Albuminuria in diabetes. How low should levels go?

Diabetic kidney problems
Kidney diseases
Diabetic kidney disease, a main cause of end-stage kidney disease requiring renal replacement therapy, is associated with significant cardiovascular mortality. Reducing albuminuria confers cardiac and renal protection in the longer term.
- Albuminuria not only causes but also reflects structural damage to the kidneys.
- Albuminuria and a decline in glomerular filtration rate are key prognostic markers in diabetic kidney disease (DKD).
- Albuminuria is predictive not only of kidney function but also of cardiovascular risk and all-cause mortality.
- Clinical studies use reductions in the level of albuminuria as a surrogate marker of renoprotection.
- Current and future therapies for DKD aim to lower albuminuria and hence reduce the progression of kidney disease and minimise cardiovascular risk.
- The two main classes of drugs shown to confer renoprotection and cardioprotection in DKD are the renin-angiotensin-aldosterone system blockers and the sodium-glucose cotransporter-2 inhibitors.
- It is unclear whether aiming to lower albumin in the normoalbuminuric range translates to cost-effective benefit.
The number of people with all stages of chronic kidney disease (CKD) reached almost 700 million worldwide in 2017. Driven by increasing diabetes and obesity, the incidence of diabetic kidney disease (DKD) is growing exponentially. DKD, the main cause of CKD, is characterised by albuminuria, declining glomerular filtration rate, hypertension, kidney fibrosis and increased cardiovascular risk. Ultimately, dialysis or kidney transplantation is required to sustain life. Despite effective forms of renal replacement therapy, CKD is the twelfth leading cause of death worldwide.1 DKD has led to large personal and socioeconomic costs, especially in the context of limited organ donation. Although albuminuria and CKD are associated with increased cardiovascular risk, they are not variables in cardiovascular risk prediction calculators commonly used for risk assessment.2
This article discusses measurement of albumin levels and the definition of albuminuria, as well as the importance of albuminuria as a modifiable risk factor. The question of what levels of albuminuria should be targeted is considered in the context of albumin as a surrogate marker in clinical trials and the feasibility of achieving clinically meaningful renal endpoints.
Measuring and defining albuminuria
Albumin is the main type of protein in the urine, and an initial screening method for albuminuria is a simple urine dipstick test. It is important to note that a standard dipstick urinalysis detects protein with bromophenol blue indicator dye and is most sensitive to albumin and less sensitive to Bence Jones protein and globulins. It does not detect abnormal levels of albumin in the microalbuminuric range, and the albumin level can fall below the detection limits if the urine is very dilute.
Albumin can be more accurately quantitated in two ways. The first is by collecting urine over a 24-hour period and measuring the total amount of albumin excreted in that period. This is cumbersome and is not the most reliable method, as often the collection is incomplete due to patient factors. A simpler, more practical and preferred approach is to collect a single random sample of urine (‘spot urine’) and to calculate the urinary albumin to creatinine ratio (UACR), which accounts for either a concentrated or a dilute spot urine sample.If the UACR indicates albuminuria, then testing should be repeated twice within three months to see if albuminuria is persistent. A UACR test should be done at least once a year if the patient has diabetes or high blood pressure, and every two years if the patient is obese, smokes or has cardiovascular disease, a family history of CKD or is Aboriginal or Torres Strait Islander.
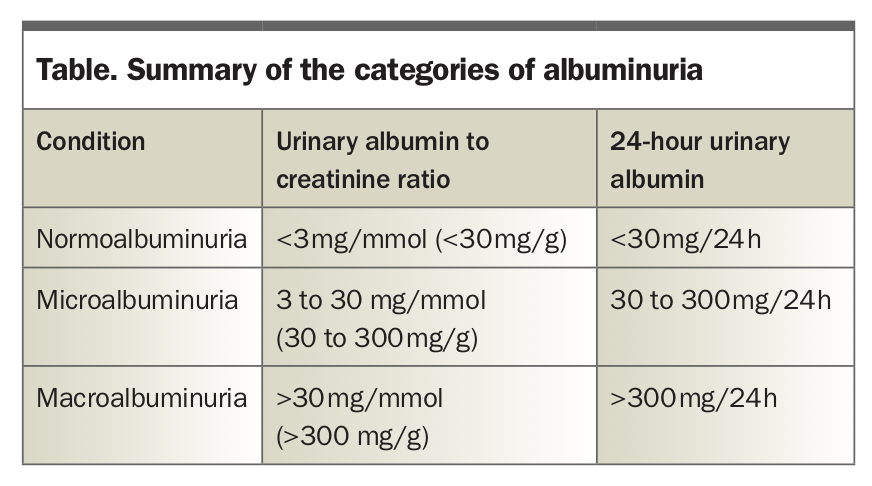
Albuminuria can be classified as either microalbuminuria or macroalbuminuria, but recently the reporting of specific levels is encouraged as it is recognised that albuminuria represents a continuous risk for cardiovascular and renal disease. Moderately increased urinary albumin, or microalbuminuria, is defined as an albumin excretion rate of 30 to 300 mg/day or an albumin to creatinine ratio of 3 to 30 mg/mmol of creatinine (in SI units). Severely increased urinary albumin, or macroalbuminuria, is defined as an albumin excretion rate of greater than 300 mg/day or a UACR of greater than 30 mg/mmol of creatinine. This is summarised in the Table. These two measurements correlate well in the non-nephrotic proteinuria range. Importantly, there is a clear trend towards conceptualising albuminuria as a continuum in the context of estimated glomerular filtration rate (eGFR) and to use strategies to reduce it if it is progressing, regardless of the ‘category’ of albuminuria.3
{kind=link}
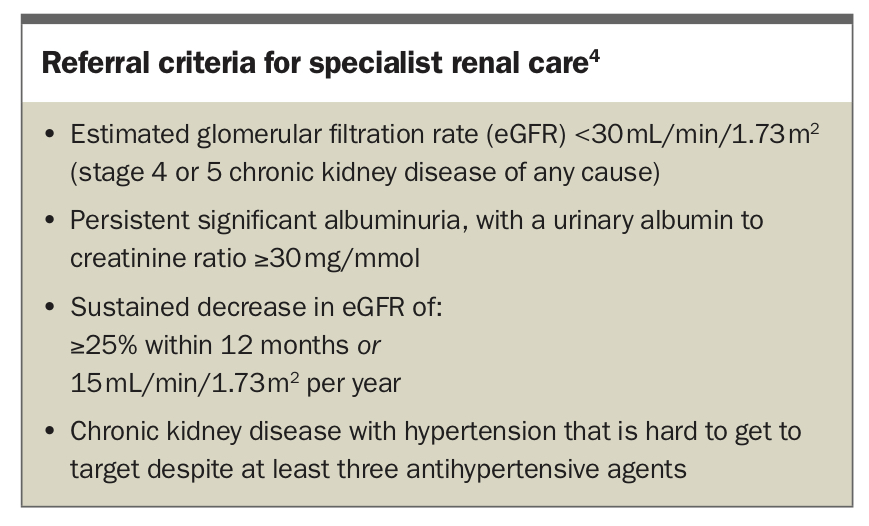
The presence of albuminuria implies structural damage to the nephron unit, which is the glomerular filtration barrier. It is one of the earliest signs of DKD as well as other forms of CKD, before the patient has any symptoms attributable to kidney damage. In addition, given there is effective treatment to halt progression, it is imperative to screen early in patients with diabetes, as albuminuria contributes to renal inflammation and scarring.3 Albuminuria is a modifiable risk factor in both DKD and cardiovascular disease and strong evidence of improved outcomes supports the use of pharmacological therapies (see below). It is important to note that albuminuria may be caused by other nondiabetic abnormalities and that it can be present transiently for other reasons such as exercise, inflammation, fever or upright body position. Hence, repeated quantitation to confirm persistence of albuminuria is required. Indications for specialist referral according to the Kidney Health Australia guidelines for CKD are summarised in the Box.4
{kind=link}
Reducing albuminuria confers renoprotection and improves cardiovascular outcomes
In addition to modification of lifestyle factors, weight reduction and optimisation of blood pressure and glycaemic control, renin-angiotensin-aldosterone system (RAAS) blockade and sodium-glucose cotransporter-2 (SGLT-2) inhibition have been shown to reduce albuminuria, delay the progression of kidney disease and reduce cardiovascular risk.5,6 Combined therapy with an ACE inhibitor and an angiotensin receptor blocker is not recommended, however, owing to the risk of acute kidney injury and hyperkalaemia.7
Evidence from a recent meta-analysis of three major trials (EMPA-REG, CANVAS and DECLARE TIMI) of SGLT-2 inhibitors in patients with type 2 diabetes showed use of SGLT-2 inhibitors reduced risk of cardiovascular death and hospitalisation from heart failure by 23%, with secondary endpoint analyses demonstrating a 45% reduction in risk of DKD progression.8-11 The CREDENCE study showed reduced albuminuria as well as improved cardiorenal outcomes with the SGLT-2 inhibitor canagliflozin.12 Importantly, a post hoc analysis demonstrated that early changes in albuminuria were independently associated with long-term kidney and cardiovascular outcomes.13
The outcomes of more recent trials such as Dapagliflozin in Patients with CKD (DAPA-CKD) and Cardiovascular and Renal Outcomes with Empagliflozin in Heart Failure (EMPEROR-Reduced) suggested that the cardiorenal benefits of SGLT-2 inhibitors extended to patients with nondiabetic kidney disease (eGFR >20 mL/min/1.73 m2 in EMPEROR-Reduced, and eGFR >25 mL/min/1.73 m2 in DAPA-CKD) as well as those with established heart failure (ejection fraction <40%), independent of diabetes status.14,15 Recently, the FIDELIO study demonstrated that adding finerenone (a nonsteroidal, selective mineralocorticoid receptor antagonist) to RAAS blockade resulted in lower risks of CKD progression and cardiovascular events compared with placebo in patients with type 2 diabetes and CKD, although finerenone resulted in a higher incidence of hyperkalaemia-related discontinuation of the trial regimen.16
One of the mechanisms by which both RAAS blockade and SGLT-2 inhibition protect the kidneys is by reducing hyperfiltration, a surrogate marker of raised intraglomerular pressure and an important early initiator of DKD.17 This, together with systemic haemodynamic effects on blood pressure, is likely to be why they reduce albuminuria.18 There is clear evidence, especially in type 2 diabetes, that reducing albuminuria affords kidney protection and reduces cardiovascular risk.19,20 The mechanism by which this protection occurs is beyond just a reduction in albuminuria.
The SGLT-2 inhibitors empagliflozin, dapagliflozin and ertugliflozin are only registered to be started above an eGFR of 45 mL/min/1.73 m2 and stopped when it falls below this. Although glucose-lowering effects are reduced as eGFR falls, lowering of urinary albumin, renoprotective and cardiovascular benefits, including reduction in heart failure, are consistently observed across all levels of eGFR.
Validity of albuminuria as a surrogate endpoint in clinical trials
Ideally, the presence and extent of kidney disease are best determined by a kidney biopsy as the tissue can be histologically inspected for inflammation, fibrosis and relevant markers of early disease activity. However, this is an invasive procedure and not without risk. Furthermore, it is often not required or justified for a diagnosis in DKD, which is often determined clinically, typically in the presence of a long history of poor diabetic control associated with hypertension, retinopathy, neuropathy, smooth normal-sized kidneys, albuminuria, absence of haematuria and a steady decline in GFR of 2 to 5 mL/min/year, in the absence of alternative CKD causes. Biomarkers such as serum creatinine level (to calculate the eGFR) and urinary albumin level are the best surrogate markers currently available and are well-accepted renal endpoints in clinical trials.21
How low should albuminuria go?
Most clinical trials furnishing clinicians with evidence-based guidelines for DKD use a predetermined albuminuria endpoint such as a 30% reduction, which is accepted by the US Food and Drug Administration as being a clinically meaningful decrease.21 However, there is also evidence to suggest that the relationship between albuminuria and renal and cardiovascular risk is continuous, even in the normal range and not only among individuals with type 2 diabetes but also among the general population.22-25 What is less clear is whether there is any long-term cardiorenal benefit in further reducing albumin within the currently accepted normal range (UACR <30 mg/g) and whether this is cost-effective. A multicentre controlled trial involving 285 normotensive patients with type 1 diabetes and normoalbuminuria who were randomly assigned to receive losartan 100 mg daily, enalapril 20 mg daily or placebo followed participants for five years. This study showed histologically there was no slowing of renal disease progression;26 however, there is evidence to suggest that RAAS blockade in combination with the SGLT-2 inhibitor empagliflozin prevents the development of albuminuria among normoalbuminuric patients.27,28
The challenges and limitations in conducting clinical trials in kidney disease to achieve a meaningful outcome for patients are significant. The challenges include executing an adequately powered randomised trial, which often takes many years, and determining clear, achievable renal and nonrenal endpoints within a realistic timeframe in a cost-effective manner. Innovation in clinical trial design is exemplified by the Study of Diabetic Nephropathy with Atrasentan (SONAR) trial, a phase 3 clinical outcome trial to determine whether atrasentan, a selective endothelin-1 receptor antagonist, can safely delay or prevent progression to end-stage renal disease. The study used an enrichment design to select participants on the basis of drug tolerance (for assessing safety) and responder status (for assessing efficacy) before randomisation.29,30 The rationale for an enrichment strategy is to enhance the selection of patients who would benefit most and exclude those unlikely to benefit from the drug. Unfortunately, this trial was stopped early due to ‘futility’ (a lower than expected event rate for the renal composite endpoint), but on analysis suggested significant benefit. As a consequence, atrasentan is now being trialled in immunoglobulin A nephropathy. This highlights the challenges of trial design in CKD.
Conclusion
There is strong evidence that reducing albuminuria in patients with DKD using SGLT-2 inhibitors in combination with RAAS blockade is associated with a reduction in renal disease progression and cardiovascular risk. SGLT-2 inhibitors have benefits beyond their glucose-lowering effects and should be considered for renal and cardiac protection, given the well-described glucose-independent mechanisms that converge to bring about the clinically measurable outcome of a reduction in albuminuria. There may be long-term value in reducing albuminuria levels even within the normal range; however, the safety profile and cost–benefit ratio for stakeholders are yet to be determined. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.