Thyroid hormone replacement therapy in hypothyroidism

Dr Luisa Rosi is an Advanced Physician Trainee in Endocrinology and an Endocrinology Registrar in the Department of Endocrinology and Diabetes at The Alfred, Melbourne. Professor Topliss is a Senior Endocrinologist in the Department of Endocrinology and Diabetes at The Alfred; and a Professor of Medicine at Monash University, Melbourne, Vic.
Thyroid diseases
Endocrine diseases
Hypothyroidism and thyroid hormone replacement therapy can generally be managed in general practice, with endocrinologist input recommended for more complex cases. Decisions about who, when and how to treat should be based on the aetiology of hypothyroidism, thyroid function test results and patient circumstances.
- Hypothyroidism is a common condition that will be managed by multiple clinicians across a patient’s life span.
- Levothyroxine is there commended first-line treatment for hypothyroidism, with initial four- to six-weekly dose titration, guided by thyroid function test results to achieve stable euthyroidism, dependent on aetiology.
- Liothyronine treatment alone or in combination with levothyroxine is not routinely recommended due to a paucity of robust clinical evidence of its efficacy and safety.
- Persistent hypothyroidism that is out of keeping with anticipated thyroid hormone requirements should lead to an evaluation of adherence or reduced drug absorption due to concomitant food or medication intake or bowel disease.
Hypothyroidism is a common condition that often requires lifelong thyroid hormone replacement therapy. It is important to consider patient circumstances, aetiology of hypothyroidism and treatment targets when prescribing and managing patients receiving thyroid hormone replacement therapy.
Aetiology of hypothyroidism
Thyroid hormone regulates growth, development, thermogenesis and body metabolism. The two biologically active thyroid hormones are thyroxine (T4) and triiodothyronine (T3). T4 is solely secreted by the thyroid gland, whereas 80% of circulating T3 is derived from T4 by deiodination in various tissues, especially liver, kidney, muscle and skin.1 The circulating half-life of T4 is about one week, and that of T3 about one day.
Primary hypothyroidism is most often caused by autoimmune thyroid disease. There is usually a gradual transition from euthyroidism with positive thyroid antibodies to subclinical hypothyroidism, then overt hypothyroidism. If the thyroid stimulating hormone (TSH) level is raised and antibodies are present, overt hypothyroidism develops at a rate of about 5% per year. Primary hypothyroidism can also result from surgery or radioiodine therapy for hyperthyroidism or total thyroidectomy for thyroid cancer. Medications such as lithium, amiodarone, immune checkpoint inhibitors and other immunoactive agents can impair thyroid function, particularly in the presence of autoimmune thyroid disease.
Secondary hypothyroidism is caused by pituitary or hypothalamic disease, such as pituitary tumour and hypophysectomy, and can result from use of the immune checkpoint inhibitor ipilimumab. Secondary hypothyroidism is much less common than primary hypothyroidism.
Thyroid function tests
There is no single measure or biomarker of thyroid hormone action at the cellular or clinical level. Laboratory assessment of thyroid function mainly involves assays of free T4 (FT4) and TSH. In primary hypothyroidism, the TSH level is elevated: overt hypothyroidism is defined as high TSH and low FT4 levels, and subclinical hypothyroidism or mild thyroid failure as high TSH and normal FT4 levels.
In secondary hypothyroidism, TSH level is not elevated despite a low FT4 level. If secondary hypothyroidism is known or suspected, the clinical notes should inform the laboratory of this, and both FT4 and TSH levels should be requested, as measurement of TSH alone cannot be used for diagnosis or monitoring.
In people with profound medical illness, abnormalities of thyroid function test results are common.2 This nonthyroidal illness (NTI) can cause transient low free T3 (FT3) levels in people with acute illness and low FT4 levels in those with severe or critical illness. The TSH level can also be low in people with NTI, although it is rarely suppressed to the level seen in hyperthyroidism, and it may become mildly transiently elevated during recovery. A diagnosis of hypothyroidism in people with severe NTI can therefore be difficult and is best left, if clinically possible, until they have recovered.
Reverse T3, the metabolically inactive form of T3, is not a clinically useful measurement, and testing for it should not be requested for people with thyroid disease or NTI.
Prescribing thyroid hormone replacement therapy
Hypothyroidism is treated with thyroid hormone replacement. Synthetic levothyroxine is the pharmaceutical form of T4. It is the recommended first-line thyroid hormone replacement therapy because of its efficacy, purity, accuracy of dosing, satisfactory absorption, long half-life with production of stable FT3 levels, long experience of safety and low cost. Levothyroxine is deiodinated to T3, so an adequate supply of both hormones can generally be achieved with levothyroxine alone.
Liothyronine is the pharmaceutical form of T3. Liothyronine therapy alone is mainly used transiently during preparation for radioactive iodine therapy for thyroid cancer and (rarely long term) for apparent intolerance or poor absorption of levothyroxine. Treatment with liothyronine is difficult to manage, as its endogenous concentration varies markedly throughout the day in relation to time of ingestion, due to its short half-life. It is unclear if this nonphysiological variation of T3 levels from high to low is without risk.3 A low FT4 level in a patient receiving liothyronine therapy alone is to be expected and does not mean hypothyroidism; TSH level is the best laboratory guide to thyroid status.
There is no established role for combined levothyroxine and liothyronine therapy, either as separate synthetic agents or as a desiccated thyroid gland extract of animal origin (DTE). Combination levothyroxine and liothyronine therapy has been used in multiple small trials of patients dissatisfied with levothyroxine alone but has not been shown to have any clear general benefit.4,5 No DTE has been approved by any major national drug regulatory authority.
Which agents?
Patients with limited residual thyroid function will require about 1.6 mcg of levothyroxine per kilogram of lean body mass. Those with no thyroid function may require more, and patients with subclinical hypothyroidism may require less.6
Australia has four levothyroxine formulations available on the PBS: Oroxine, Eutroxsig, Eltroxin and Levoxine. Oroxine and Eutroxsig should be refrigerated for long-term storage unless tablets are to be taken within two weeks. Eltroxin and Levoxine do not need refrigeration but should be stored below 25°C. All forms of tablets should be kept dry and out of direct sunlight. Eltroxin may be slightly (about 10%) less potent than Oroxine, Eutroxsig and Levoxine, which are bioequivalent and therefore dose interchangeable. Nevertheless, a thyroid function test review is recommended six weeks after any brand change.
About 60 to 80% of levothyroxine is absorbed in the two to four hours after an oral dose in the fasting state.7 Levothyroxine should therefore be taken on an empty stomach, with water only, separately from other medications and at least 30 minutes before food, usually on waking in the morning.
If only liothyronine (Tertroxin) is used, the usual daily dose is 20 to 40 mcg in a divided dose. Any trial of combination therapy should be reserved for those with persistent symptoms of hypothyroidism despite having TSH levels stabilised to near the population median (1 to 2 mIU/L) with levothyroxine therapy, in the absence of, or with well-managed, nonthyroidal health problems. The optimal ratio of levothyroxine to liothyronine in combination therapy is not established. One approach is to divide 10 to 20 mcg of liothyronine across two to three doses daily, with regular monitoring of TSH levels, aiming to avoid suppression.3 It is usual to decrease the levothyroxine dose when adding liothyronine to reduce the risk of overtreatment.8
When to treat?
When considering prescribing thyroid hormone replacement therapy, it is important to consider the severity and likely course of hypothyroidism. There is consensus that patients with primary hypothyroidism with TSH levels above 10 mIU/L should be treated. However, for patients with raised TSH levels up to 10 mIU/L and with low to normal FT4 levels, the benefit is less certain.6
A slightly raised TSH level (4 to 10 mIU/L) is not diagnostic of hypothyroidism, particularly when it is only marginally raised. Even if subclinical hypothyroidism is present, treatment with levothyroxine may not be appropriate. Repeat testing and further clinical evaluation should occur over six to 12 months. Endocrinologist consultation should be considered.
The potential adverse effects of low or suppressed TSH levels from thyroid hormone therapy, including a risk of cardiac arrhythmia and bone loss, are particularly important for older patients.9
Subclinical hypothyroidism
Subclinical hypothyroidism is not generally associated with symptoms of hypothyroidism. These patients are occasionally symptomatic, but the causal relationship to the change in thyroid function is usually uncertain. The biochemical abnormality should be confirmed as consistently present over a period of at least four to six weeks.10
Treatment for subclinical hypothyroidism is recommended for people who are pregnant or trying to conceive. In adults aged over 65 years with subclinical hypothyroidism, no symptomatic clinical benefit has been shown from 12 months of treatment.11 In those younger than 65 years, where long disease duration may allow development of cardiovascular disease, the treatment decision should be based on patient preference, comorbidities such as dyslipidaemia and the likelihood of progression to overt hypothyroidism. If the management decision is observation, yearly follow up is appropriate.
Pregnancy-associated subclinical and clinical hypothyroidism
A fetus requires a maternal T4 supply until the fetal thyroid is functioning, at 16 to 20 weeks’ gestation. Before conception, women with known hypothyroidism should have their levothyroxine dose optimised to produce a TSH level in the normal range. After conception, increased metabolism of levothyroxine means there is a 30 to 50% increased requirement. This can be supplied by doubling the usual daily levothyroxine dose on two days of the week.12
Current guidelines recommend measurement of TSH levels once pregnancy is confirmed in all women aged over 30 years; those from an iodine-deficient area; and those with known autoimmune disease (including type 1 diabetes) or a family history of autoimmunity, known presence of thyroid antibodies, subfertility, prior fetal loss or preterm delivery or prior head and neck irradiation or surgery. Treatment with levothyroxine should be recommended for women with a TSH level above the normal trimester-specific range for the TSH assay or, in the absence of this information, above 4 mIU/L.12-14 Thyroid peroxidase antibodies should be assessed in those with a TSH level above 4 mIU/L.12 In women who are thyroid peroxidase antibody negative, levothyroxine therapy can be considered when the TSH level is above 2.5 mIU/L and below the upper limit of the pregnancy-specific reference range; however, there is conflicting evidence of benefit from starting levothyroxine therapy in this group of women.14 Four-weekly monitoring for dose titration is recommended in the first and second trimesters to ensure adequate supply of T4 to the fetus.
Transient hypothyroidism secondary to thyroiditis or radioactive iodine therapy
Early in the course of autoimmune thyroiditis or after radioactive iodine therapy for Graves’ disease, biochemical hypothyroidism may develop. This can recover spontaneously, usually within six months. If symptoms require levothyroxine therapy, the long-term need for treatment should be assessed by withdrawing it after six to 12 months, followed by TSH and T4 measurement four to six weeks later.13 An elevated TSH level indicates a continuing need for levothyroxine.
Medication-associated hypothyroidism
High iodine-containing agents, including kelp tablets, potassium iodide-iodine (Lugol’s iodine) and amiodarone, can cause hypothyroidism. The daily recommended intake of iodine is 150 mcg for adults and 250 mcg for women who are pregnant or breastfeeding. Intake of more than 300 mcg daily during pregnancy can result in raised TSH levels in those with autoimmune thyroid disease.
Amiodarone 200 mg tablets contain 75 mg of iodine, which can supply 9 mg daily of iodide and cause iodide-induced hypothyroidism. Thyroid function should be checked when initiating amiodarone therapy and then every six months, to detect hypothyroidism or hyperthyroidism. If amiodarone induces hypothyroidism but is necessary for managing major arrhythmias, levothyroxine can be started and amiodarone continued.
Lithium inhibits thyroid hormone synthesis and release, with up to 19% of people using lithium developing overt hypothyroidism and 23% developing subclinical hypothyroidism.15 Lithium therapy can be continued if clinically necessary, with concomitant levothyroxine therapy.
Immune checkpoint inhibitors, such as ipilimumab (a CTLA-4 inhibitor), nivolumab and pembrolizumab (PD-1 inhibitors) and atezolizumab, avelumab and durvalumab (PD-L1 inhibitors), are used to treat malignancies and are known to cause endocrinopathies, including hypothyroidism. Treatment protocols recommend routine monitoring of thyroid function. Presence of autoantibodies (e.g. antithyroid peroxidase antibody positivity) has been found to be a risk factor for developing endocrine dysfunction in patients using immune checkpoint inhibitors.16
Alemtuzumab, a monoclonal antibody treatment for relapsing-remitting multiple sclerosis, can cause hypothyroidism but more often causes Graves’ hyperthyroidism.17
Severe hypothyroidism and myxoedema coma
Severe hypothyroidism can be treated with a full dose of levothyroxine unless the patient has concomitant cardiac disease, in which case a low dose (12.5 to 25 mcg daily) should be initiated, with gradual increments every few weeks, to avoid precipitating cardiac ischaemia. It is usual to start at the lower dose in older patients, who have a higher risk of undiagnosed ischaemic cardiac disease.
Myxoedema coma is a thyroid emergency and, if suspected, requires immediate referral to a major hospital. Treatment includes parenteral levothyroxine and/or liothyronine.
Congenital hypothyroidism
Congenital hypothyroidism is usually caused by failure of normal fetal thyroid tissue development (thyroid agenesis or lingual thyroid). Assessment of neonatal thyroid function is part of the newborn screening program in Australia. For newborn infants with hypothyroidism, biochemical and clinical parameters are normalised with levothyroxine therapy of about 10 to 15 mcg/kg/day started within the first 10 days of postnatal life. There is high-quality evidence that starting levothyroxine results in excellent outcomes; however, without treatment, neonatal hypothyroidism leads to permanent neurological deficit.13 Adjustment of levothyroxine dose with age should be guided by a paediatric endocrinologist. Overtreatment can have side effects, such as craniosynostosis.
Nonthyroidal illness
No clear evidence yet supports thyroid hormone replacement therapy for people with NTI and low FT4 levels, and there is a risk of harm, particularly in those with cardiac illness or heart failure. Therefore, use of thyroid hormone replacement therapy in people with NTI is not recommended.18
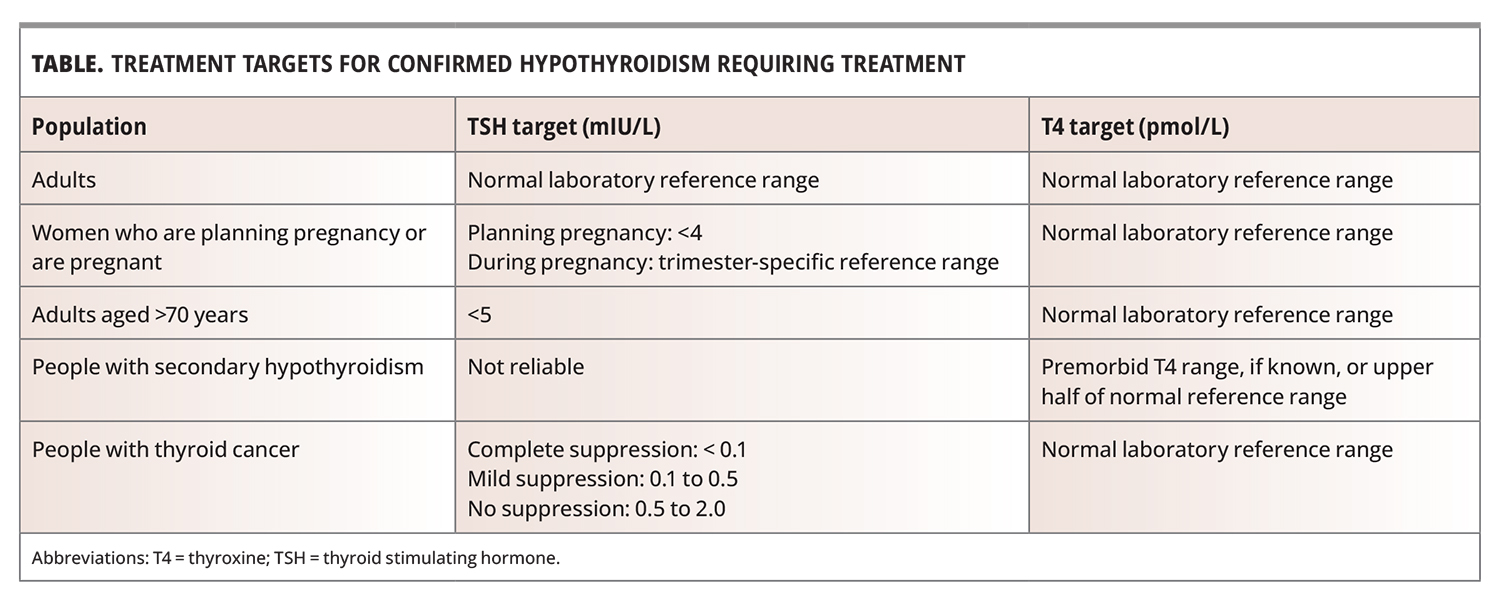
Targets for treatment of hypothyroidism and dose titration
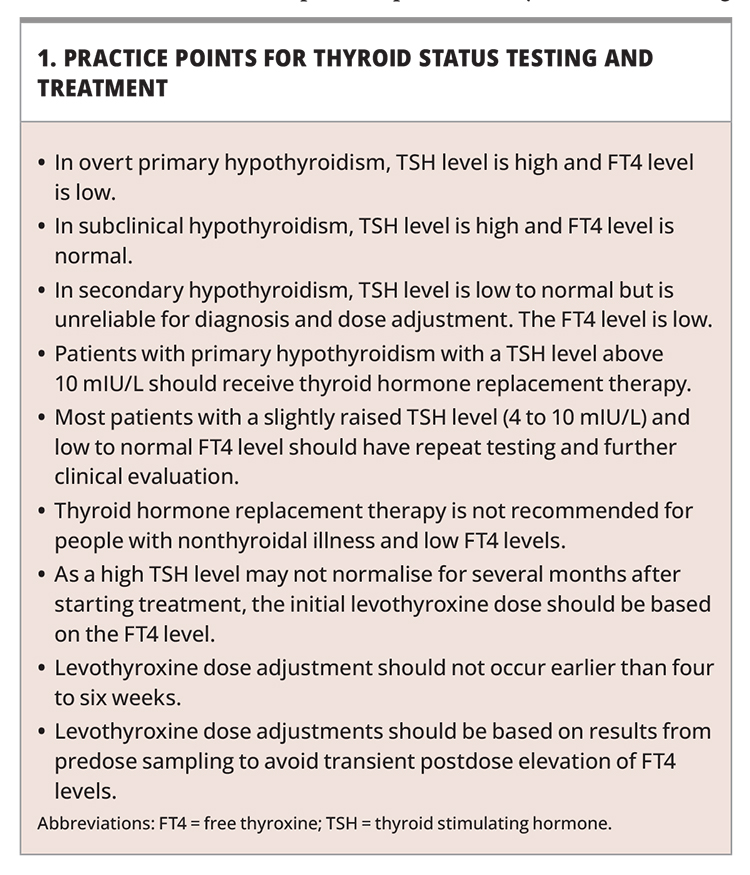
Targets for TSH and T4 levels for various population groups are outlined in the Table, and practice points for thyroid status testing and treatment are summarised in Box 1.
{kind=link}
{kind=link}
Early in the treatment of established primary hypothyroidism with a high TSH level, the TSH level may not normalise for several months, so the initial levothyroxine dose should be based on the FT4, not TSH, level.
Dose titration depends on target aims, initial thyroid function and clinical comorbidities. A full dose can be started or aimed for in those with no cardiac disease or risk factors. For those with a history of ischemic heart disease, heart failure or risk factors for these, the dose should be titrated judiciously, as significant change in thyroid hormone level can precipitate decompensation of cardiac disease.
Levothyroxine has a long half-life and takes four to six weeks to reach a plasma steady-state level. Therefore, dose titration should generally not be done before four weeks.
The finding of a high FT4 level with normal TSH level should not prompt levothyroxine dose reduction. This pattern is often caused by blood sampling being performed within a few hours after the levothyroxine dose. Adjustments should be based on results from predose sampling to avoid transient postdose elevation of FT4 levels.
In thyroid cancer treatment, a TSH level of less than 0.1 mIU/L can be a target to control cancer growth, so the levothyroxine dose should not be reduced. The managing endocrinologist should be consulted before any dose change is made for these patients.
The need for levothyroxine should be reviewed if the aetiology is thought to be transient, if causative medications have been ceased or if there is a clinical assessment that supplementation is no longer needed. Dose reduction and monitoring of thyroid function are recommended, initially six weeks after reduction or cessation of levothyroxine. If levothyroxine is ceased, a further review at six months is recommended.
Troubleshooting persistent hypothyroidism
Several factors can result in persistent hypothyroidism despite treatment.
Timing, adherence and physiological changes over lifespan
As levothyroxine should be administered first thing in the morning on an empty stomach, it is important to clarify the patient’s adherence to the dose and timing before undertaking dosage changes. Other factors to consider throughout the patient’s treatment are any change to body weight or lean body mass and advancing age, all of which can alter the patient’s requirement for thyroid hormone and therefore the required levothyroxine dose.19
Absorption
Levothyroxine tablets require an acidic environment for optimal breakdown before being absorbed in the small intestine.20 The presence of food, particularly calcium-containing food and drink, including soy-based products, milk or coffee, or several medications, including protein pump inhibitors, iron supplements, calcium carbonate, aluminium hydroxide, sucralfate, bile acid sequestrants and raloxifene, can impair absorption of levothyroxine.20 It is therefore recommended that levothyroxine be taken on an empty stomach and separated from these medications by four hours. Patients should be informed of these interactions and that new medications or changes to lifestyle can affect thyroid hormone levels, which should be monitored after any changes are made.
Small bowel disease, such as coeliac disease or untreated lactose intolerance, can also impair absorption. Gastric and small bowel surgery, especially if there is loss of small bowel, can result in malabsorption of levothyroxine.21
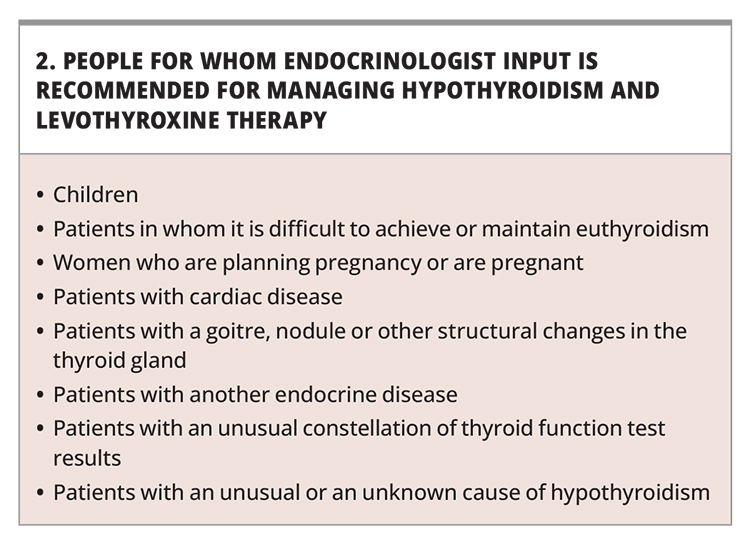
Referral to specialist
Most physicians and GPs who have an interest and experience in thyroid disease can manage hypothyroidism and levothyroxine therapy. People for whom endocrinologist input is recommended are listed in Box 2.6
{kind=link}
Conclusion
Thyroid hormone replacement treatment of hypothyroidism is simple, highly effective and safe. However, many issues, including aetiology of hypothyroidism, thyroid test results, patient circumstances, comorbidities and treatment targets, should be considered to achieve the best outcome over a lifetime of therapy. MT
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.