Sick days, type 2 diabetes and the GP

Diabetes type 2
Diabetes medicines
Many acute illnesses or infections can lead to hyperglycaemia in people with diabetes, with a subsequent risk of serious consequences. A clear written plan is essential so that patients know how they may need to adjust their usual diabetes management if they are sick from another cause and what to do in the event of a diabetes emergency.
- Sick-day management is important for people with diabetes to avoid possible serious consequences of acute illness or infection.
- Patients are best served with a written sick-day plan of diabetes therapy adjustments that may be needed when they are unwell.
- Risk and management of hyperglycaemic emergencies, including diabetic ketoacidosis associated with use of sodium-glucose cotransporter-2 (SGLT-2) inhibitors, need to be incorporated in each patient’s plan.
- Certain medications, such as metformin and SGLT-2 inhibitors, may need to be temporarily stopped in patients with severe dehydration.
Managing diabetes can present challenges in general practice, including planning for patient sick days. Sick-day plans should be based on established consensus principles and focused on individualised patient-centred care, with a broad understanding of the effects of acute illness on people with diabetes and how management and support need to be adapted to meet these challenges.1
The widespread threat of infection that has accompanied the coronavirus disease 2019 (COVID-19) pandemic has highlighted the clinical need for sick-day planning for all patients with diabetes. Good sick-day planning can be achieved using a keen practical focus combined with effective practice systems and a team-based approach to care.
What are sick days?
For people with diabetes, a sick day is defined as a short-term illness or infection from other causes that requires them to make changes to their usual diabetes management.1,2 Sick-day management plans may be a challenge for GPs in terms of how to translate medical information into practical patient education and advice. The plan should be formulated when a patient is first diagnosed with diabetes, then reviewed at least annually and when altering management strategies, when there is onset or development of diabetes complications and after an episode of illness.
Discussion in this article will be limited to type 2 diabetes, as sick-day planning for patients with type 1 diabetes requires careful multidisciplinary input and adequate specialist endocrine team support, especially when patients are using pump technologies or complex insulin regimens.3
Why is sick-day management important?
The aim of sick-day planning is to promote early assessment and proactive self-management and to prevent progression to serious consequences. Many of the clinical causes of short-term illness may give rise to hyperglycaemia (through acute and progressive insulin resistance or increased secretion of counterregulatory hormones with liver or renal dysfunction)4-8 and resulting risks that may not be obvious to patients. Identification and management of the cause of an illness will help manage the compounding risks, beyond just hyperglycaemia (e.g. gastroenteritis causing hypovolaemia aggravated by hyperglycaemic diuresis). Infections (e.g. skin, feet, urinary tract and respiratory tract) affecting patients’ cognitive state may limit their self-care abilities, increasing the risk of progressive deterioration. As hyperglycaemia accompanying acute coronary or cerebral ischaemia portends a poorer prognosis, these aetiologies need to be identified early.9,10 The use of medications such as corticosteroids may require GPs to reconsider management options, as these may destabilise blood glucose levels.4,5,7
Setting glycaemic risk levels
The RACGP advises goals for optimal glucose levels in a non- sick-day state of 4 to 7 mmol/L fasting and 5 to 10 mmol/L postprandial. A sick-day plan should emphasise the importance of increased self-monitoring of blood glucose (SMBG), usually every two hours when unwell, with the aim of re-establishing optimal blood glucose levels. It is recommended that instruction on adequate hydration needs and supportive nutrients also be part of the plan.1,2
Patients should be advised when to implement their plan: that is, if they are feeling unwell (even if their glucose level is normal), or if their glucose level is above 15 mmol/L two times in a row, or if their glucose level falls below 4 mmol/L. They should also be instructed to call their doctor or diabetes team if they become too unwell to manage the requirements for monitoring or if they need any assistance.
An important general written instruction for a sick-day plan is: ‘When unwell, some adjustments need to be made to your therapy. However, do not stop taking any medication, particularly insulin, unless advised’. Further specific instructions may include temporarily stopping certain medications, such as sulfonylureas, metformin, glucagon-like peptide-1 (GLP-1) receptor agonists and sodium-glucose cotransporter-2 (SGLT-2) inhibitors, if the patient has diarrhoea or vomiting or cannot tolerate fluids. Sulfonylureas may aggravate hypoglycaemia if the patient has limited oral intake. Metformin may worsen dehydration in patients with gastrointestinal illness and, rarely, increases the risk of lactic acidosis.11 GLP-1 receptor agonists risk aggravating nausea, and SGLT-2 inhibitors may exacerbate hypovolaemia from illness. Recent studies examining the use of non-insulin therapies in patients with COVID-19 infection have emphasised the safety of these agents, unless the patient has severe illness or requires hospitalisation.12,13
Insulin should not be ceased, but its use on sick days requires careful instruction. Patients might need to change their insulin dose according to the SMBG assessment, either because of hypoglycaemia, when a reduced dose of insulin is required, or hyperglycaemia, when an increased dose of insulin is required. The latter will typically involve temporarily increasing basal insulin doses by 10% until glycaemia is restored.2 However, the glycaemic effect of altered doses of ultra-long-acting insulins containing glargine 300 IU/mL or degludec (in coformulated insulins) may be reduced in acute illness because of the prolonged half-lives of these agents. Thus, patients using these insulins require careful SMBG. Additional prandial or rapid-acting insulins can be temporarily used to counteract a blood glucose level that is rising despite non-insulin therapy, noting the term effect of these may be only up to four hours after the dose and the effects are dose-to-glucose level-dependent. Safe use of supplemental rapid-acting insulin dosing can be achieved in a planned setting with a previously well-educated patient who is capable of performing the necessary SMBG; proactive instruction from a credentialled diabetes educator (CDE) will be an asset in this situation. Insulin doses will depend on the range of hyperglycaemia, with typical starting doses being two to four units of rapid-acting insulin if the glucose level exceeds 15 mmol/L despite other interventions.1
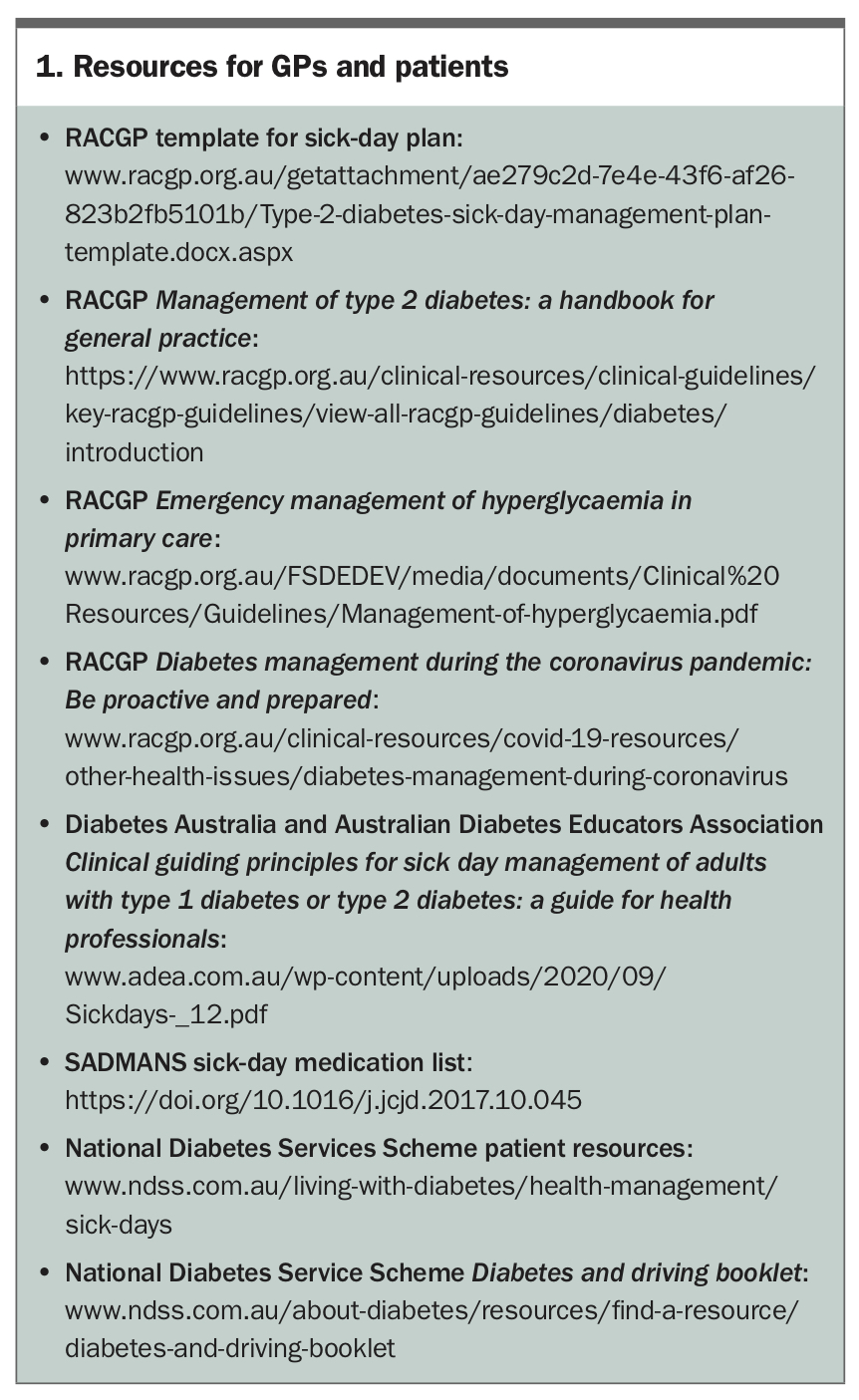
GPs who remain uncertain of the necessary advice can seek education, use available resources (Box 1) and consult appropriate diabetes experts, such as a CDE or diabetes specialist.1,2 A Canadian guideline using the acronym SADMANS (sulfonylureas, ACE inhibitors, diuretics, metformin, angiotensin II receptor blockers, NSAIDs and SGLT-2 inhibitors) was published in 2018 and gives greater detail on sick-day planning, including nondiabetes medications that are known to increase risks in patients with diabetes.14
{kind=link}
Patients with special needs
Older patients, patients with complex comorbidities such as chronic kidney disease or heart failure, and patients taking multiple medications are at greater risk from the effects of glycaemic changes that accompany sick days.15-17 As such, these patients need early identification when they are diagnosed with diabetes and regular updating of an individualised sick-day plan.
Patients with a glucose level above 15 mmol/L and blood ketone level above 1.5 mmol/L need to be assessed for a possible diabetes emergency. Urine ketone testing is not as reliable as blood ketone testing, as it may be difficult to perform in a dehydrated patient with reduced urinary output.2,18,19 Blood ketone monitoring may need to be proactively considered for patients using an SGLT-2 inhibitor, because of the risk of euglycaemic diabetic ketoacidosis (eDKA), as well as those who have had past ketoacidosis and those requiring insulin.
In addition to being rarely associated with diabetes in pregnancy, eDKA is associated with the use of SGLT-2 inhibitor therapy, including combined metformin and SGLT-2 inhibitor therapy and combined SGLT-2 and dipeptidyl peptidase-4 inhibitors. This form of ketoacidosis can occur even when glucose levels are normal and not extremely elevated (e.g. above 15 mmol/L). This can lead to the illness being overlooked, as the symptoms of eDKA might mimic triggers such as an acute illness or infection, especially in a patient with reduced fluid or oral intake and vomiting.20 Patients with low carbohydrate intake or who have recently started SGLT-2 inhibitor therapy with insulin are also at risk of eDKA.20 The risk of eDKA should serve as a reminder to check ketone levels in patients with acute illness when they are using SGLT-2 inhibitors. Blood ketone levels above 1.0 mmol/L, even with a normal glucose level, should raise the alarm for eDKA. Urgent contact with or referral to specialist care is needed if eDKA is suspected.
Patients preparing for surgery when using SGLT-2 inhibitors should be given clear instructions to lower their risk of eDKA, in accordance with Australian Diabetes Society recommendations.21 For prolonged procedures requiring one or more days in hospital, or those using bowel preparations (e.g. for colonoscopy), patients should be instructed to not take their SGLT-2 inhibitor for two days before the surgery and on the day of the procedure (three days in total). For day surgery, such as endoscopy, patients should not take the SGLT-2 inhibitor on the day of the procedure. After the procedure, SGLT-2 inhibitors may be safely restarted after the patient has resumed eating and drinking.21 Withholding combination SGLT-2 inhibitor therapy with metformin or other agents may mean that the patient needs supportive advice on monitoring for hyperglycaemia as a priority.
Sick-day emergencies
Clear written instructions to patients underpin how to detect and manage any life-threatening emergency. An acute rise in blood glucose level to 15 mmol/L or higher for more than eight to 12 hours, with symptoms of emerging metabolic crises, should indicate a potential emergency.
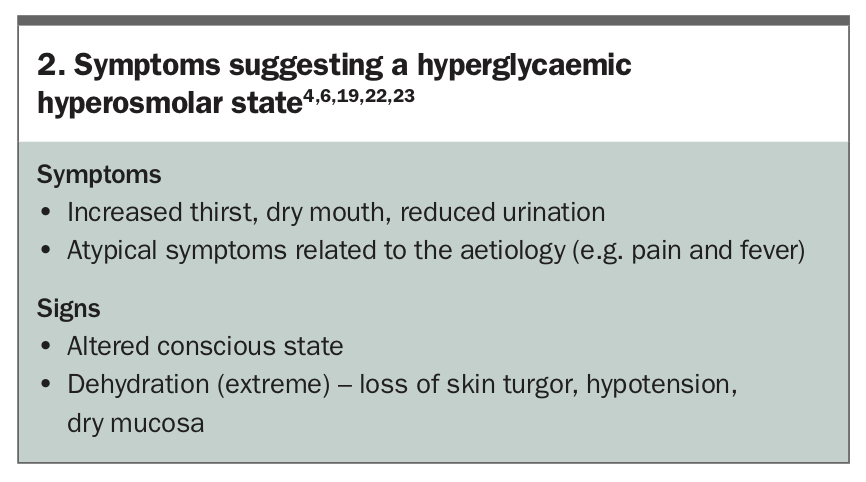
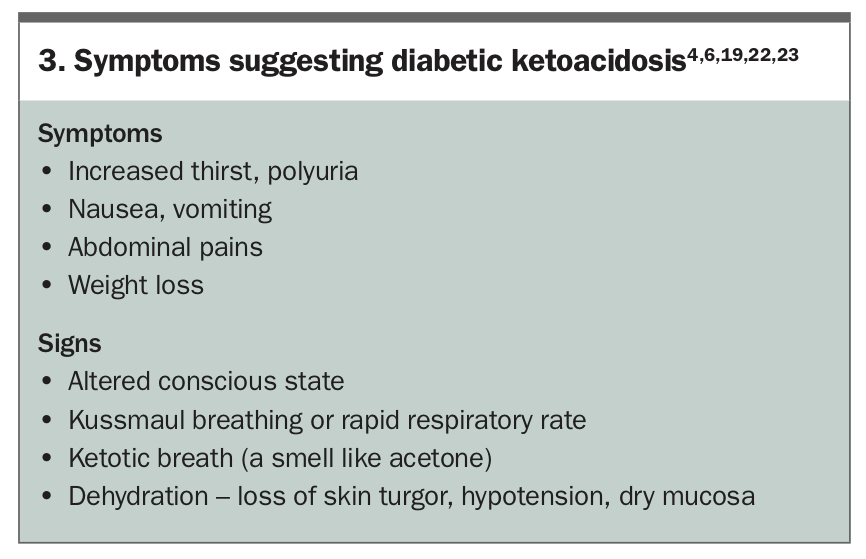
Hyperglycaemic emergencies may evolve into hyperosmolar states without ketosis, often accompanied by severe dehydration, or diabetic ketoacidosis, which may be fatal if inadequately managed.19 The symptoms and signs of these two hyperglycaemic emergencies are shown in Box 2 and Box 3, respectively.4,6,19,22,23 Emergency transfer to appropriate specialist care is imperative in either case.19 Diagnostic criteria for a hyperosmolar state include a plasma glucose level above 33.0 mmol/L, serum osmolality above 320 mmol/kg and no appreciable metabolic acidosis or ketonaemia.2 Diagnostic criteria for diabetic ketoacidosis include a blood glucose level above 11.0 mmol/L, arterial pH below 7.3, serum bicarbonate level below 15.0 mmol/L and ketonaemia (ketones higher than 3.0 mmol/L) or significant ketonuria.2
{kind=link}
{kind=link}
Hypoglycaemia may accompany some sick-day illnesses if food intake is inadequate, especially in patients using sulfonylureas and insulins. If SMBG shows a glucose level below 4 mmol/L, implementation of a sick-day plan is necessary, and action must be taken to address the hypoglycaemia.1 Severe hypoglycaemia, defined as hypoglycaemia requiring the assistance of another person to recover, is an emergency. Importantly, patients should be informed not to drive with a blood glucose level below 5 mmol/L.24
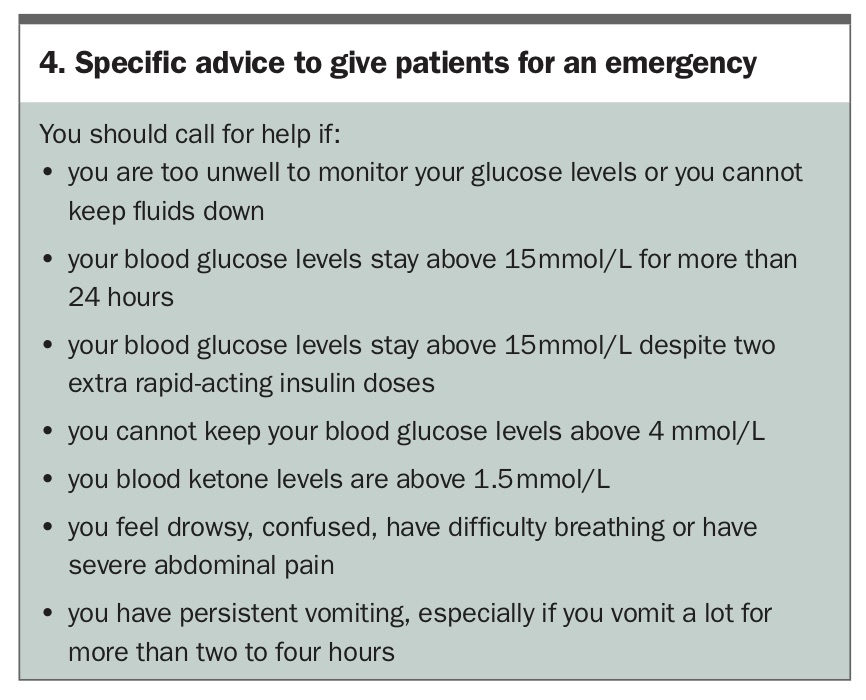
Patients should be advised to call for help in any of the circumstances listed in Box 4. If they feel frightened or unsure or cannot contact a GP, they should either present to an emergency department or call 000.
{kind=link}
Conclusion
The principles of diabetes sick-day management are further elaborated in several RACGP publications, including advice for managing patients with diabetes during the COVID-19 pandemic (Box 1).1,19 Sick-day planning includes diabetes-specific education and any actions that patients need to undertake when they are ill. These plans raise patients’ awareness of the risks and signs of hyperglycaemic and hypoglycaemic emergencies and the important steps needed to proactively deal with any potential problems. Providing patients with a written sick-day management plan and ensuring they have access to advice and support is an investment in avoiding possibly life-threatening complications. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.