Ashim is a 70-year-old retired engineer with a history of type 2 diabetes, diagnosed at 55 years of age on a routine medical test. He was initially given recommendations for lifestyle modification. One year later, he was started on metformin, which he has taken ever since. Four years later, a sulfonylurea was added. Five years ago, due to progressive deterioration in his HbA1c and increase in his fasting blood glucose levels (BGLs), Ashim was started on insulin glargine, once daily. Ashim developed microvascular complications of diabetes, including mild nonproliferative diabetic retinopathy and microalbuminuria, but he has remained stable on ACE inhibitor therapy, with no impairment of renal function (estimated glomerular filtration rate [eGFR] >90 mL/min/1.73 m2).
Six months ago, Ashim presented to you, his GP, with chest pain and shortness of breath. An ambulance was called to take him to hospital, where he was found to have a 70% stenosis of his left anterior descending coronary artery. He underwent angioplasty and stenting. His HbA1c was 7.5% on presentation. In hospital, he was started on a sodium-glucose cotransporter-2 (SGLT-2) inhibitor, empagliflozin 10mg, in addition to his usual metformin, sulfonylurea and basal insulin.
Advertisement
How do SGLT-2 inhibitors work?
Under normal circumstances, about 180 g of glucose is filtered through the kidneys each day. The SGLT-1 and SGLT-2 are cell-surface proteins in the proximal tubular cells of the nephron, responsible for the reabsorption of filtered glucose back into the bloodstream. SGLT-1 and SGLT-2 are responsible for 10% and 90% of glucose reabsorption, respectively, thus preventing glucose from appearing in the urine. Glycosuria occurs when the capacity to reabsorb filtered glucose is exceeded, usually due to hyperglycaemia. SGLT-2 inhibitors block tubular reabsorption and permit excretion of 50 to 100 g of glucose daily.1 This has beneficial effects on blood glucose lowering and caloric loss, in clinical trials, equating to an average reduction in HbA1c of 0.5 to 1% and weight reduction of about 2 kg compared with placebo.2 Glycosuria induces water excretion, due to the osmotic effects of glucose.
Common side effects of SGLT-2 inhibitor therapy include polyuria and dehydration, if adequate fluid intake is not maintained. This can lead to hypotension, especially if co-prescribed with antihypertensive agents. Glycosuria creates a conducive environment for bacterial and fungal growth, which leads to an increased risk of genitourinary tract infections. It is important to remember that measurement of urinary glucose does not reflect a patient’s blood glucose profile when taking an SGLT-2 inhibitor.
What are the indications for starting an SGLT-2 inhibitor?
According to the 2018 American Diabetes Association and European Association for the Study of Diabetes consensus report on the Management of hyperglycemia in type 2 diabetes, SGLT-2 inhibitors are appropriate second-line agents in people with established atherosclerotic cardiovascular disease who have not met glycaemic targets with use of metformin alone.3 They may also be considered after metformin in people in whom weight management and/or minimisation of hypoglycaemia are clinical priorities. They can be added as third-line agents when glycaemic targets are not achieved with dual therapy.
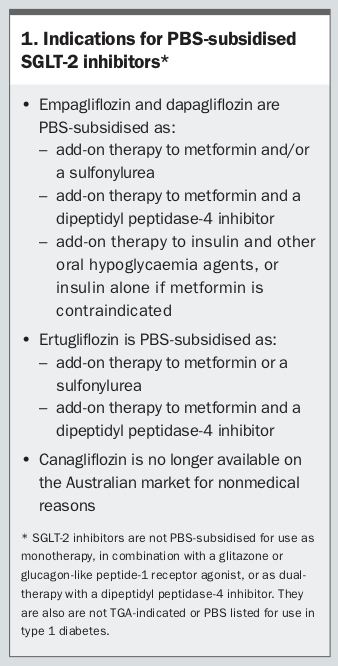
SGLT-2 inhibitors are indicated by the TGA as monotherapy in patients for whom metformin is considered inappropriate, and as add-on therapy to any other glucose-lowering therapy when glycaemic targets are not being met. Indications for PBS-subsidised SGLT-2 inhibitors are listed in Box 1. SGLT-2 inhibitors are not recommended for glucose lowering in people with significant renal disease (eGFR <45 to 60 mL/min/1.73 m2, depending on the agent), as their mechanism of action depends on adequate glomerular filtration. However, recent trials suggest that SGLT-2 inhibitors may have renoprotective effects in people with lower eGFRs (down to an eGFR of 30 mL/min/1.73 m2).2
What are the benefits of adding SGLT-2 inhibitors to insulin therapy?
Although insulin is often considered ‘the last line’ in diabetes management, adding an SGLT-2 inhibitor has been shown to reduce insulin requirements, improve glycaemic control while maintaining lower daily insulin requirements, improve weight parameters, lower blood pressure and potentially reduce hypoglycaemic risk.4
Advertisement
What are the cardiovascular benefits of SGLT-2 inhibitors?
In the Canagliflozin Cardiovascular Assessment Study (CANVAS) of 10,142 participants with type 2 diabetes, of whom 66% had a history of cardiovascular disease, canagliflozin reduced the composite outcome of cardiovascular death, nonfatal myocardial infarction and nonfatal stroke by 13% compared with placebo.5 In the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) study of 7020 participants with established cardiovascular disease, empagliflozin reduced the risk of the same composite outcome by 14%.6 A reduction in heart failure admission and all-cause mortality was also observed. In the Dapagliflozin Effect on Cardiovascular Events-Thrombolysis in Myocardial Infarction 58 (DECLARE-TIMI58) trial of 17,160 patients, of whom 42% had atherosclerotic cardiovascular disease, dapagliflozin did not significantly reduce the composite outcome of major adverse cardiovascular events compared with placebo, but did result in a lower rate of hospitalisation for heart failure.7 Taken together, these studies suggest that SGLT-2 inhibitors should be considered, where indicated, in people with heart failure, and in the Australian context, empagliflozin can be used for secondary prevention of atherosclerotic cardiovascular disease, including in patients treated with insulin. These studies also demonstrated reduced risk of progression of renal disease.
Ashim returned to see you four months after his hospital admission. He described his cardiac event as being a ‘wake-up call’ and had made concerted efforts to manage his diabetes. In particular, he had eliminated white rice and naan bread from his diet and switched to grilled meat and fish, and vegetables. Although he was not overweight to start with, he had lost 4kg since admission and now had a body mass index of 21 kg/m2. On follow up in the hospital’s postdischarge diabetes clinic, the insulin glargine dose had been gradually reduced due to early morning hypoglycaemia, with a plan to cease it altogether if his BGLs remained in target. As Ashim’s HbA1c had come down to 6.5% and he was only taking eight units of glargine daily, you were able to cease the insulin at that visit.
Ashim walks into your clinic today looking pale and unwell. It is six months since his hospital admission, and your immediate thought is whether he may be having another coronary event. He denies chest pain, but states that he first became unwell with a ‘gastro bug’, seven days ago. He had initial vomiting and diarrhoea, which seemed to settle after a couple of days, although he remained off his food. In the past 48 hours he has felt more unwell, with recurrence of vomiting, accompanied by abdominal pain and shortness of breath. On examination, he has dry mucous membranes and reduced skin turgor. His blood pressure is 100/60 mmHg, with a pulse rate of 105 beats per minute. He is afebrile. His abdomen is soft, with nonspecific generalised tenderness but no rebound. Cardiac and respiratory examination is unremarkable. His BGL is 11 mmol/L. His ECG reveals sinus tachycardia but is otherwise unchanged. A urine dipstick is positive for glucose and large ketones. This prompts you to check his blood ketone levels using a ketone meter and a finger prick blood sample.
Advertisement
What are ketones and how do you interpret blood or urine ketone levels?
The term ‘ketone bodies’ refers to three molecules: acetoacetate, 3-beta-hydroxybutyrate and acetone, which are produced by the liver during fatty acid breakdown, particularly in the setting of low carbohydrate availability.8 As the brain cannot use fatty acids for energy, 3-beta-hydroxybutyrate and acetoacetate provide an alternative source of energy to glucose during prolonged fasting or starvation. Acetone gives the breath a sweet odour, which can be a recognisable sign of ketoacidosis. Very low levels of ketones may normally be present in the blood during fasting or intense exercise, but high levels result in ketoacidosis, which can cause major organ dysfunction.
Some glucose meters have a dual function, enabling detection of blood glucose and blood ketone levels, using two different types of testing strips inserted into the same device. This is a simple bedside test that measures beta-hydroxybutyrate, the predominant blood ketone. Readings of less than 0.6 mmol/L are considered to be in the normal range. Readings between 0.6 and 1.5 mmol/L suggest that increased ketogenesis is occurring. Readings greater than 1.5 mmol/L indicate high risk of ketoacidosis and levels greater than 3.0 mmol/L require urgent attention.
Urine dipstick tests provide a semi-quantitative measure of acetoacetate, which is a less reliable indicator of total ketone levels. Blood ketones may rise acutely before they can be detected in the urine, usually with a delay of two to four hours. Urinary dipstick is not recommended for detecting or monitoring ketones, although it may give clues to a diagnosis of ketoacidosis when performed for other reasons.
Ashim’s ketone level is elevated at 6.6 mmol/L and you refer him to hospital for further evaluation. A blood gas is performed in the emergency department, revealing a pH of 7.18. He is given intravenous rehydration and placed on an insulin-dextrose infusion, with hourly blood ketone monitoring. His oral hypoglycaemic agents are withheld. He is given a diagnosis of SGLT-2 inhibitor-related euglycaemic ketoacidosis.
What is euglycaemic ketoacidosis and how does it differ from diabetic ketoacidosis?
Low carbohydrate availability and subsequent fatty acid breakdown is the pathogenic feature of both these conditions. Diabetic ketoacidosis (DKA) more commonly occurs in people with type 1 diabetes due to insulin deficiency. Without insulin, glucose in the blood cannot be transported into cells to be used for energy and alternative energy sources are required. DKA is defined by the classic triad of hyperglycaemia, ketosis and high anion gap metabolic acidosis (pH <7.3, or HCO3 <15 to 18 mmol/L). DKA can also occur in people with type 2 diabetes during significant physical stress, such as sepsis, trauma and cardiovascular compromise.
Euglycaemic ketoacidosis was initially used to describe the small proportion of patients with true DKA, but with BGLs less than 16.5 mmol/L.9 These were often young women with type 1 diabetes who had very low carbohydrate consumption. Since the advent of SGLT-2 inhibitors, a new form of euglycaemic ketoacidosis has been recognised, where low carbohydrate availability is the result of ongoing pharmacologically-induced urinary glucose excretion.9
Advertisement
How common is SGLT-2 inhibitor-associated ketoacidosis and what are the risk factors?
In a randomised clinical trial of canagliflozin in people with type 2 diabetes, the DKA rate was very low, in the realm of 0.5 to 0.8 cases per 1000 patient years, compared with 0.2 cases per 1000 patient years in non-SGLT-2 inhibitor treatment arms.10 More than 50% of cases were subsequently found to have autoimmune diabetes, and most were using insulin. Insulin omission and/or intercurrent illness were also implicated. It is possible that the incidence of DKA in real-world users of SGLT-2 inhibitors is higher than in clinical trials, which involve carefully selected patients in supervised environments. A South Australian study estimated a rate of 1.8 per 1000 patient-years, based on adverse events reported to the TGA and the number of SGLT-2 prescriptions dispensed in the equivalent time period.11 A 2017 paper reviewed 105 cases of DKA in SGLT-2 users, of which 66 had presumed type 2 diabetes.12 Nine of these were subsequently diagnosed with autoimmune or pancreatic diabetes. Both hyperglycaemia and euglycaemia at presentation were observed. The duration of SGLT-2 inhibitor use varied from one day to more than one year. Precipitating factors such as insulin dose reduction or discontinuation, surgery, infection and dietary change were present in 78% of cases. The average duration of type 2 diabetes was 9.5 years.
What specific factors may have predisposed Ashim to ketoacidosis?
Ashim’s long duration of diabetes and previous requirement for insulin therapy could suggest poor beta-cell function and insulin deficiency. Weight loss and carbohydrate restriction assisted his successful transition off insulin while taking an SGLT-2 inhibitor. However, in the setting of intercurrent illness and dehydration, which increase insulin-opposing, counter-regulatory hormones, and with further reduction of carbohydrate intake compounding ongoing urinary glucose losses, fatty acid metabolism replaced glucose as an alternative fuel source. Dehydration is a particular concern in elderly users, who might have impaired thirst recognition, reduced access to fluids, or fluid restrictions imposed for other medical reasons, such as heart failure or renal disease. Abrupt reductions or interruptions in insulin therapy may also precipitate DKA.
Ashim’s condition improves with rehydration and his vital signs and renal function return to normal. His ketone levels gradually fall with insulin and carbohydrate administration and he resumes his normal diet. He is transitioned back to regular basal insulin, and metformin and a sulfonylurea are restarted. Ashim’s postprandial BGLs remain above target on the ward, and he wants to know if he should restart the SGLT-2 inhibitor. He is concerned about the risk of weight regain and the loss of cardiovascular benefit if the empagliflozin is permanently discontinued. He is not keen on having prandial insulin injections.
Can patients with SGLT-2 inhibitor-associated ketoacidosis restart SGLT-2 inhibitors once the episode has resolved and what precautions should be taken to reduce the risk of future diabetic ketoacidosis?
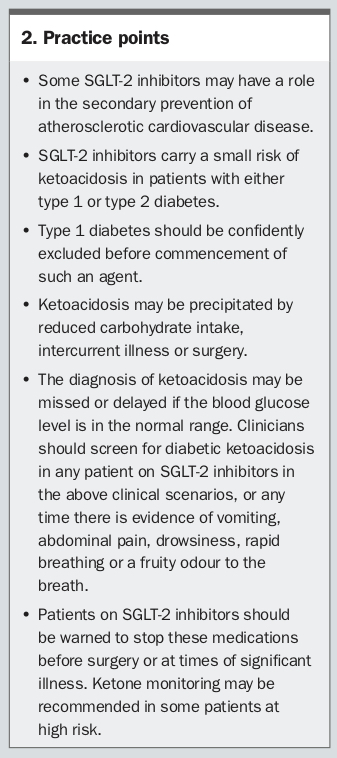
There is no clear consensus on whether restarting the SGLT-2 inhibitor is safe. In cases where DKA developed spontaneously without precipitant, it seems wise to avoid subsequent use of these agents. Death from SGLT-2 inhibitor-induced DKA has been reported. In other situations where clear precipitants are identified it may be reasonable to reuse the agents on the proviso that they are withheld in the future during any period of carbohydrate restriction or significant physiological stress, such as illness or surgery (
Box 2).
Advertisement
As an added precaution, some people on SGLT-2 inhibitors may choose to monitor their blood ketone levels on a regular basis. If ketone levels are greater than 0.6 mmol/L, they should withhold the medication and increase carbohydrate intake until levels resolve. Blood ketone strips are not currently subsidised under the National Diabetes Services Scheme.
What are the current recommendations regarding SGLT-2 inhibitor use before surgery?
A safety alert released by the Australian and New Zealand College of Anaesthetists recommends ceasing SGLT-2 inhibitors up to three days preoperatively (two days before surgery and the day of surgery), or in other situations of high physical stress. SGLT-2 inhibitors should only be restarted postoperatively when the patient is eating and drinking.13
It is prudent to recall that metformin should also be withheld in similar settings of dehydration, physiological stress and before surgery, due to the potential risk of lactic acidosis.
In what other situations should SGLT-2 inhibitors be used with caution?
Although generally safe and effective, there are particular patient groups in which SGLT-2 inhibitor therapy may not be appropriate. Older patients may be at greater risk of postural hypotension and falls following SGLT-2 inhibitor commencement due to volume shift and diuresis. Patients with recurrent genitourinary infections, urinary incontinence or urologic conditions (such as significant prostatic hypertrophy or recurrent kidney stones) may not be suitable for SGLT-2 inhibitor therapy.
Patients with diabetes experiencing unintentional weight loss, indicating a catabolic state and insulin deficiency, would be best treated with insulin therapy and investigations for weight loss undertaken, as appropriate. In some studies, SGLT-2 inhibitors have been associated with increased risk of lower limb amputations. Although reasons for this association are unclear, SGLT-2 inhibitors may not be an ideal choice in people with severe peripheral vascular disease.
SGLT-2 inhibitors are not indicated for use in type 1 diabetes in Australia – if there is any diagnostic uncertainty, anti-GAD and anti-IA2 antibody tests should be conducted before drug initiation, as latent autoimmune diabetes in adults may be clinically difficult to distinguish from type 2 diabetes.
Ashim is tested for type 1 diabetes antibodies, and the results are negative. Given that this episode had a clear precipitant, Ashim is cautiously restarted on his SGLT-2 inhibitor but is educated to withhold this medication at times of serious illness, decreased oral intake or surgery. ET
COMPETING INTERESTS: None.
Advertisement
References
1. Kalra S. Sodium glucose co-transporter-2 (SGLT2) inhibitors: a review of their basic and clinical pharmacology. Diabetes Ther 2014; 5: 355-366.
2. Minze MG, Will KJ, Terrell BT, et al. Benefits of SGLT2 inhibitors beyond glycemic control: a focus on metabolic, cardiovascular and renal outcomes. Curr Diabetes Rev 2018; 14: 509-517.
3. Davies M, D’Alessio D, Fradkin J, et al. Management of hyperglycemia in type 2 diabetes. A consensus report by the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2018; 41: 2669-2701.
4. Woo V, Berard L, Bajaj H, et al. Considerations for initiating a sodium-glucose co-transporter 2 inhibitor in adults with type 2 diabetes using insulin. Can J Diabetes 2018; 42: 88-93.
5. Neal B, Perkovic V, Mahaffey K, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377: 644-657.
6. Zinman B, Wanner C, Lachin J, et al. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117-2128.
7. Wiviott S, Raz I, Bonaca M, et al. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019; 380: 347-357.
8. Laffel L. Ketone bodies: a review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab Res Rev 1999; 15: 412-426.
9. Rosenstock J, Ferrannini E. Euglycemic diabetic ketoacidosis: a predictable, detectable, and preventable safety concern with SGLT2 inhibitors. Diabetes Care 2015; 38: 1638-1642.
10. Erondu N, Desai M, Ways K, Meininger G. Diabetic ketoacidosis and related events in the canagliflozin type 2 diabetes clinical program. Diabetes Care 2015; 38: 1680-1686.
11. Meyer E, Gabb G, Jesudason D. SGLT2 inhibitor-associated euglycemic diabetic ketoacidosis: a South Australian clinical case series and Australian spontaneous adverse event notifications. Diabetes Care 2018; 41: e47-e49.
12. Bonora B, Avogaro A, Fadini G. Sodium-glucose co-transporter-2 inhibitors and diabetic ketoacidosis: an updated review of the literature. Diabetes Obes Metab 2018; 20: 25-33.

{kind=link}
{kind=link}