An update on GLP-1 agonists: where do they fit in the type 2 diabetes management algorithm?

Diabetes type 2
Diabetes medicines
The cardiometabolic and renal benefits of glucagon-like peptide-1 agonists, and their relatively good safety profile, have rightly positioned them as a candidate for combination therapy in people with type 2 diabetes after metformin in most contemporary management algorithms.
- Glucagon-like peptide-1 (GLP-1) agonists are injectable therapies that exploit endogenous hormonal blood glucose control for people with diabetes.
- GLP-1 agonists have body weight and blood pressure benefits in addition to lowering blood glucose concentrations.
- Some of the analogues in the class have shown reductions in cardiovascular disease and renal benefits in placebo-controlled intervention trials.
- There have been no safety concerns in the intervention trials using GLP-1 agonists, but upper gastrointestinal side effects may limit tolerability in some patients.
GLP-1 and its therapeutic exploitation
Glucagon-like peptide-1 (GLP-1) is a peptide hormone produced by specialised intestinal cells in response to food. It stimulates insulin release in a glucose-dependent manner so that hypoglycaemia does not occur (the incretin effect) and it suppresses glucagon secretion, actions which inhibit hepatic gluconeogenesis.1 GLP-1 also delays gastric emptying and, probably mainly through central nervous system effects, promotes satiety. It has potential cardioprotective effects by reducing inflammation and oxidative stress.1
The therapeutic potential of GLP-1 has been harnessed in two distinct ways. First, there is the gliptin class of blood glucose-lowering therapies that inhibit the dipeptidyl peptidase-4 (DPP-4) enzyme responsible for the rapid metabolism of endogenous GLP-1 and thus increase its circulating concentrations.2 Second, a variety of GLP-1 analogues have been developed that have been designed to protect the molecule against DPP-4 activity.1 These incretin mimetics comprise compounds that are based on either the DPP-4-resistant exendin-4 structure, which has only about 50% homology with human GLP-1, or are more closely (>95%) homologous with human GLP-1 but have used alternative strategies to prolong their half-lives (Table 1).3
{kind=link}
The available GLP-1 analogues can be classified as either short acting with a half-life of a few hours or long acting with a half-life of at least 12 hours.4 The short-acting GLP-1 agonists retain relatively potent effects on gastric emptying because intermittent receptor stimulation avoids tachyphylaxis. The more prolonged exposure to the long-acting analogues is associated with less prandial glycaemic efficacy but greater insulin secretion and thus lower blood glucose concentrations during the post-absorptive period. Nausea is one of the common gastrointestinal side effects of GLP-1 analogue use, especially with the short-acting analogues, but it tends to wane with time.5
Cardiometabolic effects of GLP-1 analogues
The blood glucose-lowering efficacy of the GLP-1 analogues given alone or in combination with metformin is largely comparable with most other therapies for type 2 diabetes. Hypoglycaemia is only a potential issue if GLP-1 analogues are combined with a sulfonylurea or insulin.6 Within the class, however, there are suggestions that the long-acting analogues with greatest homology with human GLP-1 have greater glycaemic potency than the short-acting exendin-4-based compounds.5 The GLP-1 analogues are typically associated with weight loss of 2 to 4 kg in clinical trials and they reduce blood pressure by 2 to 4 mmHg, but they also increase heart rate by 2 to 4 beats/minute.5 They may also have a modest beneficial effect on the serum lipid profile.7
Cardiovascular safety trials involving GLP-1 analogues
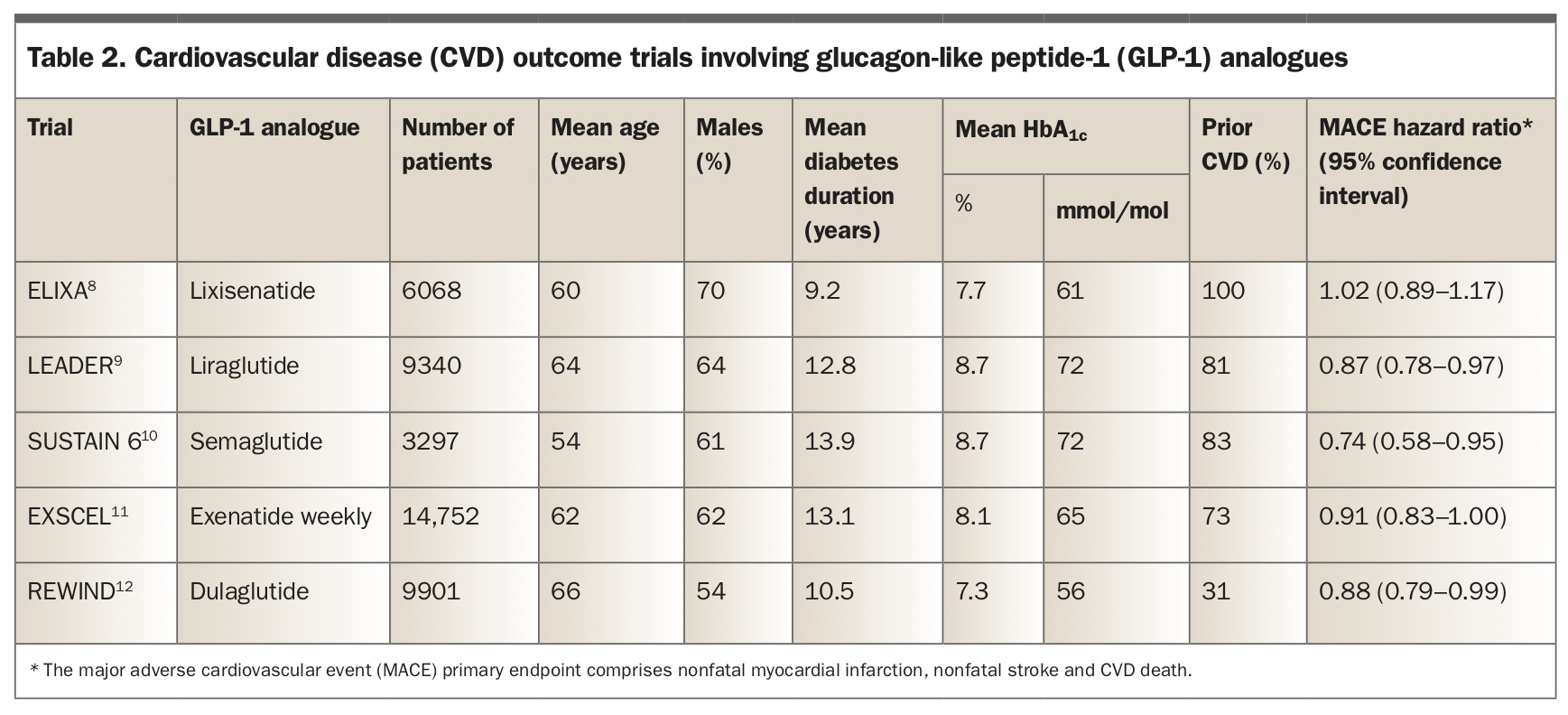
The US Food and Drug Administration requirement for most new blood glucose-lowering therapies to undergo cardiovascular disease (CVD) safety evaluation has resulted in all the GLP-1 analogues, except twice-daily exenatide, having been assessed in long-term placebo-controlled randomised outcome trials (Table 2).8-12 In recent meta-analyses of the five GLP-1 analogue trials shown in Table 2 and two others, there was a significant 13% reduction in major adverse cardiovascular event (MACE) endpoint associated with GLP-1 analogue treatment.13,14 This reduction in MACE, which is not explained by improvements in glycaemia and nonglycaemic cardiovascular risk factors, remains to be fully elucidated but may reflect other effects of GLP-1 analogues such as their antioxidative and anti-inflammatory properties.1
{kind=link}
For the individual MACE components, there were significantly lower and quantitatively similar hazard ratios for nonfatal stroke and CVD mortality, but the hazard ratio for nonfatal myocardial infarction was nonsignificant.13,14 There was no significant difference in MACE in patients with or without prior CVD, whereas the secondary endpoints of heart failure, worsening of renal disease and all-cause mortality were between 9% and 17% lower in those receiving GLP-1 analogue therapy.13 Although preclinical and early clinical utilisation data suggested that medullary thyroid cancer and pancreatitis are increased by use of GLP-1 analogues, more extensive evaluation including through the many large-scale CVD outcome trials has not confirmed these associations.1
In one placebo-controlled trial with semaglutide (Trial to Evaluate Cardiovascular and Other Long-term Outcomes with Semaglutide in Subjects with Type 2 Diabetes [SUSTAIN 6]),10 there was a significant early increase in diabetic retinopathy in patients allocated active therapy, which has been attributed to the rapidity and magnitude of improved glycaemic control (as has been observed in previous studies involving intensive insulin treatment) rather than being a direct adverse drug effect.15
Place of GLP-1 analogues in type 2 diabetes management
The favourable CVD and other outcomes with this class of blood glucose-lowering agents have seen recent changes to treatment guidelines. As is typical for a number of current national and international guidelines, the American Diabetes Association (ADA) and European Association for the Study of Diabetes (EASD)16 recommend that GLP-1 analogues with proven CVD benefit are considered in patients who do not meet individualised glycaemic targets with use of metformin and appropriate lifestyle measures if:
- atherosclerotic CVD is a major concern
- there is chronic kidney disease and sodium-glucose cotransporter-2 (SGLT2) inhibitors are not tolerated or contraindicated, and/or
- there is a compelling need to minimise weight gain and risk of hypoglycaemia in patients without CVD or chronic kidney disease.
Patients with heart failure in whom SGLT2 inhibitors cannot be given are also a group recommended for GLP-1 analogue treatment.16 However, despite the encouraging findings from a recent meta-analysis,13 there was an increase in adverse cardiovascular outcomes in patients with stable chronic heart failure treated with liraglutide versus placebo in a randomised trial, indicating that caution should be exercised in this situation.17 With this caveat, and the fact that GLP-1 analogues are generally not recommended in patients with severe renal impairment (estimated glomerular filtration rate <30 mL/min), the only limitation to their use in the ADA/EASD guidelines is their relative expense.16
Australian guidelines place GLP-1 analogues as a therapy to be considered after metformin as part of combination therapy with oral blood glucose-lowering agents and/or insulin.18 These guidelines cover the PBS restrictions, based largely on cost, to their subsidised prescription with DPP-4 inhibitors (with which there is also a shared mechanism of action and thus potential therapeutic redundancy), SGLT2 inhibitors and thiazolidinediones. There are recommendations that they should be avoided if there is a history of pancreatitis or pancreatic malignancy, as well as mention of dose adjustment in severe renal impairment.18
Conclusion
The GLP-1 analogues are the second class of blood glucose-lowering therapy after the SGLT2 inhibitors to have shown beneficial effects on primary CVD outcomes in large randomised placebo-controlled trials. GLP-1 analogues are all injectable therapies, which may be a drawback for some patients, although oral semaglutide is in development and was recently approved by the US Food and Drug Administration.19,20 However, the cardiometabolic and renal benefits of GLP-1 analogues, and relatively good safety profile, have rightly positioned them as a candidate for combination therapy in patients with type 2 diabetes after metformin in most contemporary management algorithms. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.