Continuous glucose monitoring technology: understanding the benefits

Diabetes medicines
Diabetes complications
Continuous glucose monitoring is an evolving technology that is gradually replacing fingerprick glucose measurements in the management of type 1 and insulin-requiring type 2 diabetes. It provides a complete picture of a patient’s glycaemic pattern, leading to improved diabetes control.
- Unlike self-monitoring of blood glucose (SMBG), continuous glucose monitoring (CGM) provides patients with the opportunity to monitor glucose levels continuously, and to review the trend and rate of glucose changes, which predict impending hypoglycaemia and hyperglycaemia.
- Numerous studies have shown the clinical benefits of improved glycaemic control in patients with type 1 and insulin-requiring type 2 diabetes using CGM compared with SMBG.
- The main barrier to the use of CGM is cost.
- CGM data reporting has been standardised, providing clinicians with a guide for structured interpretation.
- The ‘artificial pancreas’ comprises a CGM system integrated into an automated insulin delivery device.
Improved glycaemic control is the key factor in preventing long-term complications of type 1 and type 2 diabetes.1,2 Optimisation of glycaemic control, particularly when implemented by intensive insulin therapy, is challenging. The main limiting factors for intensive therapy include the need for frequent self-monitoring of blood glucose (SMBG) and the risk of hypoglycaemia.
Traditionally, measuring glycated haemoglobin (HbA1c) levels and SMBG have been the main methods for assessing glycaemic control. However, these methods do not provide a complete glycaemic profile and, in particular, provide limited information about glucose excursions, the trend of glucose changes and unrecognised hypoglycaemia, especially nocturnal hypoglycaemia. In the past decade, continuous glucose monitoring (CGM) technology has been developed as a novel tool to address many limitations of using HbA1c levels and SMBG. CGM technology has revolutionised diabetes therapy and has become central to state-of-the-art management of type 1 and complex type 2 diabetes.
Limitations of HbA1c and SMBG
HbA1c level is a benchmark for evaluating overall glucose control and predicting the risk of long-term complications. It is reflective of the approximate average glucose level for the past three months, but it does not provide any information about glucose fluctuation, otherwise known as glycaemic variability. It also does not provide information about the frequency and timing of hypoglycaemic and significant hyperglycaemic events. HbA1c may be misleading and inaccurate in the context of low or high red blood cell turnover, including iron or vitamin B12 deficiency, end-stage chronic kidney disease and during pregnancy.3 Therefore, HbA1c alone is not a reliable marker for personalising intensive diabetes management, particularly with regard to adjusting insulin dosing.
The introduction of SMBG in the 1970s was a major adjunct in diabetes management. However, SMBG has significant limitations when it comes to intensive insulin therapy. Frequent SMBG is commonly required in patients with type 1 diabetes or insulin-requiring type 2 diabetes for optimal glucose monitoring. As it requires a finger prick to get a capillary blood sample, the associated pain and inconvenience may limit adherence to this type of monitoring regimen. It also may not be feasible to do at work, school or while driving. Furthermore, SMBG provides only a snapshot of the blood glucose level at the time of testing without providing any data regarding the direction or rate of glucose changes. Relying purely on SMBG may result in failure to recognise asymptomatic and nocturnal hypoglycaemia.
Continuous glucose monitoring
Unlike SMBG, CGM provides patients with the opportunity to monitor glucose levels continuously and to review the trend and rate of glucose changes, which predict impending hypoglycaemia and hyperglycaemia. Some CGM systems also have customisable hypoglycaemia and hyperglycaemia alarms.4-6 The real-time information provided by CGM can provide feedback about the effect of insulin administration as well as fluctuations of glucose levels in response to diet, exercise and daily activities. Analysis of CGM data by both the patient and healthcare provider enable them to better understand the glycaemic pattern during the day and night and help to identify otherwise unrecognised hypoglycaemia (particularly overnight) and hyperglycaemia. This insight will then help to make meaningful insulin dose adjustment as well as lifestyle and behavioural modifications to improve glycaemic control and to prevent hypoglycaemic and significant hyperglycaemic events.
Current CGM systems
A CGM system comprises three components:
- a glucose sensor that is inserted into the subcutaneous tissue (usually either the arm or abdomen) and measures glucose concentration in interstitial fluid
- a transmitter that is attached to the glucose sensor
- a receiver or reader that receives, stores and displays the continuous glucose data.
The reader can be a standalone device, an application on a smartphone or smart watch, or an insulin pump. There is an advanced algorithm within the CGM system that extrapolates interstitial fluid glucose concentration measured by the sensor to actual blood glucose level. These systems therefore mostly require calibration with daily fingerpick blood glucose measurements to maintain accuracy. Sensors are worn for one or two weeks before being replaced, depending on which system is being used.
There are two forms of CGM systems currently available: real-time CGM (RT-CGM) and intermittently viewed CGM, otherwise known as flash glucose monitoring (FGM). RT-CGM displays numerical and graphical glucose data continuously in real time as well as the trend of glucose changes. Currently available RT-CGM systems in Australia are Dexcom G4 Platinum, Dexcom G5 Mobile, Dexcom G6, and Medtronic systems including Guardian Connect, Guardian Link and Minilink.
FGM comprises a combined glucose sensor/transmitter inserted into the user’s upper arm. The receiver is either a reader device or a smartphone application. When the user scans the reader or smartphone over the sensor, the immediate glucose level at the time of scanning as well as the past eight-hour glucose trend are displayed. Unlike RT-CGM, which continuously displays the glucose information and has programmable alarms, FGM only shows the glucose level when the patient scans the reader over the sensor and lacks the high or low glucose alarms. The only FGM system that is currently available is the FreeStyle Libre (Abbott Diabetes Care). This is a factory-calibrated glucose monitoring system that does not require calibration with capillary glucose measurements.
Clinical benefits of CGM
Numerous studies have shown greater clinical benefit of CGM compared with SMBG with regard to improved glycaemic control.7-13 The main observed benefits were decreased HbA1c levels, increased time spent in the target glucose range (4 to 10 mmol/L), reduced time spent in the hypoglycaemic range and decreased glycaemic variability. The benefits were observed in patients with type 1 diabetes regardless of whether multiple daily insulin injections or an insulin pump were used. A meta-analysis showed that CGM was associated with a 0.3% reduction in HbA1c and a 23% reduction in exposure to hypoglycaemia compared with SMBG.9
Benefits of CGM have also been reported in patients with type 2 diabetes, with HbA1c levels reduced by 0.2 to 0.3% and time spent in hypoglycaemia reduced by 43%.12,14-16 Evidence is limited, however, regarding CGM use in patients with type 2 diabetes who are not on insulin and women with gestational diabetes. CGM contributes to significant improvement in diabetes-specific quality of life markers including diabetes distress, sense of control over diabetes and confidence in managing and avoiding hypoglycaemia.17,18
Limitations and barriers of CGM use
The main barrier to the use of CGM is cost. In Australia there is limited government support available for some patients with type 1 diabetes through the National Diabetes Services Scheme (information available online at www.ndss.com.au/living-with-diabetes/managing-diabetes/continuous-glucose-monitoring); however, many patients are out of pocket several thousand dollars per year for full-time CGM use.
Accuracy and reliability are also limitations, as CGM measures interstitial fluid glucose levels rather than blood glucose levels. There is a lag of five to eight minutes after the blood glucose level changes and glucose equilibrates between the intravascular and interstitial spaces. The lag is greatest when glucose levels change rapidly (for example after ingesting a meal or administering short-acting insulin). For this reason, regular calibration is necessary for most CGM systems, and fingerprick checks should be performed when accuracy is in doubt. CGM accuracy has significantly improved over recent years, however, and the newest generation of continuous glucose monitors have a mean absolute relative difference of less than 10% compared with the matched reference glucose measurement.
CGM data interpretation
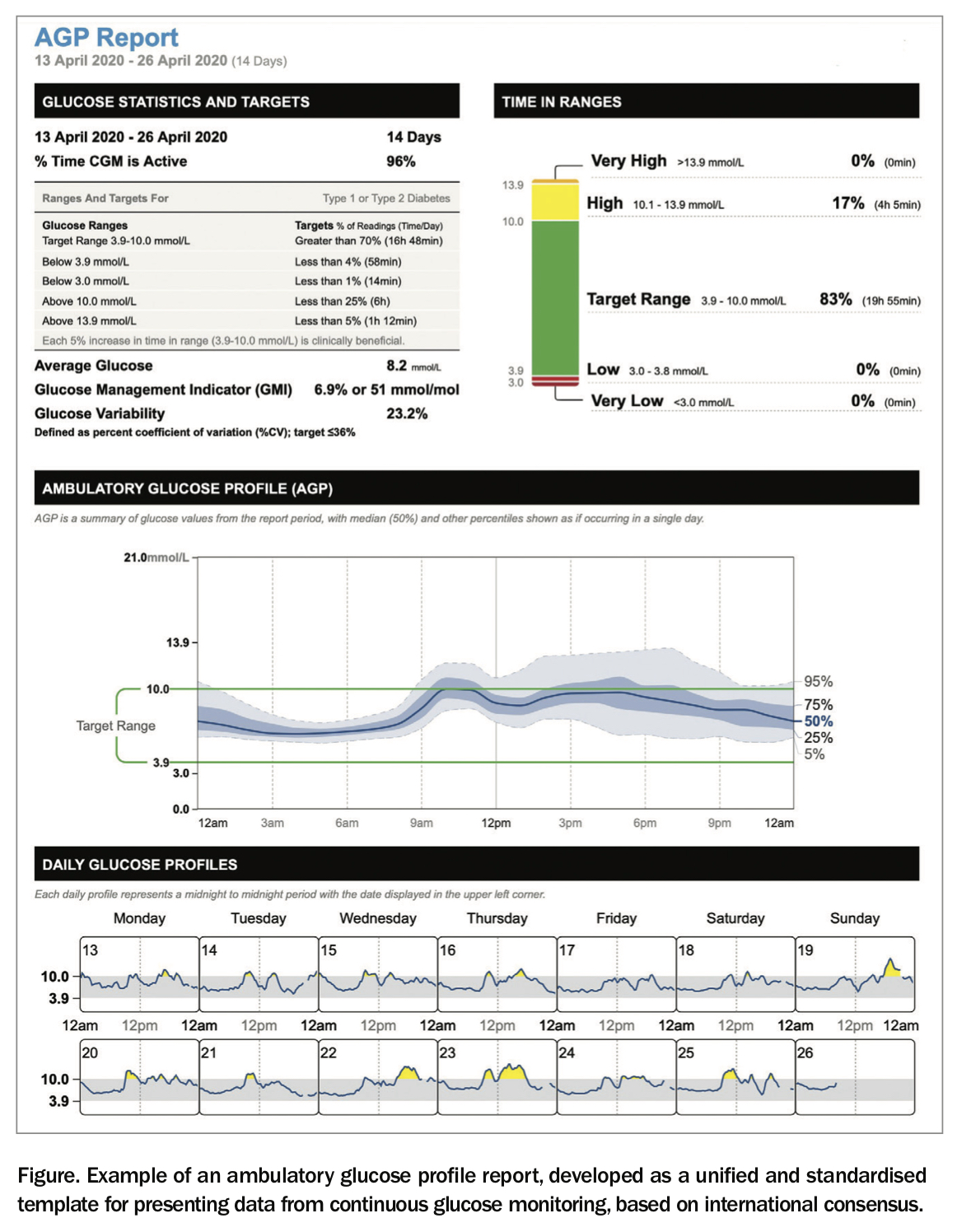
CGM provides a large amount of data that requires structured interpretation. There are now international guidelines and consensus on standardisation of CGM metrics and CGM report visualisation. The ambulatory glucose profile (AGP) has been developed as a unified and standardised template for CGM data presentation and provides a clear overall picture of globally accepted CGM metrics including time in range (percentage of time spent in the target glucose range of 3.9 to 10 mmol/L), time above range, time below range, estimated HbA1c (known as glucose management indicator, or GMI), glucose variability, a graphical display of median glucose level, and day-to-day individual data (Figure).19,20
{kind=link}
CGM does not represent an intervention in itself, but provides the opportunity for the information supplied by the device to be used to optimise diabetes management, which is important. Structured training and education of both clinicians and patients is therefore crucial to enable interpretation of the CGM data and translation of the information into individual diabetes management.
Future developments
Newer generations of CGM systems are factory calibrated, eliminating the need for calibration with a fingerprick capillary glucose level. Additionally, with improvement of the glucose sensor accuracy, integration into automated insulin delivery devices is more feasible. This will be a major step in improving functionality of closed-loop insulin delivery systems (otherwise known as artificial pancreases), which comprise a CGM system integrated into an automated insulin delivery device. Implantable glucose sensors with approval for use for up to six months have been developed and are available in some countries. These remove the need for regular replacement of sensors and are likely to improve outcomes in patients for whom wearing an external device is difficult, such as those engaging in contact sports. Eversense CGM is the first of these and may become available in Australia soon.
Conclusion
Just as SMBG revolutionised the management of diabetes, CGM has changed our understanding of the management of type 1 and insulin-treated type 2 diabetes. CGM gives a more comprehensive picture of glycaemic control by providing information regarding day and night glucose patterns, glucose excursions and nocturnal hypoglycaemia, which are not captured by measuring HbA1c levels and SMBG. This leads to a more accurate assessment of glycaemic control and more personalised therapeutic decisions. CGM should be considered in all patients with type 1 diabetes and patients with type 2 diabetes on multiple daily insulin injections, particularly those with frequent hypoglycaemia or impaired hypoglycaemic awareness. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.