Adjunctive metformin in type 1 diabetes

Diabetes type 1
Diabetes medicines
Many people with type 1 diabetes have suboptimal glucose control and features of type 2 diabetes (so-called ‘double diabetes’). This has led to interest in adjunctive therapy with noninsulin glucose control agents such as metformin. Clinical trials show some benefits of metformin in people with type 1 diabetes. Its (off-label) use merits discussion with the person with diabetes and their multidisciplinary team.
- People with type 1 diabetes may also have insulin resistance and clinical features of type 2 diabetes, contributing to suboptimal glucose control, micro- and macrovascular complications and premature death.
- There is interest in use of adjunctive medications for glucose control in people with type 1 diabetes treated with insulin; however, no medications are currently approved for this use in Australia.
- Among potential adjunctive medications, metformin has the largest evidence base and has small benefits for HbA1c, weight, LDL cholesterol, vascular function, carotid intima media thickness and kidney function in people with type 1 diabetes.
- Potential risks of adjunctive metformin include gastrointestinal upset, decreased vitamin B12 levels and possibly an increased risk of lactic acidosis.
- The optimal criteria for adjunctive metformin use in people with type 1 diabetes and monitoring are currently uncertain.
- Off-label use of adjunctive metformin in people with type 1 diabetes should be agreed with, and monitored by, the person with diabetes and their endocrinologist, GP and diabetes educator.
Despite advances in insulin treatment, including insulins with both longer and shorter durations of action, delivery systems such as insulin pumps and real-time continuous glucose monitoring, many people with type 1 diabetes have suboptimal glucose control. This places them at higher risk of acute and long-term complications.1,2
With exogenous insulin, excess caloric intake and sedentary lifestyles, many people with type 1 diabetes are overweight or obese, leading to so-called ‘double diabetes’. In double diabetes, people with type 1 diabetes have insulin resistance and clinical features common in people with type 2 diabetes. It is associated with increased insulin requirements, high rates of adiposity, a higher risk of hypoglycaemia, higher rates of micro- and macrovascular complications, nonalcoholic fatty liver disease and premature death.3-6 Adolescent growth spurts and polycystic ovary syndrome are also associated with increased insulin resistance in people with type 1 diabetes.
There is interest in the use of noninsulin glucose control agents, initially developed for people with type 2 diabetes, to improve glycaemia (including hyperglycaemia, hypoglycaemia and glucose variability) and to reduce hyperinsulinaemia, adiposity and long-term complications in people with type 1 diabetes.7-14 These drugs can be used as adjunctive therapy to exogenous insulin delivered by pump or injections.
This article discusses potential adjunctive glucose control therapies in people with type 1 diabetes, focusing on the most commonly studied and most widely used of these, metformin. The evidence base and clinical use of metformin in type 1 diabetes are described.
Potential adjunctive therapies to insulin
Potential classes of drugs that might be used as adjunctive therapy to insulin in people with type 1 diabetes include:
- insulin sensitisers (metformin and pioglitazone)
- incretin-based therapies glucagon-like peptide-1 (GLP-1) agonists and dipeptidyl peptidase-4 (DPP-4) inhibitors
- amylin analogues (e.g. pramlintide, which is not available in Australia)
- alpha-glucosidase inhibitors
- sodium-glucose cotransporter-2 (SGLT-2) inhibitors.8
Use of these therapies as adjuncts to insulin therapy in people with type 1 diabetes is currently off-label in Australia and most other countries. Clinical trials have been initiated for some agents and are planned for others. Only pramlintide is approved by the US Food and Drug Administration for use in people with type 1 diabetes. The main features of these potential adjunctive therapies are summarised in the Table.
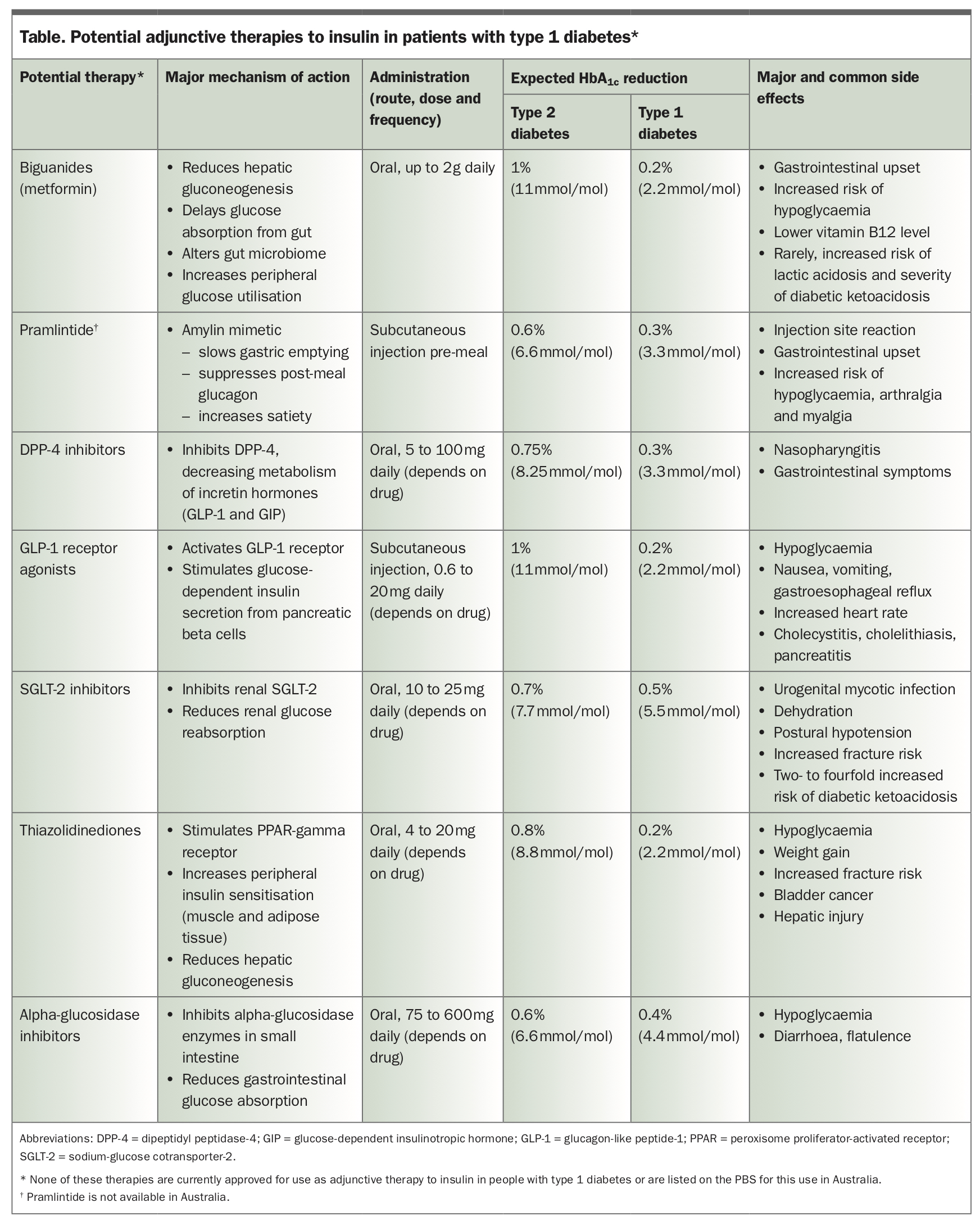{kind=link}
Of these therapies, metformin is the most often studied and is likely the most commonly used adjunctive therapy in clinical practice in Australia.9-14 In the Australian National Diabetes Information Audit and Benchmarking (ANDIAB) data collection, the prevalence of the metabolic syndrome (WHO criteria) in 2120 adults with type 1 diabetes was 30%. Metformin was prescribed to 7.7% of people with type 1 diabetes, more so in those with versus without the metabolic syndrome (16% versus 4%; p = 0.001).6 Adjunctive metformin is mentioned in some diabetes care guidelines, such as those of the American Diabetes Association.7 Metformin is not approved for use in people with type 1 diabetes in Australia.
Metformin as adjunctive therapy
Mechanism of action
Metformin, which has been used to treat people with type 2 diabetes for over 60 years, has a generally favourable efficacy, tolerability, safety and cost profile.15 It lowers the blood glucose level by multiple means, specifically decreasing glucose absorption from the intestine, decreasing hepatic gluconeogenesis and glucose output and increasing skeletal muscle glucose uptake, and also increases insulin sensitivity.
Some of metformin’s known mechanisms of action include increasing endogenous GLP-1 secretion, inhibiting advanced glycation end-product formation, inhibiting complex 1 of the mitochondrial respiratory chain, and activating AMP-kinase.15 AMP-kinase is a widely expressed intracellular enzyme involved in cellular energy homeostasis, fatty acid oxidation, glucose uptake, ketogenesis, lipolysis, lipogenesis and modulation of insulin secretion and action.
Benefits and risks
The potential clinical benefits and risks of adjunctive metformin are summarised in the Box, and some are further discussed below.
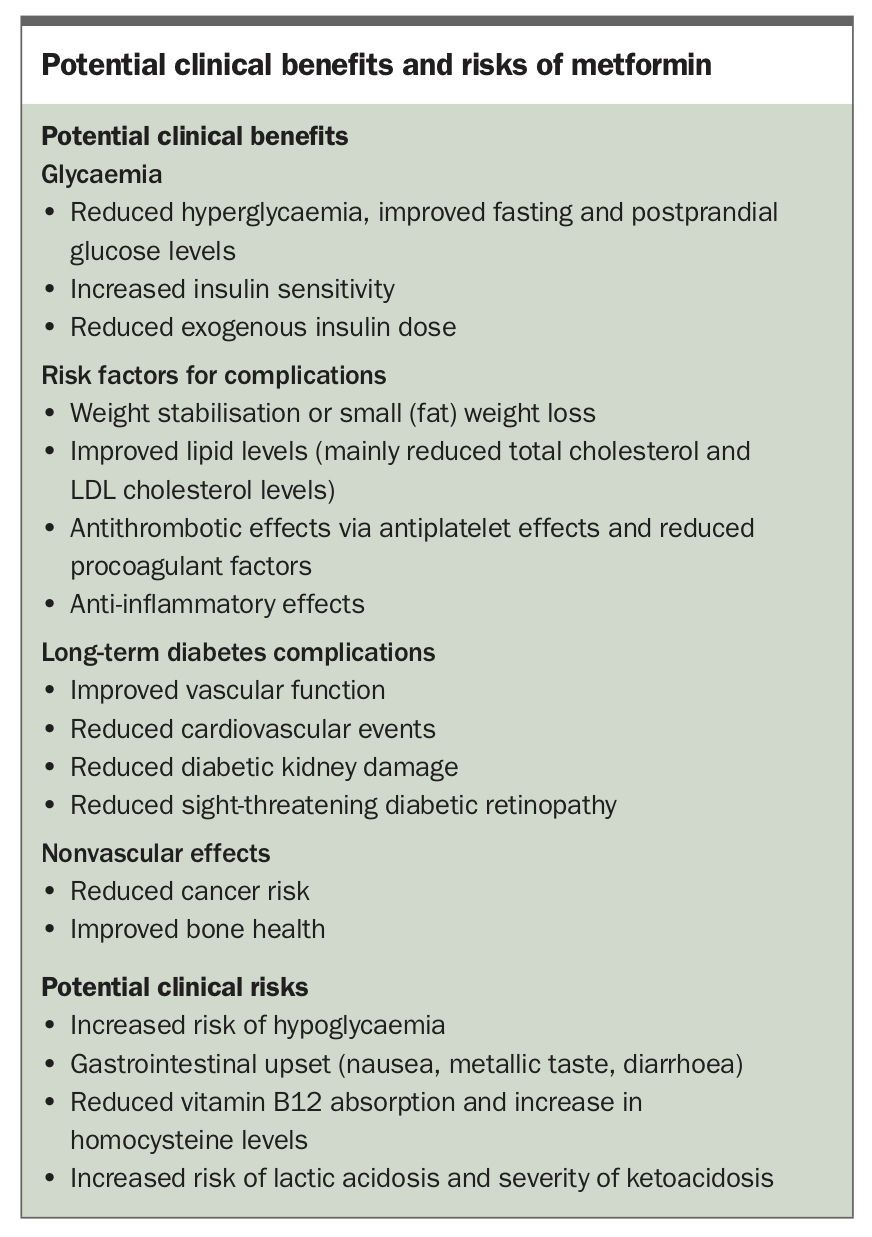{kind=link}
Studies of metformin in type 1 diabetes
Most of the over 200 clinical studies of metformin use in children and adults with type 1 diabetes relate to its effects on glycaemic control and vascular risk factors, with very few trials evaluating vascular function or long-term complications.8-21 Barriers to assessing long-term complications include the large numbers of participants and long follow up required and consequent high costs.9 In general, the use of metformin had often variable and at best small to modest favourable effects on glycaemia, total and LDL cholesterol levels, weight and fat mass, and total daily insulin dose. However, over the many years that atherosclerosis and microvascular complications of diabetes take to develop, even small improvements in risk factors may be beneficial.
In two placebo-controlled studies using hyperinsulinaemic-euglycaemic clamps, one in adults and the other in adolescents, metformin significantly increased glucose disposal.17,18 Glycaemic variability is an emerging risk factor for vascular complications. In a six-month pilot study using interstitial fluid continuous glucose monitoring, metformin did not significantly improve glucose variability.19
The few studies on the effects of metformin on the vasculature in people with type 1 diabetes have had mixed results. Two (one in adults for six months and another in children for 12 months) reported favourable effects of metformin on vascular function in people with type 1 diabetes.19,20 In contrast, in the three-year REMOVAL (REversing with MetfOrmin Vascular Adverse Lesions) trial the use of metformin in adults with type 1 diabetes showed no benefit on vascular function.21 The effect of metformin may differ according to the type of vascular function test used.19
The REMOVAL trial is the largest and longest study of metformin in people with type 1 diabetes to date, and the first with a cardiovascular disease (CVD) endpoint, albeit the surrogate measure, carotid intima media thickness (IMT).21 This multicentre study conducted in five countries, including Australia, involved 428 adults aged 40 years or older with a high CVD risk. It evaluated the effects of a mean of three years of metformin versus placebo treatment on the primary endpoint of carotid IMT; secondary and tertiary endpoints included renal and retinal measures, vascular function, weight, glycaemia, and lipids, vitamin B12 and homocysteine levels.
Metformin was associated with small but statistically significant improvements in HbA1c (−0.13 percentage points [−1.4 mmol/mol], with no increase in severe or milder hypoglycaemia), total daily insulin dose (−1.9 units/day), LDL cholesterol level (−0.13 mmol/L), weight (−1.2 kg) and estimated glomerular filtration rate (eGFR; −4 mL/min/1.73 m2).21 Although mean carotid IMT (the trial’s primary endpoint) was less with metformin versus placebo, the difference did not reach statistical significance. The prespecified secondary and tertiary endpoints of maximum carotid IMT (which includes plaque), kidney function and vascular risk factors were positive.21 Mean carotid IMT in nonsmokers and intervention for sight-threatening diabetic retinopathy were also positive. 22, unpublished data
Metformin adverse effects and contraindications
Potential adverse effects of metformin include gastrointestinal upset, rash and sometimes increased risk of hypoglycaemia, including severe hypoglycaemia (when used with insulin), and possibly the rare, but dangerous, lactic acidosis. Slow-release preparations of metformin have fewer gastrointestinal side effects. Metformin can reduce vitamin B12 absorption and, when vitamin B12 absorption is disrupted or there is concomitant folate deficiency, can increase homocysteine levels.16,23,24 There are no studies of the effects of vitamin B12 and/or folic acid supplementation on this homocysteine level rise in people with type 1 diabetes. Monitoring of vitamin B12 levels in people with type 1 diabetes taking metformin, and replacement therapy if these levels are low, are important, particularly if they have coeliac disease, pernicious anaemia or gut bacterial overgrowth caused by autonomic neuropathy (which can also lower vitamin B12 levels).
Lactic acidosis is a rare adverse effect of metformin. The risk of lactic acidosis is higher in people with kidney or liver disease, peripheral vascular disease, heart failure, recent myocardial infarction, pulmonary embolism, dehydration, blood loss, excessive alcohol intake or intercurrent illness and during and after a dye-requiring imaging study (which can worsen kidney function).16
A reduction in metformin dosage is recommended in people with chronic kidney disease, and metformin is best avoided in those with severe kidney disease (eGFR less than 30 mL/min/1.73 m2).25 Metformin is also contraindicated in people with liver failure and heart failure because of the increased risk of lactic acidosis. We suggest that metformin also be avoided in people with type 1 diabetes and recurrent diabetic ketoacidosis, because of the potentially high risk of adverse outcomes associated with combined diabetic ketoacidosis and lactic acidosis.
Although metformin is commonly prescribed for pregnant women with type 2 diabetes or gestational diabetes, we do not currently recommend its use during pregnancy and breastfeeding for women with type 1 diabetes. However, studies investigating this use are being undertaken.26
Which people with type 1 diabetes might benefit from metformin?
Clinical questions include:
- how to select people with type 1 diabetes who may benefit from adjunctive metformin
- how to monitor people with type 1 diabetes receiving adjunctive metformin.
The selection criteria may vary with the desired endpoint (e.g. reduced insulin dose or lower risk of complications). Currently, clinicians tend to offer metformin to those who are overweight or obese, have double diabetes or the metabolic syndrome, or are receiving high insulin doses.6 However, the REMOVAL trial suggested a benefit independent of body mass index (BMI), although the trial’s primary endpoint was not statistically significant.21 Adiposity and insulin resistance are not always well correlated. Even lean people may have insulin resistance.
Indices other than BMI may provide a better indication of the degree of insulin resistance. We suggest the use of a simple formula including clinical variables such as sex, age, waist to hip ratio, pulse pressure and HDL cholesterol level to estimate insulin sensitivity, such as those derived from the research tool of hyperinsulinaemic clamp studies.27
An alternative that merits further study is the use of the sex hormone binding globulin (SHBG) level as an indicator. The SHBG level has been shown to be inversely related to the magnitude of insulin resistance. A low SHBG level has been associated with increased insulin resistance and type 2 diabetes.28 In our cross-sectional study in adults with type 1 diabetes, we found that SHBG levels declined as the number of features of metabolic syndrome increased (unpublished data).
Using metformin in clinical practice
Although clinical trials show that metformin has small benefits on weight, glycaemia, LDL cholesterol level, vascular function and some long-term diabetes complications, it should not be routinely prescribed to all people with type 1 diabetes. Some doctors offer it as off-label use/non-PBS prescriptions to some of their patients with type 1 diabetes, usually those with double diabetes or metabolic syndrome who have no contraindications. The off-label use of adjunctive metformin in people with type 1 diabetes should be agreed with and monitored by the person with diabetes and their endocrinologist, GP and diabetes educator.
Metformin should usually be started at a low dose (e.g. 500 mg once daily with food) and titrated upwards slowly in people with type 1 diabetes, as in those with type 2 diabetes, to a maximum of 2 g daily (or less if kidney impairment is present) as tolerated, with insulin dosage adjustment as needed to avoid hypoglycaemia. Initial adverse gastrointestinal side effects often settle with time without drug cessation. As in people with type 2 diabetes, once-daily extended-release metformin may reduce some side effects and improve adherence relative to that with standard (nonextended release) metformin formulations.16,21 Checking of vitamin B12 levels and stopping metformin use during intercurrent illnesses, surgery or vascular dye studies is desirable. GPs are well placed to help ensure the safe use of adjunctive metformin.
Notwithstanding interest in adjunctive pharmacotherapy to reduce insulin resistance and metabolic features of type 2 diabetes in people with type 1 diabetes, attention should be given to maintaining a healthy weight and optimal nutrition, abstinence from smoking, regular aerobic and resistance physical activity, limited alcohol intake and good sleep hygiene. Stress and depression have adverse cardiometabolic effects and should be screened for and managed appropriately. It is not sufficient to measure weight; waist circumference should also be measured. Glycaemic control, levels of lipids (including triglycerides and HDL cholesterol) and blood pressure should be regularly monitored. Increasing abnormalities should prompt clinical review of lifestyle factors and perhaps in the future consideration of adjunctive pharmacotherapy.
Conclusion
Many people with type 1 diabetes have suboptimal glycaemic control, are overweight or obese, and have or are at high risk of long-term complications. Coexistent insulin resistance may contribute to these problems. There is ongoing interest in the use of adjunctive glucose control therapies in people with type 1 diabetes, with the goals of improving glycaemia and other risk factors, and reducing excess body fat and the risk of long-term complications. Of the five drug classes of interest, none are currently approved for use in Australia. Metformin is the most commonly studied and likely used off-label adjunctive therapy. The use of metformin in people with type 1 diabetes should be agreed with, and monitored by, the person with diabetes and their endocrinologist, GP and diabetes educator. We recommend monitoring their vitamin B12 levels and supplementing if required. Ongoing research is desirable to inform about the clinical benefits and risks and how best to choose and monitor people with type 1 diabetes for adjunctive metformin. ET