Type 2 diabetes and multimorbidity. Factors affecting decision-making

Diabetes type 2
Diabetes complications
In Australia, 90% of people with type 2 diabetes live with multiple medical conditions. The management of multimorbidity requires recognition of the limitations of individual disease-focused guidelines. Care needs to focus on the person’s health goals and shared decision making, with regular review of treatment burden and pharmacological management.
- Multimorbidity is usual in people with type 2 diabetes.
- Single disease-focused guidelines contribute to the treatment burden.
- Goal-orientated care involves the identification of patient priorities and health outcomes.
- A Home Medicines Review (MBS Item 900) can be used to optimise prescribing in general practice.
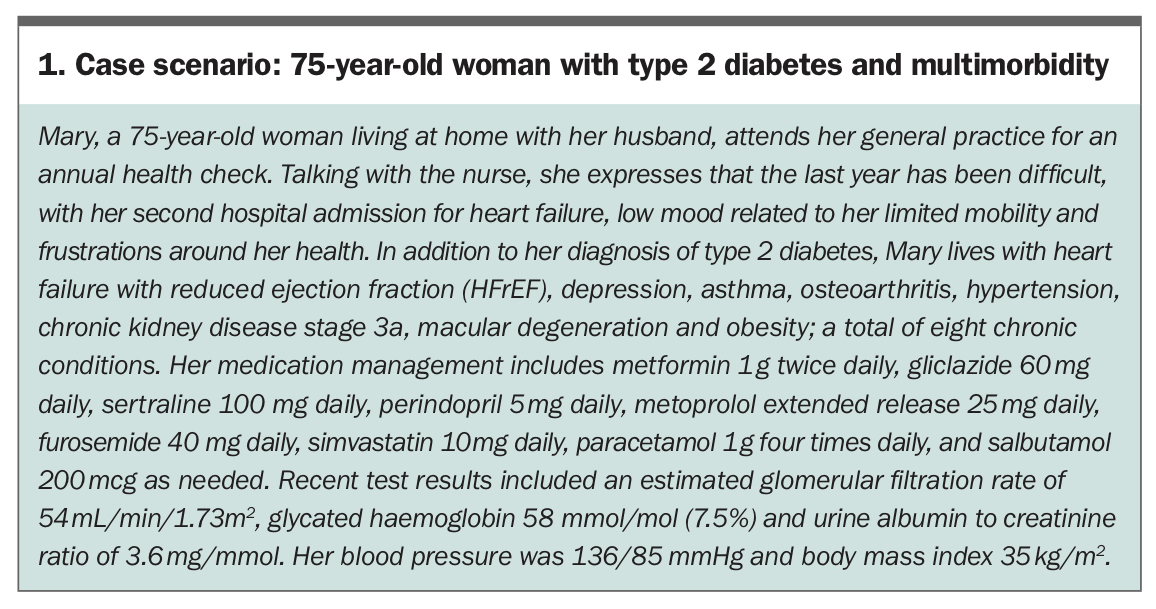
In Australia, over 90% of people with type 2 diabetes attending general practice live with multimorbidity, which is generally defined as the presence of two or more chronic conditions.1,2 In general practice, multimorbidity is associated with increased visits to general practice and polypharmacy.3 Other definitions of multimorbidity include ‘complex multimorbidity’, the co-occurrence of three or more chronic conditions affecting three or more different body systems.4 Conditions contributing to multimorbidity can be additionally characterised as concordant and discordant conditions. Concordant conditions share management goals, for example, hypertension and type 2 diabetes, but co-existing asthma is considered a discordant condition.5 For the purpose of this article, we will define multimorbidity as two or more conditions, while acknowledging that an increasing number of discordant conditions increases the complexity of management.5 Although the discussion is primarily focused on type 2 diabetes as the index condition, the principles can be applied to the broader population. A case scenario, presented in Box 1, is used as an example of applying these principles.
{kind=link}
Consequences of multimorbidity and limitations of guideline-focused care
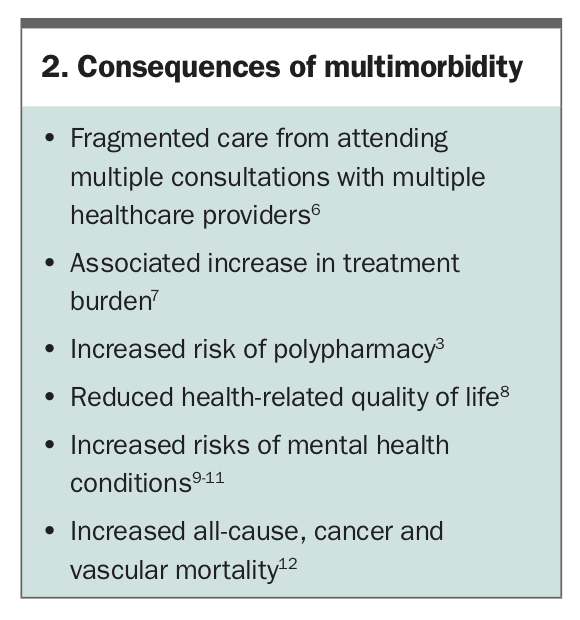
Multimorbidity is associated with many challenges, especially for people with type 2 diabetes, as outlined in Box 2.6-12 Multimorbidity and single disease-focused guidelines contribute to increased treatment burden, as discordant conditions do not share management recommendations.7 Following single disease-focused guidelines can result in polypharmacy and complicated self-management regimens with an increased risk of adverse events.13,14 Many guidelines are developed based on studies of people with specific conditions, with multimorbidity excluded or not considered in studies.15 Recently, the Royal Australian College of General Practitioners/Diabetes Australia guidelines have included recommendations for managing a person with type 2 diabetes and multimorbidity.16 The principles of care of a person with multimorbidity include:
{kind=link}
- establishing the treatment burden
- identifying patient goals, values and priorities
- performing a medication review focusing on benefits and harms of each medication
- developing a management plan.17
These recommendations are in keeping with the Ariadne principles of realistic goal-setting between healthcare professionals and people with multimorbidity.18 The Ariadne principles propose assessing the person’s conditions with prioritisation of health problems based on their preferences. Considering the patient’s preferences is particularly important, as evidence suggests that alignment of priorities between healthcare professionals and people with multimorbidity are low.19 People with multimorbidity may prioritise health issues based on their daily experiences rather than longer term outcomes, such as prioritising analgesia for diabetic neuropathy over glycaemic control.19 Following these principles, individualised management with a planned review of goals can be arranged, using clinical templates and GP management plans.18 In treating people with type 2 diabetes and multimorbidity in general practice, decision- making needs to be person-centred, with shared decision-making determining goals that focus on the person’s quality of life and functional conditions while limiting inappropriate prescribing.20 Person-centred care provided in general practice is based on longitudinal knowledge of people and provides the basis for better recognising health needs over time.21 In a qualitative study, people with multimorbidity indicated a preference for co-ordinated care and a focus on self-management and psychological aspects of care.22
Goal-orientated care
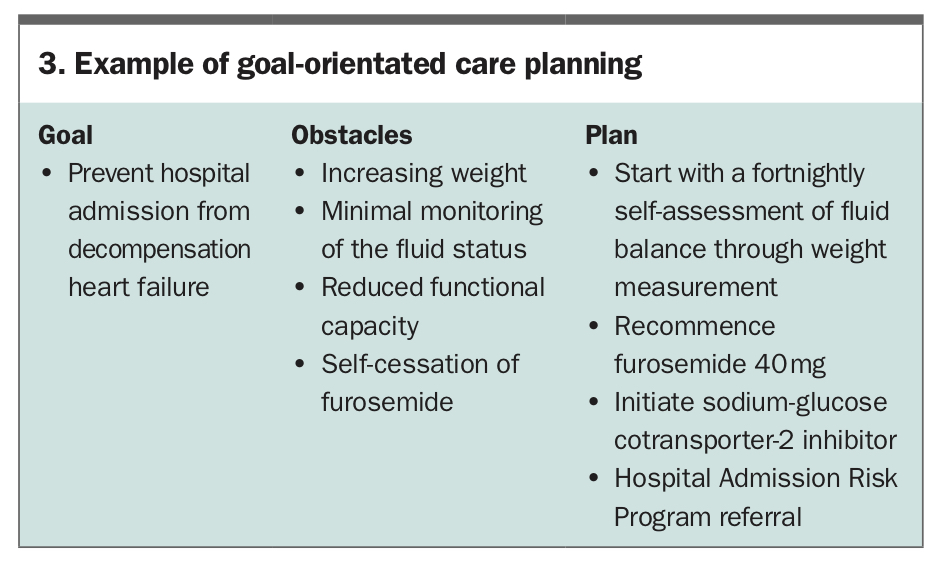
Goal-orientated care adopts a person-centred approach to managing a person with multimorbidity instead of using single-disease problem lists.23 It allows discussion of priorities related to the person’s health and values as opposed to managing each disease separately within the constraint of single disease guidelines.24 Personal health goals can include preventing premature death or disability, maintaining or improving quality of life, optimising personal growth and decreasing unwanted investigations and interventions at the end of life through advanced-care planning.25 In practice, questions such as, ‘What is important to you?’ can initiate goal-orientated care. An example of goal-orientated care planning is illustrated in Box 3.
{kind=link}
Assessment of treatment burden
Treatment burden refers to the demands and impact on wellbeing from treatment and self-management of medical conditions.26 Treatment burden can include self-management of a condition, attending appointments and self-education about the conditions and their management.27 With increasing numbers of chronic conditions, people spend longer self-managing their conditions (up to 80 hours per month for type 2 diabetes and multimorbidity).28 Frequently, the burden of daily self-management is not apparent to healthcare professionals when periodically assessing health status using prespecified targets during consultations, for example, lowered glycated haemoglobin level or weight loss.29
People with multimorbidity have increased visits to primary care, which provides opportunities for assessment of treatment burden.30 Practically assessing treatment burden involves exploring how a person’s health conditions and self-management strategies impact their mental health, wellbeing and quality of life. It is also useful for establishing the burden of treatment on carers and family members. Given the increased prevalence of mental health disorders among people with type 2 diabetes, discussing and addressing any mental health concerns related to living with chronic conditions is also needed. Using validated tools such as the Problem Areas in Diabetes (PAID) scale identifies areas of diabetes management that may be causing psychological distress and the areas of treatment a person with diabetes finds burdensome.31 Assessing the treatment burden in a person-centred manner allows for identifying the ‘invisible’ work done by people with multimorbidity when self-managing multiple conditions.32,33
Applying goal-orientated care and treatment burden principles in Mary’s case
Mary identified that her primary goal was to avoid another hospitalisation related to her heart failure symptoms. Exploring her current self-management revealed that regular assessment of fluid status at home had not occurred, and Mary had self-ceased furosemide due to concerns it was ‘damaging her kidneys’. Mary explained she always disliked weighing herself due to previous negative experiences about her weight management. Her legs have recently increased in size, and her mobility has reduced. The obstacles were explored using motivational interviewing, and after receiving education on fluid monitoring to prevent hospitalisation, Mary agreed to monitor her weight fortnightly at home.
Prescribing in type 2 diabetes and multimorbidity
Multimorbidity impacts people’s ability to self-manage medication regimes owing to complexity, with people who have three chronic medical conditions taking between six to 13 medications per day if complying with guidelines for each individual condition.34,35 Medications with value across concordant conditions could reduce polypharmacy. Although metformin is still recommended as initial therapy, if intensification of therapy is indicated the addition of a sodium-glucose cotransporter-2 (SGLT-2) inhibitor or glucagon-like peptide-1 receptor agonist can be considered in people with type 2 diabetes who also have cardiovascular disease, cardiovascular risk factors or chronic kidney disease.36 However, single-disease guidelines rarely account for serious drug-drug interactions. A study has shown that following the prescribing recommendations of the UK national clinical guidelines for type 2 diabetes as well as those for 11 other common conditions could result in 32 potentially serious drug-drug interactions.37,38
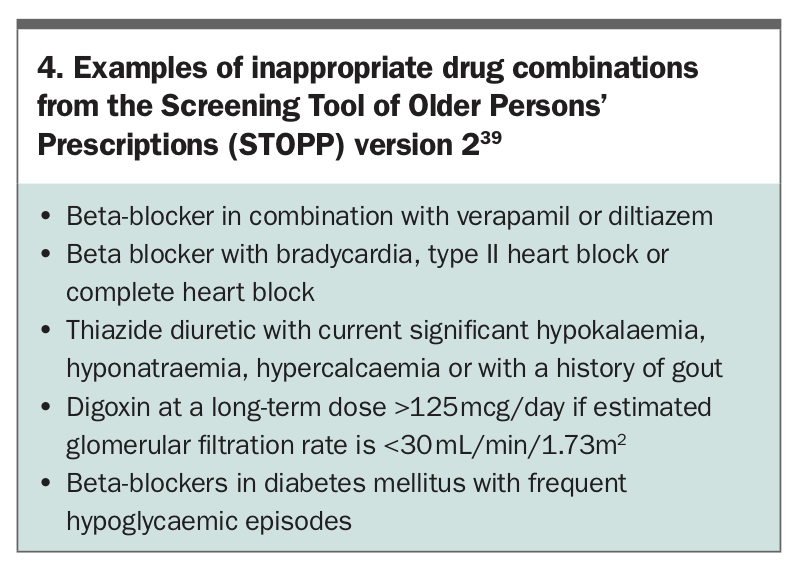
When prescribing medications for a person with type 2 diabetes and multimorbidity, consideration of the person’s overall life expectancy is needed. Consider medicines that could be stopped or appropriately prescribed using tools such as the Screening Tool of Older Persons’ Prescriptions and the Screening Tool to Alert Doctors to Right Treatment (STOPP/START criteria; Box 4). The STOPP tool, developed by geriatricians, guides review of around 80 indicators of inappropriate prescribing in older people, and the START tool recommends appropriate prescribing for older people with chronic conditions.39 Referring to the person with type 2 diabetes’ goals and values while addressing potentially inappropriate prescribing allows for shared decision-making when deciding to start or stop any medication. Having a home medicines review by a pharmacist (MBS Item 900) allows for identifying drug interactions, inappropriate medication use, adherence issues and excessive medication doses and can increase patients’ ability to discuss potential medication changes with their GP.40,41
{kind=link}
Applying prescribing principles in Mary’s case
Considering Mary’s concurrent asthma, type 2 diabetes and heart failure, continuation of metoprolol was discussed and deemed appropriate given Mary’s goals related to reducing hospitalisation and using salbutamol minimally.42 After referring to the Australian evidence-based clinical guidelines for diabetes, an SGLT-2 inhibitor was identified as a more appropriate glycaemic medication with cessation of gliclazide. This was decided on consideration of the risk of hypoglycaemia and lack of evidence of cardiovascular benefits with gliclazide, and also Mary’s dislike of self-monitoring of blood glucose levels and her goal of preventing hospitalisation. Mary was educated regarding the risk of developing diabetic ketoacidosis (which can be euglycaemic) if dehydrated or having a major procedure with prolonged fasting while taking an SGLT-2 inhibitor.43 A referral to a local Hospital Admission Risk Program was arranged for cardiac rehabilitation. A general practice review appointment was arranged for two weeks’ time to discuss her fluid status and monitor for symptoms following commencement of the SGLT-2 inhibitor.
Conclusion
Decision-making with people who have type 2 diabetes and multimorbidity requires a focus on the goals that are important to a person and development of an appropriate management plan while considering prescribing choices that benefit concordant conditions. This article has highlighted these principles as they apply in real-world general practice. ET