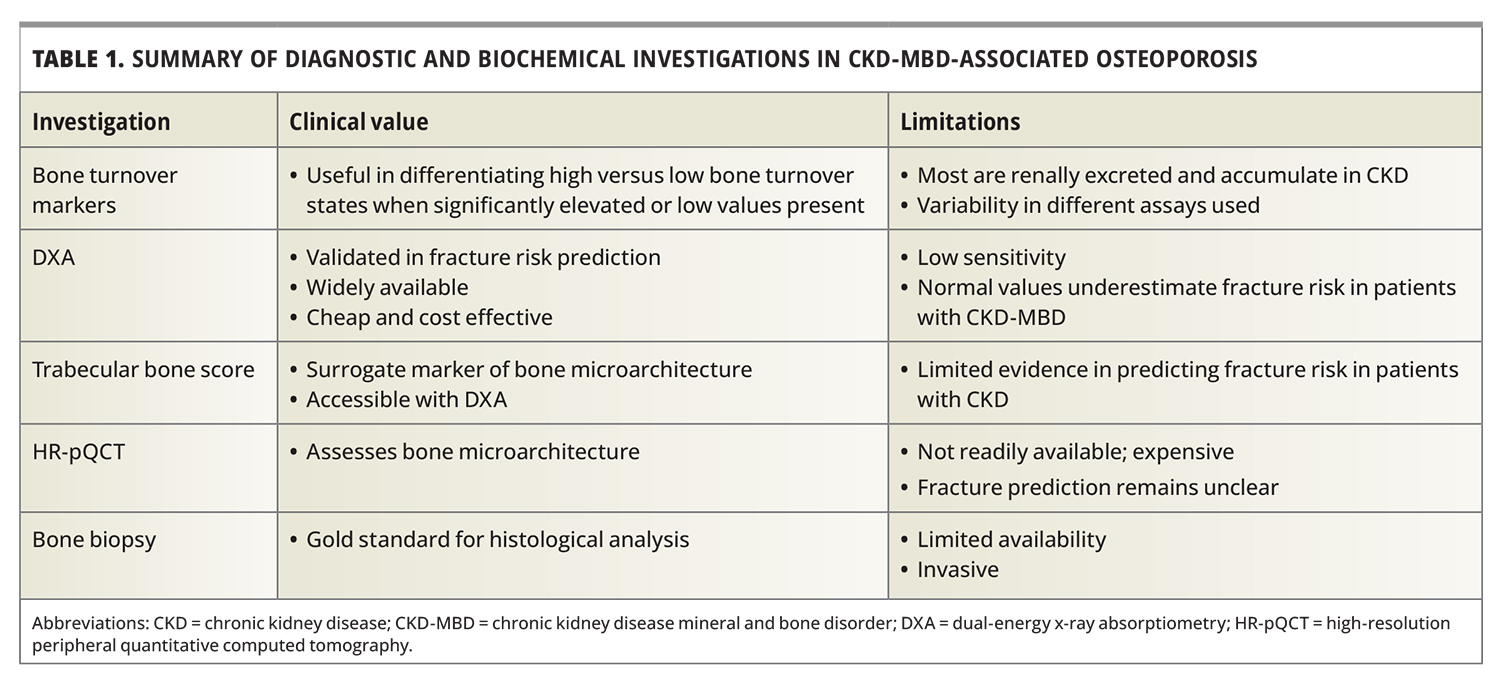
Assessment of fracture risk and bone turnover
There are multiple noninvasive diagnostic techniques to assess bone mineral density (BMD) and bone quality (Table 1).
{kind=link}
Fracture risk assessment
The measurement of BMD by dual-energy x-ray absorptiometry (DXA) is used to stratify fracture risk in patients without CKD, in which osteoporosis is defined as 2.5 standard deviations or more below the young adult mean value (T-score ≤−2.5).12 Historically, DXA has not been recommended for patients with CKD as it has typically underestimated fracture risk, with the disparity between BMD and fracture risk reflected by altered bone quality not captured by the two-dimensional area assessment of bone mass.13,14 Concerns about vascular calcification, which is highly prevalent in patients with CKD, have also hindered its acceptance.15
Reduced BMD and osteoporotic T-scores have been shown to predict fracture risk in patients with CKD similar to those without CKD.16-18 This has led to updated KDIGO recommendations endorsing the use of DXA in patients with CKD stages 3 to 5D if the result will inform treatment decisions.19 However, the diagnostic implications of normal T-scores in patients with known CKD-MBD remains uncertain, as they do not necessarily signify normal bone architecture, strength or a lower fracture risk.
The Fracture Risk Assessment (FRAX) tool uses ten clinical risk factors for fracture risk, with or without BMD measurement, to provide a ten-year absolute risk of osteoporotic fractures. It has recently been validated for fracture risk in patients with nondialysis and dialysis-dependent CKD, with some studies showing improved fracture prediction over BMD alone. However, others show no such additional benefit to performing a DXA alone, especially in those with stages 4 to 5D CKD.20-23
The trabecular bone score is a grey-level analytical tool retrospectively applied to spinal DXA images, providing a surrogate measure of microarchitectural deterioration. It demonstrates fracture prediction in the general population and some preliminary studies have shown its utility in CKD-MBD.24-26 Trabecular bone score is usually low in patients with CKD, including patients on dialysis. It correlates better with incidence of fracture in predialysis CKD, patients on dialysis and kidney transplant recipients compared with BMD.27,28
High-resolution peripheral quantitative computed tomography (HR-pQCT) of the tibia and radius, and MRI, can differentiate between cortical and trabecular bone, demonstrate microarchitectural deterioration and provide noninvasive insights into bone fragility.29,30 HR-pQCT provides more detailed information about bone microstructure than conventional spinal and hip DXA and QCT, which do not detect trabecular thickness or cortical porosity. Studies using HR-pQCT have shown a preferential loss of cortical bone in patients with CKD. In CKD stages 2 to 4, before the onset of secondary hyperparathyroidism, impairment of trabecular bone is noted with HR-pQCT, and may explain the increased risk of fractures in early CKD.31 As CKD progresses with increased bone turnover, bone loss assessed by HR-pQCT is predominantly cortical and is highly associated with fractures in weight-bearing and nonweight-bearing sites. However, its use in clinical practice is currently limited by availability and costs.
Bone turnover assessment
Identification of high versus low bone turnover states is essential before use of specific antiosteoporosis therapies; however, this remains diagnostically challenging. Bone biopsy remains the gold-standard investigation to diagnose the underlying bone disease in CKD-MBD and provides information relating to bone turnover, volume and mineralisation. Previously, indications for performing a bone biopsy in patients with CKD included unexplained bone pain, atypical fractures and to exclude mineralisation abnormalities due to aluminium or iron toxicity. However, in clinical practice it is now predominantly performed to determine the underlying bone turnover type before considering specific antiosteoporosis therapies. Bone histomorphometry is mainly used in research, given its limited availability and invasiveness.32
Bone turnover markers provide an indication of the bone resorption and bone formation rate. They provide an integrated dynamic assessment of skeletal metabolism and facilitate management of renal osteodystrophy. Despite limitations, bone turnover markers may be used as an adjunct in defining bone turnover states in CKD. High PTH values (31.8 pmol/L [>300 pg/mL]) in conjunction with elevated bone-specific alkaline phosphatase levels provides the greatest discriminatory values for high bone turnover states.33 Low PTH values (<15.9 pmol/L [150 pg/mL]) are more likely found in adynamic bone disease, although significant overlap exists between these values.19,34 Furthermore, various PTH assays are available, and clinicians should aim for serial measurements within the same laboratory and assay when assessing bone turnover.35,36
Additional biomarkers of bone resorption include collagen type 1 crosslinked C-telopeptide (CTX), a breakdown product of type 1 collagen used in the formation of bone matrix, and tartrate resistant acid phosphatase (TRAP) 5b, an osteoclast derived enzyme. CTX is renally excreted and hence accumulates in CKD, with its elevation misleadingly suggestive of high bone turnover states. TRAP5b is not renally cleared and has shown greater accuracy for assessment of bone turnover but its measurement by immunoassay is currently not available for clinical settings.37,38
Procollagen type 1 N-terminal propeptide, an osteoblast-derived peptide, is a marker of bone formation. Although metabolised by the liver into monomeric and trimeric forms, the monomeric forms are renally excreted and hence may accumulate disproportionately when renal function is impaired.37,39
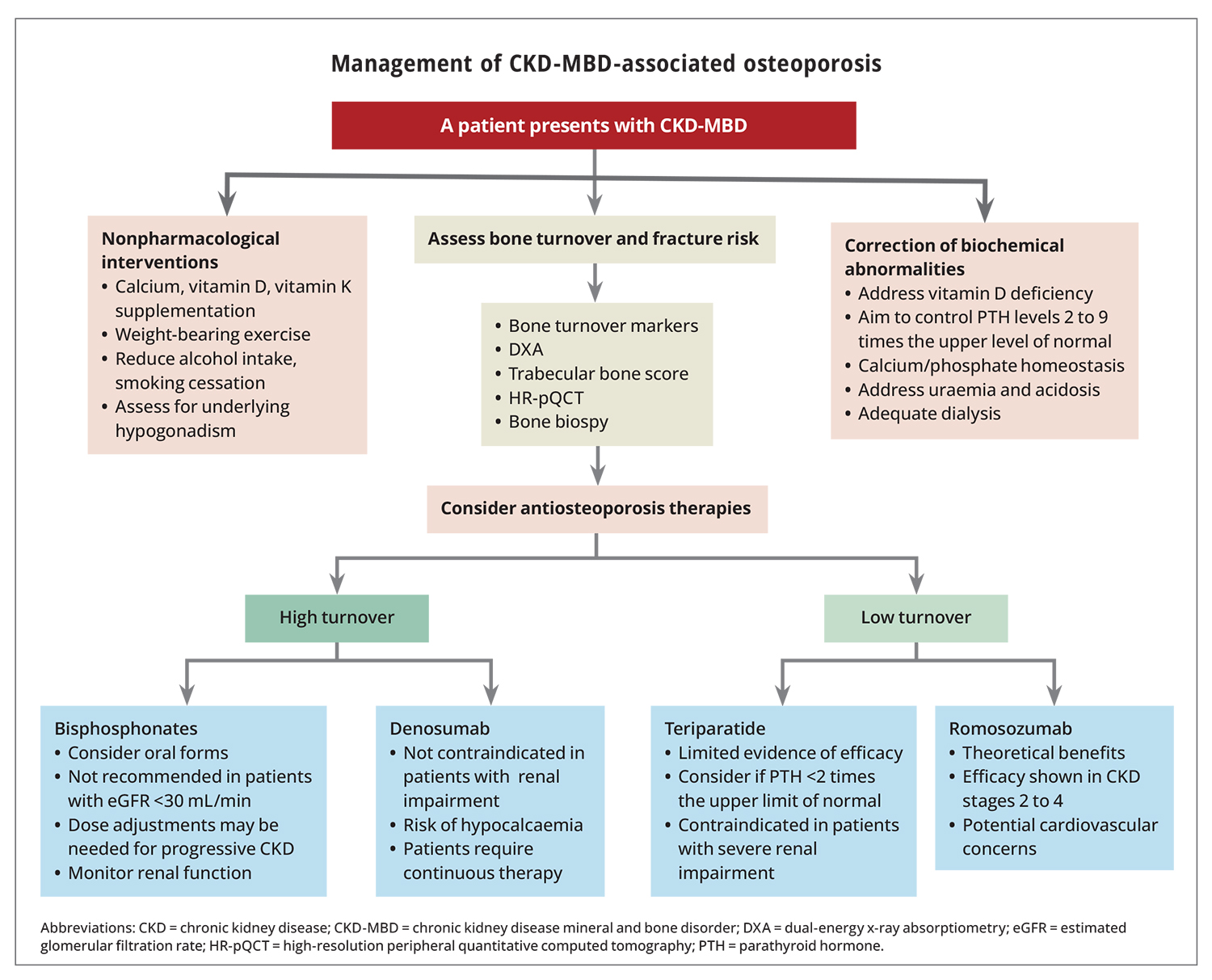
Management of CKD-MBD-associated osteoporosis
Management of CKD-MBD-associated osteoporosis requires a multifaceted approach based on nonpharmacological interventions, correction of biochemical abnormalities of CKD-MBD and use of specific bone-directed pharmacological agents (Flowchart).
{kind=link}
Nonpharmacological interventions
Nonpharmacological interventions applied to the general population should also be used in patients with CKD. These include strategies such as smoking cessation, avoiding excessive alcohol intake, adequate protein intake and resistance and strength exercises.12,40 Assessing underlying hypogonadism, which has been reported in 50 to 60% of all patients with CKD, should be addressed according to endocrinological guidelines.41-43
Patients with CKD are also at a higher risk of falls owing to changes in fluid status and postural hypotension, vision loss, myopathy, neuropathy, sarcopaenia and polypharmacy, and these should be managed accordingly.44,45
Correction of biochemical abnormalities underlying CKD-MBD
Correction of biochemical abnormalities underlying CKD-MBD is important in mitigating fracture risk. This should primarily address vitamin D deficiency, hyperphosphatemia and secondary hyperparathyroidism. Cholecalciferol supplementation is often used to treat vitamin D deficiency, even in patients requiring dialysis. It has been shown to potentially control PTH levels and aid in the management of secondary hyperparathyroidism.46-48 Although there is no clear consensus as to the optimal target range in patients with CKD, some international guidelines have recommended a higher target (>75 nmol/L) compared with the general population to stimulate residual renal hydroxylation and compensate for high osteoid activity.49,50
Hyperphosphatemia management should include dietary modifications to avoid consuming foods that contain high inorganic phosphate levels such as soft drinks, spreadable cheeses and packaged and frozen meals.51 Most patients also require use of phosphate binders to be taken with meals. Currently, only calcium-based phosphate binders are listed on the PBS for patients with CKD stages 5 to 5D and some data show that they reduce fracture risk across all patients with CKD, in addition to controlling serum phosphate levels.52-54
Secondary hyperparathyroidism is an important consequence of CKD-MBD, with persistent elevations of PTH associated with cortical thinning and porosity.9 There is a lack of randomised controlled trials to define an optimal clinical PHT range. As such, the KDIGO guidelines recommend controlling PTH levels at two to nine times the upper limit of normal in people on dialysis, to allow sufficient remodelling in the face of signalling resistance to PTH in uraemic bone.19,55 Assay variability necessitates the need to review trends in values and treat persistent elevations of PTH levels, rather than focusing on a single reading.19,35,36 In addition to cholecalciferol, activated vitamin D receptor analogues, such as calcitriol, may be more effective in reducing PTH levels, but their use can be limited by hypercalcaemia, and a recent meta-analysis showed no conclusive benefit in fracture reduction.48,56 Calcimimetics, such as cinacalcet, increase the sensitivity of the parathyroid glands to serum calcium levels, hence lowering PTH secretion and decreasing serum levels. However, their impact on mortality, bone health and cardiovascular outcomes remains contentious.14,56-60 Despite conflicting evidence, the updated KDIGO guidelines continue to recommend these pharmacological agents to limit secondary hyperparathyroidism.19 Conversely, over-suppression of PTH levels with use of any pharmacological agent may lead to a low bone turnover, which should also be avoided because of increased risk of fracture.61
Surgical parathyroidectomy can be considered in patients who fail to respond to pharmacotherapy. Successful parathyroidectomy has been associated with improved control of serum calcium and phosphate levels, improved BMD increments, lower fracture rates and increased survival in cohort studies.7,62,63 After parathyroidectomy, however, patients are at risk of critical hypocalcaemia and may require high doses of calcium and calcitriol supplementation.64
Antiosteoporosis therapies in patients with CKD
In CKD stages 1 to 3 with no evidence of CKD-MBD, antiosteoporosis therapies can be administered according to general osteoporosis guidelines (Table 2). There are no primary safety or fracture data in patients with CKD stages 3 to 5D with evidence of CKD-MBD and, as such, no specific recommendations for the use of these drugs in this cohort. Therefore, an individualised assessment of fracture risk and bone turnover is needed before using these agents.
{kind=link}
Bisphosphonates
Bisphosphonates are the most common antiresorptive medication used in people with osteoporosis. They bind to hydroxyapatite and interfere and reduce osteoclastic reabsorption. About 20 to 50% is renally excreted without prior metabolism, but they can be used without any major dose reductions in CKD stages 1 to 3.19 In CKD stages 4 to 5, the consideration for bisphosphonate therapy is guided by bone turnover markers to ensure treatment of a high bone turnover state.40,65
Data for bisphosphonate use in CKD stages 4 to 5D has been primarily derived from post-hoc analyses of major osteoporosis trials, in which patients did not typically have associated CKD-MBD.66,67 Nonetheless, there is increased expertise with their use in CKD stages 4 to 5D, and international guidelines recommend an individualised approach for their use, recognising that they are not recommended in patients with an estimated glomerular filtration rate (eGFR) of less than 30 mL/min/1.73m2.19,68 They should be reserved for patients with CKD with high turnover states to avoid inducing adynamic bone disease, despite no studies confirming bisphosphates exacerbate underlying low bone remodelling.69 A bone biopsy before their use may be considered but is no longer mandated.19
Aside from the general risks of bisphosphonates in patients with osteoporosis, recent evidence has shown a decline in eGFR of up to 15% with oral bisphosphonate use, thus active monitoring of renal function is required.70 Due to their renal accumulation, dose adjustments of bisphosphonates may need to be considered with progressive CKD and should be administered post-dialysis to avoid filtration in patients on dialysis.68 A typical regimen in later CKD stages may start with fortnightly dosing of oral bisphosphonates, increasing to weekly if bone turnover markers are not suppressed and renal function remains stable. There is no data relating to the long-term duration of bisphosphonate therapy and drug intermissions (holidays).
Denosumab
Denosumab is a fully humanised monoclonal antibody to the receptor activator of nuclear factor kappa-Β ligand (RANKL), which binds to endogenous RANKL, inhibiting its action and thus inhibiting the development and activity of osteoclasts. It therefore decreases bone resorption, increases bone density and reduces fracture rates.71 It undergoes hepatic metabolism with no drug accumulation with declining renal function.72
The efficacy of denosumab in CKD cohorts has been derived from post-hoc analyses of major osteoporosis trials in participants with reduced eGFR but in the absence of concurrent CKD-MBD.71,73 A recent meta-analysis suggests that denosumab may be more efficacious in improving femoral neck BMD compared with bisphosphonates in patients with CKD.74 HR-pQCT studies have also shown denosumab specifically decreases cortical bone resorption. Its use, however, has been associated with protracted hypocalcaemia, and many clinicians are now cautious about prescribing it for patients with advanced CKD.75,76
Although there is no consensus, adequate vitamin D and normal calcium levels should be ensured before the use of denosumab; ample vitamin D supplementation and serial monitoring of calcium levels may assist to reduce the development of hypocalcaemia after denosumab administration. Discontinuing denosumab in patients with CKD may lead to a rebound increase in bone turnover, losses in BMD and increased vertebral fractures, similar to those observed in general osteoporosis cohorts, and thus its cessation without consolidation therapy is not recommended.77
Teriparatide
Osteoanabolic agents that simulate bone formation provide the most optimistic treatment for patients with low turnover in CKD. Teriparatide is a PTH analogue that stimulates osteoblastic activity and bone formation and, when given in cyclical doses, results in BMD gains and reduced vertebral fracture rates in patients with osteoporosis. In a small study in patients on haemodialysis with adynamic bone disease, teriparatide improved low BMD, with no significant change in levels of bone turnover markers (CTX, PTH, alkaline phosphatase) after six months of therapy.78 Additionally, no safety concerns were reported in small pilot studies of its use across all ranges of CKD, including dialysis patients.78-80 However, there is a concern that its use may potentiate cortical thinning and porosity, the principal microarchitectural abnormality observed in patients with CKD.81
Romosozumab
Romosozumab is a monoclonal antibody that promotes bone formation by selectively inhibiting sclerostin, a glycoprotein which inhibits the Wnt signalling pathway that normally promotes bone resorption.82 Romosozumab has been associated with BMD gains and reduced fracture rates in osteoporosis populations and is listed on the PBS for severe osteoporosis.83,84 A recent post-hoc analysis in patients with mild to moderate CKD (eGFR >30 mL/min/1.73 cm2) taking romosozumab showed similar improvements in both lumbar and femoral neck BMDs, reduced relative risk of new fractures and stable renal function, without an increase in adverse events over 12 months.85 A small observational study in patients on haemodialysis taking romosozumab also showed improvements in BMD without significant adverse events.86 However, concerns about an increase in cardiovascular events have been raised and, given that patients with CKD already exhibit elevated cardiovascular risk, the use of romosozumab as a safe anabolic treatment in this cohort remains to be elucidated.87
Conclusion
Patients with CKD have higher rates of fracture compared with the general population, which is associated with increased morbidity and mortality. Patients with CKD-MBD require a multidisciplinary and individualised treatment approach based on clinical, biochemical and imaging parameters to optimise their bone health. There have been recent advances in diagnostic strategies, primarily the wider acceptance of DXA, and increasing data for safety and efficacy of antiosteoporosis therapies, but evidence gaps remain. The potential risk of hypocalcaemia (predominantly with denosumab use) and deterioration in vascular disease (with osteoanabolics) may offset their benefits in fracture reduction. Further research is needed to better define optimal diagnostic methods and treatment approaches for this high-risk cohort. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.