Testosterone replacement therapy: a practical guide to initiation and monitoring

Men's health
Endocrine diseases
Several preparations of testosterone are available but the key factors in determining the most suitable preparation are convenience, ease of administration and safety for the individual. Testosterone replacement therapy should not be prescribed until the diagnostic work up is complete.
- A thorough work up should be completed before commencing testosterone replacement therapy (TRT) to determine the underlying cause of androgen deficiency.
- Men with proven androgen deficiency, in the absence of contraindications, should be offered TRT.
- The choice of testosterone preparation will reflect the individual’s concurrent medical history and personal choice.
- Fertility plans of all men should be discussed before commencing TRT. TRT suppresses spermatogenesis and the duration of this effect varies depending on the formulation used.
- Monitoring of testosterone levels in men receiving TRT will differ according to the preparation prescribed.
Testosterone is essential for male sexual differentiation and spermatogenesis. Physiological testosterone levels vary during distinct phases of life and plateau in adulthood. Longitudinal studies suggest a 1 to 2% decline per annum in testosterone levels from the fourth decade onwards, although much of this decline is related to comorbidities.1-3 Indeed, healthy men may maintain testosterone levels within the healthy young male normal range into their seventh decade.2,4
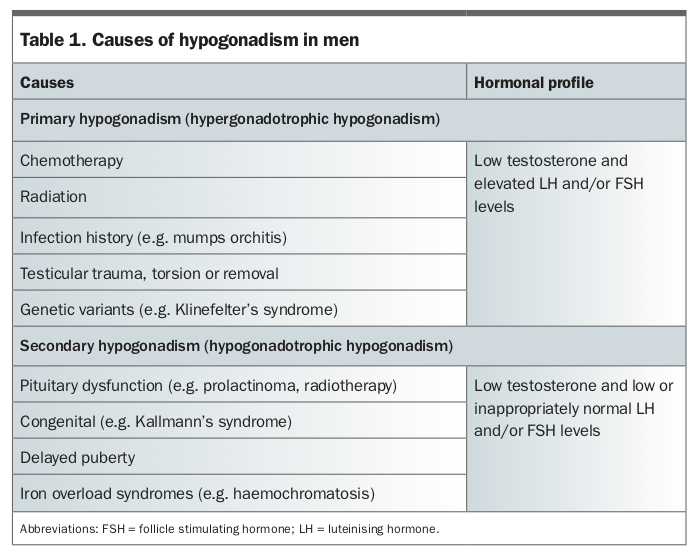
Testosterone deficiency may be congenital or acquired at any time in a man’s life. It is generally classified as either primary or secondary hypogonadism, with the causes outlined in Table 1. Primary hypogonadism is related to testicular failure and characterised by a low testosterone level and compensatory rise in luteinising hormone and follicle stimulating hormone levels. Secondary hypogonadism is due to hypothalamic or pituitary dysfunction, and luteinising hormone and follicle stimulating hormone levels remain low or ‘inappropriately’ normal in the setting of low testosterone levels.
{kind=link}
Diagnosis of hypogonadism
To determine both the presence of testosterone deficiency and its underlying cause, clinicians should undertake a careful initial clinical assessment by history taking and examination, which should include testicular examination with an orchidometer. Testosterone measurement is key to the diagnosis and should be measured early in the morning and on fasting, ideally using a liquid chromatography/mass spectrometry platform to avoid the variability seen with immunoassays.5,6 It is recommended that this measurement is carried out at least twice, two to four weeks apart and with accompanying gonadotrophin measurements to interpret the potential pathogenesis. The causes of testosterone deficiency should also be screened for (Table 1), including iron studies and karyotype testing if clinically indicated. In hypogonadotrophic hypogonadism, pituitary profile evaluation should include prolactin measurements and pituitary imaging.
For the purposes of current PBS-subsidised testosterone prescribing in men without testicular or pituitary pathology, androgen deficiency is defined as: testosterone level less than 6 nmol/L; or testosterone level between 6 and 15 nmol/L with luteinising hormone level either 1.5 times the upper limit of normal range or greater than 14 IU/L. There are no qualifying testosterone levels for men with established testiscular or pituitary disease.
Testosterone replacement therapy
The increasing number of prescriptions being written for testosterone in Australia and the concern over safety in men without clear indications for the medication has led to tighter regulation of the PBS criteria for eligibility of subsidised testosterone in men. Testosterone replacement therapy (TRT) should never be commenced before the diagnostic work up is complete. Failure to undertake a full evaluation before TRT may overlook the underlying aetiology and will suppress the endogenous hypothalamic–pituitary–testicular axis making further evaluation difficult.
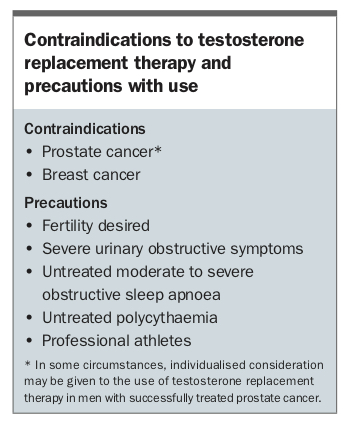
The use of TRT for men with hypogonadism presumes a requirement for lifelong therapy, and men should be committed to this only when it is appropriate clinically. An updated comprehensive position statement for the evaluation of hypogonadism and use of testosterone in men was recently published by the Endocrine Society of Australia.7,8 There are no proven clinical benefits for TRT in men without pathological hypogonadism, and indeed there are safety considerations including cardiovascular concerns that should preclude its use unless warranted clinically. The contraindications and precautions for use of TRT are outlined in the Box and these should be evaluated before prescribing testosterone.
{kind=link}
Fertility considerations
It is recommended that the fertility plans of all men should be discussed and documented before commencing TRT. Exogenous testosterone suppresses spermatogenesis and the duration of this effect may vary depending on the formulation used.9 For example, intramuscular testosterone undecanoate (Reandron) is suppressive for many months after its last administration.
It is also worth considering the fertility options available to men depending on the underlying cause of hypogonadism. Sperm banking before men have cytotoxic therapy is well established. Current experience in fertility options for men with Klinefelter’s syndrome is evolving, with recent emerging evidence of the potential for fatherhood.10 For men with hypogonadotrophic hypogonadism, gonadotrophin therapy is used for the induction of spermatogenesis and should be carried out under the guidance of a reproductive endocrinologist or andrologist.11 For men in these groups who desire children and are receiving a long-acting TRT preparation, changing to a short-acting TRT preparation for up to one year may be necessary before receiving gonadotrophin treatment or if considering testicular sperm extraction (e.g. in men with Klinefelter’s syndrome). This should be carried out in conjunction with reproductive specialists, depending on the underlying pathogenesis.
Finally, the use of TRT for pubertal induction should only be undertaken by those experienced in this aspect of androgen prescribing such as paediatric endocrinologists or andrologists.
Goal of testosterone replacement therapy
For men with established hypogonadism requiring treatment, the aim of TRT is to replicate endogenous hormone ranges such that androgen-dependent tissues are exposed to physiological levels. Many studies have demonstrated that restoration of testosterone levels in hypoandrogenic men improves libido, bone mineral density and metabolic parameters, particularly lipid profiles, increases lean muscle mass and reduces fat mass.12,13 The psychological impacts of androgen deficiency, such as depression, low mood and general wellbeing, are also improved.
Tailoring testosterone preparation to the individual and monitoring therapy
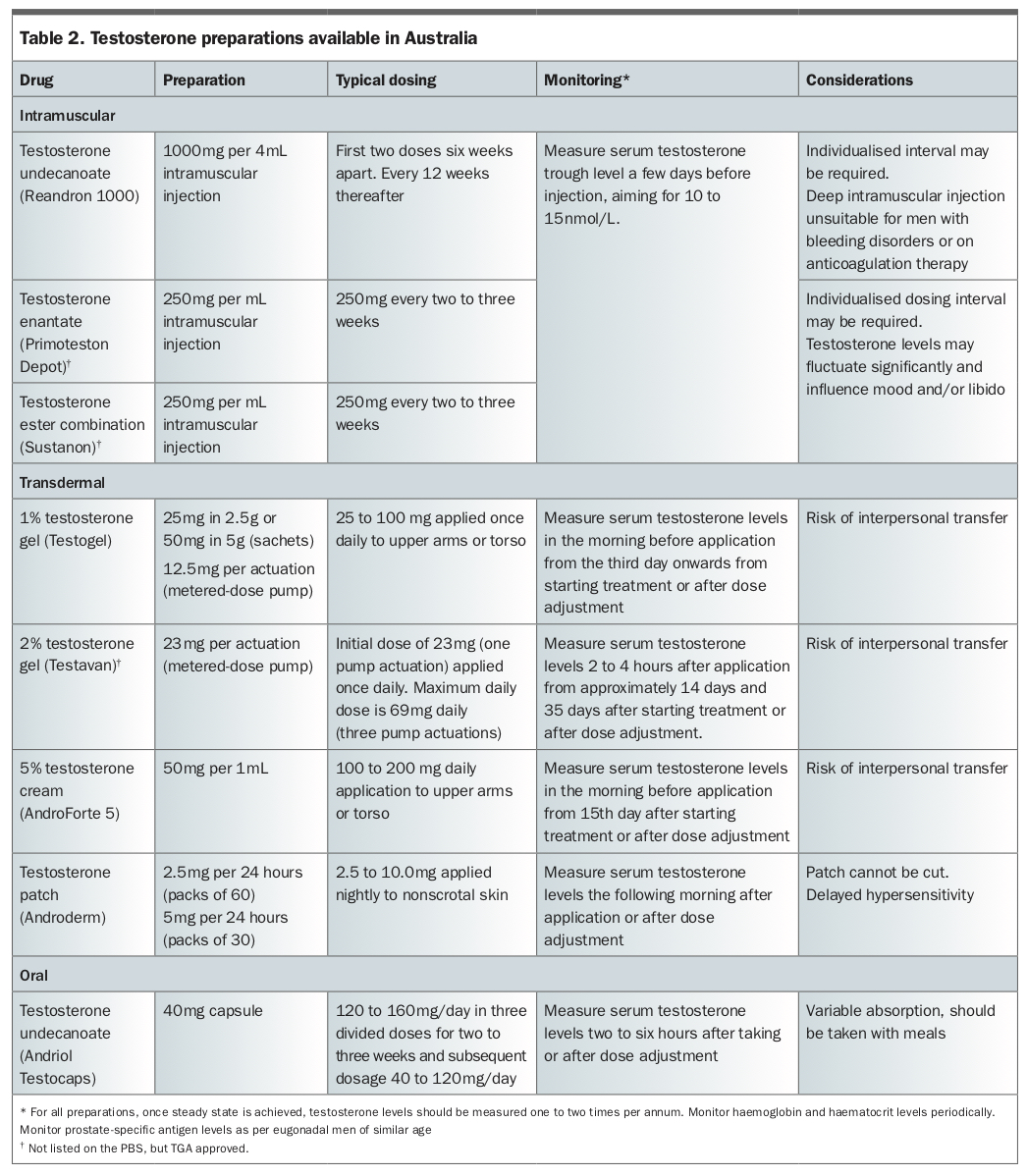
Several testosterone preparations are available to patients and clinicians, as summarised in Table 2. Convenience, ease of administration and safety for the individual are key factors in determining which formulation is preferred. When monitoring the efficacy of TRT, it is necessary to appreciate the pharmacokinetics of the formulation used and the timing of the last dose to evaluate steady-state serum testosterone levels. This is discussed for each preparation below.
{kind=link}
Injectable testosterone
Injectable testosterone preparations vary in terms of their duration of action. Testosterone esters (Primoteston Depot, Sustanon) can be administered every two to three weeks, and patients can be taught to self-inject. Trough serum testosterone levels should be measured a few days before the next injection is due to guide the dosing interval. However, the pharmacokinetic profile can result in supraphysiological testosterone levels, followed by a relatively rapid decline, which can cause fluctuations in libido or mood in some men and increase the risk of polycythaemia.
Intramuscular testosterone undecanoate (Reandron 1000) is a long-acting preparation of approximately 12 weeks’ duration. It is administered slowly in a deep intramuscular injection and is a safe and efficacious means of TRT delivery, requiring approximately four to five injections annually.14-16 A rise in haematocrit levels may limit the dosing interval. As it is a deep intramuscular injection, it is not recommended in anticoagulated men or those with bleeding disorders.
In clinical practice, eugonadal testosterone range is achieved and maintained in most men receiving testosterone undecanoate. However, this therapy does exhibit individual differences requiring titration of the interdose frequency according to symptoms and haemoglobin, haematocrit and trough testosterone levels to achieve the optimal dose interval for each patient.
After initiation of therapy (1000 mg dose) at baseline and at week six, testosterone levels should be measured before the week 30 injection. The aim of treatment is to readminister intramuscular testosterone undecanoate before symptomatic androgen deficiency recurs and when testosterone levels fall into an appropriate range before the next dose. This range will differ according to factors including age and comorbidities but is usually in the lower half of the eugonadal range. For most men 12 to 14 weeks is a consistent and predictable interval for ongoing injections, but there can be a marked interindividual variation. Monitoring for polycythaemia along with the nadir testosterone level also allows individualisation of dosing interval. Men with concurrent obesity or obstructive sleep apnoea or those who smoke may be more likely to have elevated haematocrit levels and require lower dosing or longer intervals between doses.
Transdermal testosterone
Testosterone gel is applied daily to intact dry skin of the torso and upper arm for absorption and more closely mimics the diurnal rhythm of endogenous testosterone. Serum testosterone levels rise from two hours after application and a steady state is generally achieved 48 to 72 hours after daily application. Peak absorption occurs within two to four hours after application, and testosterone levels should be measured in that timeframe. This preparation is easily reversible with a return to baseline within four days of ceasing treatment.12,17 Skin irritation has been reported with an incidence of up to 7%, although this is rarely so severe as to cause discontinuation of treatment.18 As the gel remains on the skin for several hours, men should cover up with clothing and not shower or swim for four to six hours post application. Patients must be educated by the prescriber to avoid interpersonal transfer of the preparation through skin to skin contact with children, sexual partners and women.19 A 1% preparation is available (Testogel) and a 2% formulation (Testavan) has recently been approved by the TGA.
Only one testosterone cream preparation (AndroForte 5) is approved by the TGA for use in Australia. It is applied to the torso with the usual starting dose being 2 mL of cream (100 mg of testosterone) daily, with a dosing range of 2 to 4 mL daily. It is supplied with a metered syringe for dosing.
A testosterone patch (Androderm) requiring daily application is also approved by the TGA for use in Australia. These patches are available in two strengths (2.5 mg per 24 hours and 5 mg per 24 hours), which can present challenges in dose titration for some men. The patch consists of a reservoir containing testosterone with a permeation-enhancing vehicle and gelling agents. Although these patches achieve adequate serum testosterone levels and are clinically efficacious, up to 66% of men develop skin hypersensitivity at some time during therapy with consequently poor continuation rates.20 It is recommended that these patches are applied to intact skin in the late evening and testosterone levels should be measured the following morning.
Oral testosterone
Testosterone undecanoate (Andriol Testocaps; 40 mg capsules) can be taken orally, but it is necessary to take it two to three times a day and with a fat-containing meal to aid absorption.21,22 There can be marked fluctuations in serum testosterone levels, which should be measured two weeks after initiation, two to six hours after ingestion. Compliance, adherence and pill burden can be major barriers to achieving adequate serum testosterone levels.
Other considerations
It is important to consider reversibility of preparations. Intramuscular testosterone undecanoate will take weeks to months to wear off. In men with long-standing androgen deficiency, a topical preparation in the first instance is useful to assess tolerability, and longer-acting preparations can be offered when it is established that men tolerate a gradual achievement of eugonadal testosterone levels.
Elevation in haematocrit levels is common in men receiving testosterone and, along with measurement of serum testosterone levels, men should be monitored for polycythaemia. Deep intramuscular injections should be avoided in therapeutically anticoagulated men and those with bleeding disorders.
The incidence of prostate cancer increases with age and therefore judicious use of intramuscular testosterone undecanoate is advised in older men in whom an intercurrent diagnosis of prostate disease may be more likely, although there is no evidence that testosterone treatment initiates prostate cancer. This applies to both men who are commencing TRT and those who are considering a change in the modality of testosterone application.
Combining specialist input with GP care
Men receiving TRT should attend specialist appointments periodically to support ongoing assessment to ensure the testosterone preparation and doses are maintained at safe and efficacious levels and are continuing to meet the patient’s clinical needs and personal circumstances. When patients are stable on a dosing regimen, shared care between the GP and the endocrinologist, urologist or sexual health physician can be advantageous. As the primary care provider, the GP is well placed to use reviews for testosterone prescriptions as an opportunity to address other aspects of men’s primary health care. These include monitoring of blood pressure, weight, mental health, sexual function and prostate health as well as periodic assessment of lipid and blood glucose levels, obstructive sleep apnoea and bone mineral density, if clinically indicated.
Conclusion
Testosterone is a safe and effective therapy for men with proven androgen deficiency due to testicular or pituitary disease. The choice of preparation will reflect personal choice taking into consideration the man’s medical history. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.