The ‘AIDS’ acronym: identifying causes of hyperglycaemia in type 2 diabetes

Diabetes type 2
Diabetes medicines
When an individual with type 2 diabetes presents with a chronic deterioration in blood glucose levels the healthcare professional who manages them must consider a broad range of issues that may be causing the clinical picture. This article describes a helpful acronym that has been developed to enable systematic consideration of the causes of the hyperglycaemia.
- Many causes of persisting or deteriorating hyperglycaemia in patients with type 2 diabetes are easily identified.
- The AIDS acronym is a tool to help systematically target the cause(s) of deteriorating blood glucose levels and to improve patient outcomes.
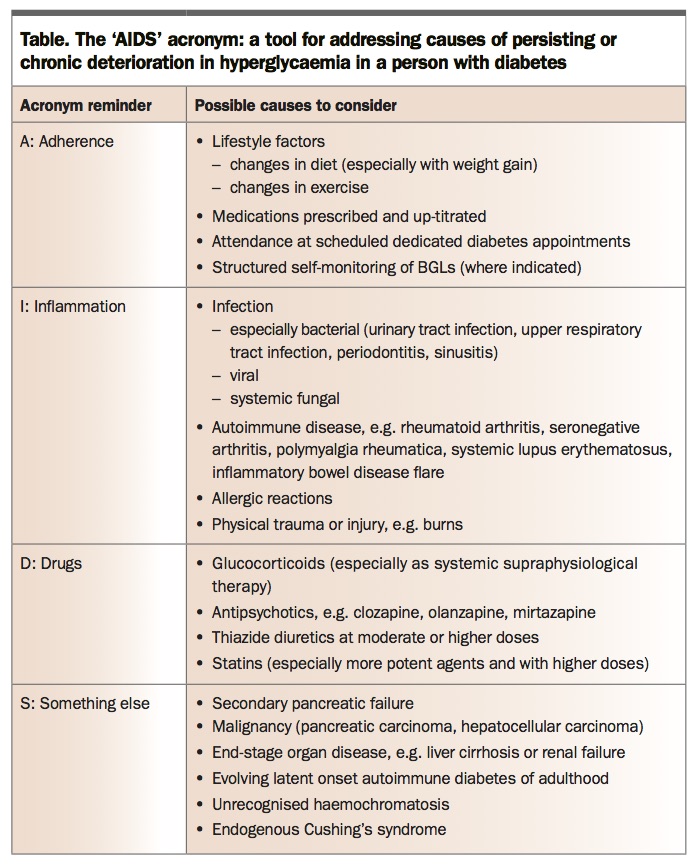
- Areas covered by the acronym are adherence, inflammation, drugs, and other causes grouped as ‘something else’ and including cancers, progressive kidney disease and liver impairment, incorrect diabetes subtype characterisation and ‘secondary failure’ of pancreatic beta cells.
- Adherence is a broad area of care, including nutrition and exercise, patient attendance at appointments, medication adherence and glucose monitoring in those who require it.
Picture credit: © Charles Milligan/Medical Images Models used for illustrative purposes only
The updated type 2 diabetes blood glucose treatment algorithm, as a collaborative document from the Australian Diabetes Society, the National Prescribing Service, Diabetes Australia and the Royal Australian College of General Practitioners, was released about a year ago (Figure).1 As a summary guideline, it helps healthcare professionals in managing individualised blood glucose care in patients with type 2 diabetes. It provides a flow diagram approach, outlining the preferred first-line agents to treat this condition and recognising the common need for subsequent, additional agents and cessation of medicines that may be ineffective in some patients.
{kind=link}
Whenever a person with type 2 diabetes is seen for a medical consultation, important overall issues include establishing their current glycated haemoglobin (HbA1c) target. Depending on the individual profile of the patient, including their comorbidities, diabetes duration and chronological age, the HbA1c target could be anywhere from 42 mmol/mol (6.0%) up to 64 mmol/mol (8.0%). When a palliative approach to patient care is undertaken, with only conservative monitoring of blood glucose levels (BGLs) required, there may be no HbA1c target. For example, a person with dementia in institutionalised care needs BGLs that will avoid symptomatic hypoglycaemia or hyperglycaemia, rather than a particular HbA1c target. In most cases, the HbA1c target is set for the patient, then therapy is instituted to achieve and then maintain HbA1c levels.
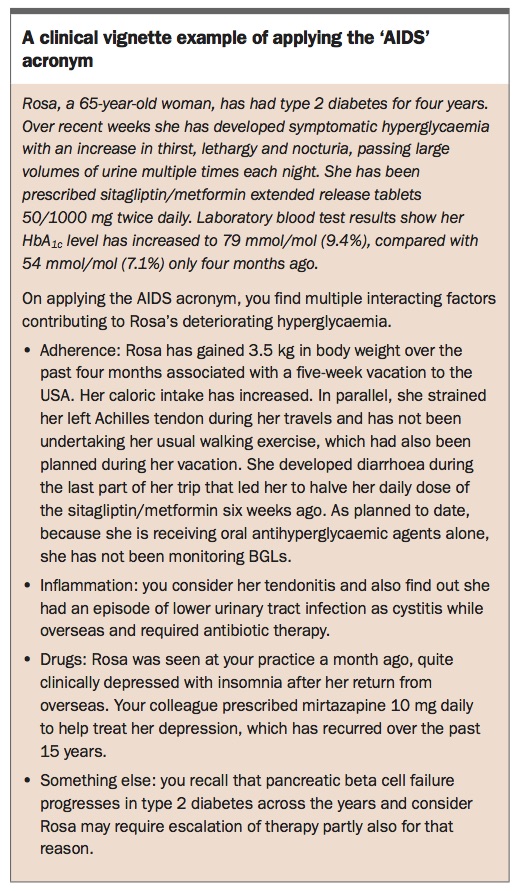
Persisting hyperglycaemia is frequently encountered in both primary and tertiary care settings. The blood glucose management algorithm includes advice about factors to consider when a patient’s BGLs are above target. However, although many causes are easily identified, we and our diabetes colleagues thought it would be helpful to have a tool to ensure all causative factors for deterioration in control of blood glucose levels are considered when in consultations with patients. We developed the ‘AIDS to the blood glucose algorithm’ acronym as a tool to provide a structured approach to this common clinical issue (Table). The acronym can be easily recalled and applied. Implementing this tool as described in this article will help healthcare professionals to ensure less common or obscure precipitants are not overlooked as contributing factors. A clinical case vignette is given in the Box as an example of the acronym in action.
{kind=link}
The AIDS acronym
A: Adherence
For patients with type 2 diabetes, the broad issue of adherence relates to lifestyle management (nutrition and exercise), patient attendance at appointments, medication adherence and glucose monitoring in those who require it. Adherence is greater among patients who are actively engaged in self-care and helps them achieve better glycaemic and overall outcomes.
There are many components to the adherence part of the acronym. A ‘sub-acronym’ that may be a helpful for remembering its parts is ‘GAMED’: glucose, attendance, medication, exercise and diet.
Glucose
In recent years in Australia it has been more clearly confirmed which patients with diabetes will benefit from glucose monitoring. This includes both capillary blood glucose monitoring and, in some cases, interstitial monitoring with glucose monitoring systems. The people who benefit most are those receiving insulin therapy and, for safety purposes, people receiving sulfonylurea oral agents.Some real-world large data sets demonstrate that people who more frequently monitor their capillary or interstitial BGLs across a day have more tightly controlled HbA1c levels.2-4 However, monitoring should be structured and specifically targeted to aid adjustments of therapy in a systematic manner across the day so the HbA1c level can be improved and hypoglycaemia minimised. Although the need for glucose monitoring in patients with type 2 diabetes must be individually assessed, in general in those for whom it is recommended, more frequent daily structured monitoring is associated with improved glycaemic outcomes. In contrast, asking the person to mindlessly monitor their BGLs every day without any change in behaviour or medication is not helpful.
Attendance
It is important that people with type 2 diabetes maintain their appointments with healthcare professionals. In our experience, considering the pressures on the healthcare system and the large number of people with type 2 diabetes, these appointments are made in a judicious manner. Data from domestic and international sources increasingly indicate that people with diabetes who do not attend their ambulatory care appointments, either in primary care or specialist settings, have much higher prospective attendant morbidity and mortality.5 It is important for healthcare services to spend time following up patients who do not attend their appointments, to determine how to support and motivate them to do so subsequently. One strategy for the person who says, ‘Nothing was going well, so I didn’t want to see you’ is to respond, ‘When things aren’t going well is exactly when I want to see you, so we can work together to improve things. You will not be judged, as I understand it is tough self-managing your diabetes every day’.
Medication
Some studies indicate that up to 50% of people with diabetes do not take their medications as prescribed. Data from randomised controlled trials indicate that adherence to medication taking is especially important in type 2 diabetes.6
The Look Ahead study in people with morbid obesity and type 2 diabetes focused on weight loss and essentially did not show improved cardiovascular outcomes.7 However, series of studies have shown improvements in preventing microvascular and in some cases macrovascular outcomes in patients taking medication for type 2 diabetes. These include the landmark studies of the United Kingdom Prospective Diabetes Study and its post-study monitoring.8,9
More recent studies targeting glycaemic control have indicated that microvascular complications can be prevented through the medicines used in blood glucose management. These include the ADVANCE study and the ACCORD study.10,11 The latter also reminds us that excessively intensifying glucose management in individuals at high risk for cardiac events can lead to adverse mortality outcomes.
Thus, adhering to regimens of appropriate blood glucose management using targeted medicines, as well as targeting blood pressure and lipids with appropriate medicines, can markedly improve outcomes for people with type 2 diabetes. This combined approach is best exemplified in the study known as STENO-2, where combined tight blood pressure, lipid and blood glucose management in people with albuminuria, realised mainly through medication approaches, reduced adverse microvascular and macrovascular outcomes.12
Adherence to ambulatory insulin administration has its own particular challenges in people with type 2 diabetes. Many people do not self-administer all prescribed injections, and determining this can be difficult. When a patient’s lack of adherence is revealed, a frank exploration of the reasons for it is needed. Reasons may include discomfort in self-injecting, forgetfulness, clinical depression, fear of hypoglycaemia and/or concern about weight gain. Effort will then be required to address the causes of reduced adherence to improve clinical outcomes.
A trap that many health professionals and patients fall into in responding to nonadherence is to increase the medication dosages. Subsequently, when the person does adhere to taking their medicine as prescribed and regularly, they experience hypoglycaemia. This can lead to further nonadherence as a means of avoiding hypoglycaemia. Therefore, a critical clinical point during every consultation is to ask, in a nonjudgemental manner, about the person’s adherence to their prescribed medicines.
Exercise and diet
Most people with type 2 diabetes are overweight or obese, with caloric excess contributing to susceptibility for developing the condition. Reducing caloric intake to achieve and sustain weight loss is difficult to achieve generally, and in particular in people with type 2 diabetes. One cause of a deterioration in BGLs and a corresponding increase in HbA1c level is progressive weight gain. The type and daily amount of macronutrients ingested plays a major role in weight gain, especially intake of fat, which is calorie dense, as well as rapidly absorbed carbohydrate in sweetened soft drinks, fruit and fruit juice.
Most adults in Australia do not achieve the recommended level of at least 150 minutes of moderate intensity exercise (brisk walking or equivalent) per week, spread across three or more days. Adherence to recommended exercise levels tends to be suboptimal in people with type 2 diabetes in particular, because clinical depression and physical comorbidities such as osteoarthritis often contribute to nonadherence. People who are able to transiently achieve recommended exercise thresholds often lose continuity across months, due to tendon injury, muscle strain or during a vacation when they are out of routine, for example. Series of randomised controlled trials have shown that regular exercise can improve the HbA1c level by about 0.3 to 0.5%; however, data also suggest that loss of a regular exercise routine results in worsening BGLs.13,14
In treating a person who is inactive, encouraging them to start out small with only five minutes of activity and to build from this can be a successful strategy. In our experience, telling a person they need to do 150 minutes of activity per week and achieve a normal body mass index is a strategy often doomed to failure. Work with the person, finding out what they are prepared to do, and then encourage them to do it. If they do not achieve their goals, avoid words that make them feel guilty or that they are a failure.
I: Inflammation
Inflammation commonly results in increased insulin resistance and worsening pancreatic beta cell deficiency, in the setting of increasing BGLs with toxicity. A common cause of inflammation is infection, particularly bacterial infection with increased levels of systemic proinflammatory cytokines. Infections may be overt (e.g. urinary tract infection, paronychia, bacterial pneumonia) or subtle (e.g. chronic periodontitis, osteomyelitis, chronic sinusitis); thus, it is important to have a healthy degree of suspicion of infection and consider occult causes.
Other causes of inflammation that may need investigation are listed in the Table and include autoimmune inflammatory diseases such as rheumatoid arthritis, types of seronegative arthritis and polymyalgia rheumatica. In our experience, these inflammatory conditions can result in marked deterioration in BGLs. Whatever the cause, once the systemic inflammatory condition is treated, BGLs usually become much easier to manage.
D: Drugs
Certain drugs can exacerbate hyperglycaemia. It is very common for people with type 2 diabetes to receive systemic glucocorticoids, often as anti-inflammatory treatments for asthma or as part of a chemotherapeutic regimen, for example. As a result, their BGLs deteriorate rapidly. The glucocorticoid is often taken in the morning, and the patient’s BGLs progressively rise during the day. In more severe cases, fasting hyperglycaemia is also markedly exacerbated. Managing hyperglycaemia worsened by a glucocorticoid often requires major intensification of blood glucose-lowering therapies such as tailored insulin regimens. It is very important to match the insulin regimen to the glucose profile and not just rely on a traditional type 2 diabetes insulin regimen. Typically, a person on prednisone will require much more insulin during the day and less insulin overnight and early in the morning when the corticosteroid effect wears off. The regimen for someone on dexamethasone, because of its longer action, would be different.
Medicines other than glucocorticoids can also exacerbate hyperglycaemia. The atypical antipsychotic agents, especially the ‘pines’, are prone to not only cause body weight gain but also exacerbation of hyperglycaemia. More rarely, they can cause severe pancreatic beta cell deficiency, even leading to diabetic ketoacidosis. When mirtazapine became more commonly used to treat clinical depression, we found that some patients with type 2 diabetes who were prescribed the agent had a major exacerbation of hyperglycaemia and their HbA1c levels increased by a number of percentage points, often resulting in marked deterioration in previously well-controlled BGLs.
Furthermore, although statin therapy usually results in minimal elevation in BGLs, we have observed some cases of marked increases in BGLs. Some published work in Australia suggests that the more potent statins are associated with an increase in HbA1c level of 0.5%.15 We emphasise that statins are very important in reducing cardiovascular risk in patients with diabetes, however it needs to be appreciated that in some people these medicines can cause deterioration in glycaemia, requiring intensification of blood glucose-lowering therapy.
Other prescribed medicines, including higher-dose thiazide diuretics, have also been shown to exacerbate hyperglycaemia; for example, hydrochlorothiazide at 25 mg/day or more. Thus, in a patient whose BGL is deteriorating, one consideration is changing therapies that may have a secondary adverse effect on blood glucose.
S: Something else
In cases where blood glucose is very difficult to control despite escalating doses of blood glucose-lowering therapy, consideration of the possible causes needs to include certain cancers that can cause marked insulin resistance and pancreatic beta cell deficiency. It is recognised that pancreatic adenocarcinoma and hepatocellular carcinoma can present as deteriorating glycaemia, including in people with pre-existing type 2 diabetes. Thus, in patients with persisting hyperglycaemia that is not responding to therapy, and in patients with progressive weight loss possibly with cachexia symptoms, imaging of the pancreas and, in correct clinical context, the liver should be considered. Other factors that can cause hyperglycaemia include progressive chronic kidney disease and liver impairment with chronic liver disease. Both of these conditions contribute to increasing insulin resistance.
It is also important to consider that sometimes diabetes mellitus subtype characterisation is incorrect. Many people diagnosed with type 2 diabetes may actually have a form of slow-onset type 1 diabetes known as latent onset autoimmune diabetes of adulthood, or LADA. In that setting, measuring pancreatic autoantibodies can help in making the correct diabetes mellitus diagnosis, especially antiglutamic acid decarboxylase (anti-GAD) autoantibodies plus autoimmune antibodies such as insulinoma antigen-2 (IA-2) and zinc transporter 8 (ZnT8). Be alert to this with regard to the person who is not overweight, in whom oral therapy has failed and who in a relatively short period (over a couple of years) requires insulin therapy to achieve their HbA1c target. Other causes of diabetes mellitus such as haemochromatosis or endogenous Cushing’s syndrome may explain deteriorating hyperglycaemia despite concerted treatment efforts.
The main reason blood glucose control deteriorates progressively in people with type 2 diabetes is that their pancreatic beta cells do not make enough insulin. Type 2 diabetes is a progressive disease and the rate of loss of pancreatic beta cell function in people from diagnosis is about 3 to 5% per year. Considering that the loss of this function is usually at 50% at diagnosis, by 10 years’ diabetes duration, most people will have lost more than 90% of their pancreatic beta cell function. This results in the need for insulin commencement, usually well within 10 years of the diagnosis of type 2 diabetes, due to ‘secondary failure’ of the pancreatic beta cells to make adequate insulin. Diabetes is a condition of insulin deficiency, and despite many more options in the treatment algorithm these days, including oral agents and noninsulin injectable therapies, most people with type 2 diabetes will in time require insulin treatment. In that clinical setting, advising the person that they will require increasing numbers of medications and increasing doses is important so that they know what to expect and that these increases are normal in the course of diabetes.
Conclusion
The AIDS acronym is intended to be an adjunct to the blood glucose algorithm as a tool to help target the cause or causes of deteriorating BGLs and to improve patient outcomes. The broad focus of this article precludes a detailed approach to investigating and managing each of the factors covered.
This article also does not address the important issue of management choices for symptomatic hyperglycaemia. At the extreme of hyperosmolar coma, patients will require hospital admission. For less marked symptomatic hyperglycaemia, options are greater and controlling hyperglycaemia is less urgent.
We have refined the AIDS acronym in recent months and found it to be of practical use in our team-based diabetes clinical service for systematising clinical care of patients with progressive chronic hyperglycaemia. When considering hypoglycaemia, a different acronym could be used, although the major cause of recurrent and severe hypoglycaemia still relates to adherence and a mismatch between medication dosage, physical activity and carbohydrate intake. We hope that other healthcare professional teams seeing patients with type 2 diabetes may find it useful to customise our tool to their local patient-care needs. ET
References
blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet 1998; 352: 854-865.
type 2 diabetes: the Fremantle Diabetes Study. Diabetes Obes Metab 2016; 18: 1143-1146.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.