Niche oral agents in type 2 diabetes

Diabetes type 2
Diabetes medicines
Alpha-glucosidase inhibitors (e.g. acarbose) and thiazolidinediones (e.g. pioglitazone) are older classes of oral type 2 diabetes medication that are less commonly used because of their undesirable side effects. However, they are still effective therapeutic agents and may be considered when formulating a personalised management plan for patients with type 2 diabetes.
- Alpha-glucosidase inhibitors (e.g. acarbose) and thiazolidinediones (e.g. pioglitazone) have not been definitively shown in prospective trials to have specific effects in reducing cardiovascular events or mortality in people with type 2 diabetes but may have niche roles in their treatment.
- Although many patients do not tolerate acarbose because of gastrointestinal side effects, its use may delay progression of impaired glucose tolerance to type 2 diabetes.
- Risk of hypoglycaemia on acarbose or thiazolidinedione monotherapy is low; however, if used in combination with insulin, sulfonylurea therapy (or fibrates in the case of thiazolidinediones), hypoglycaemia risk is increased.
- Thiazolidinediones are an effective oral agent in treatment of patients with type 2 diabetes but have been associated with significant adverse effects and must be used judiciously.
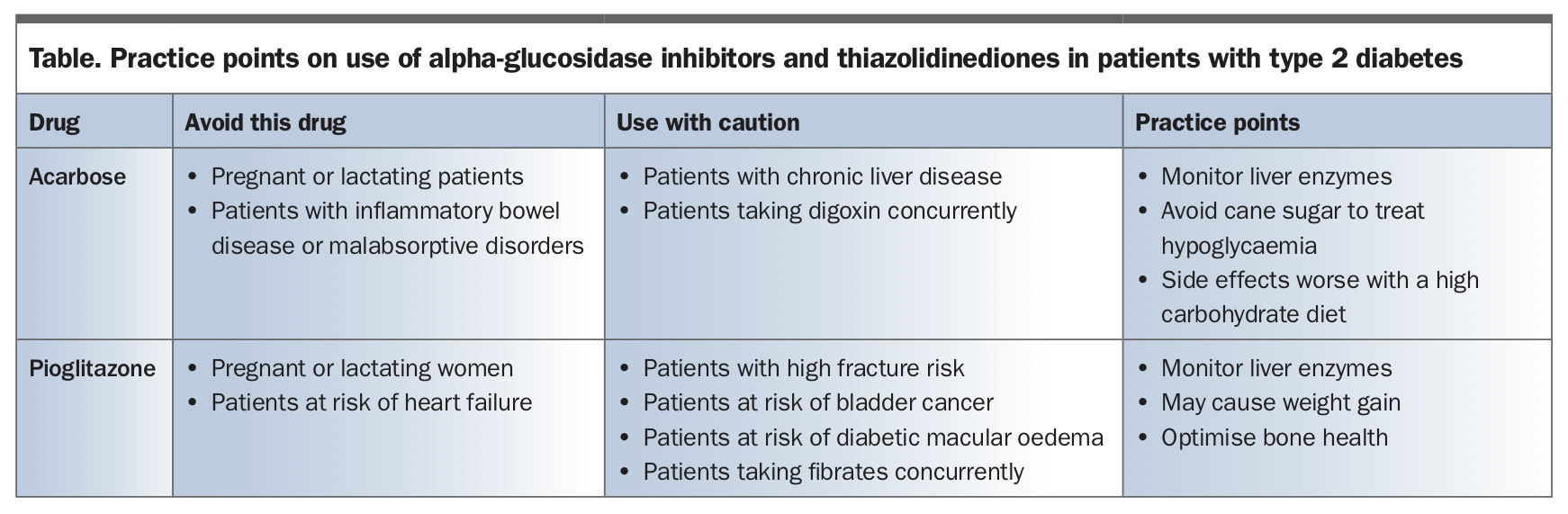
A multitude of oral and injectable therapies are available in Australia for managing patients with type 2 diabetes. Each has its own role and understanding the risks and benefits enables personalised treatment of an individual patient. Metformin remains the first-line option and, as a result of favourable cardiovascular mortality outcomes in trials, use of sodium-glucose cotransporter-2 (SGLT-2) inhibitors and glucagon-like peptide-1 (GLP-1) receptor agonists have become increasingly popular as second-line agents.1 Nevertheless, there is a role for two less commonly used, older classes of diabetes medications: alpha-glucosidase inhibitors and thiazolidinediones. Medications in these classes available in Australia include acarbose and pioglitazone. This article provides guidance on use of these two ‘niche’ oral therapies. Practice points on the use of these therapies are summarised in the Table.
{kind=link}
Alpha-glucosidase inhibitors: acarbose
Acarbose is an alpha-glucosidase inhibitor available in Australia that acts as a competitive, reversible inhibitor of pancreatic alpha-amylase and membrane-bound intestinal alpha-glucosidase hydrolase.2 Acarbose acts locally in the gastrointestinal (GI) tract to reduce carbohydrate absorption and less than 2% is absorbed into the systemic circulation.2 Although a 2004 meta-analysis suggested a cardiovascular benefit to patients with type 2 diabetes using acarbose, a more recent, appropriately conducted meta-analysis of randomised controlled trials did not support this conclusion.3,4
Advantages of acarbose
Acarbose reduces glycated haemoglobin (HbA1c) in a dose-dependent manner. At the initial dose of 25 mg three times daily, HbA1c level is reduced by 0.44% and at the maximum dose of 200 mg three times daily, HbA1c level is reduced by 0.86%.2 Hypoglycaemia does not occur with acarbose monotherapy, but if the patient uses other drugs that cause hypoglycaemia such as insulin or sulfonylureas, acarbose may increase the risk. Importantly, given its mechanism of action, oligosaccharides such as cane sugar (sucrose) are less effective in treating hypoglycaemia in patients taking acarbose, and they should be counselled regarding this.
For patients who have had a diagnosis of impaired glucose tolerance, the STOP-NIDDM trial showed that long-term treatment with acarbose delayed progression to type 2 diabetes by 25% over 3.3 years, a finding that was confirmed in a meta-analysis.4,5
In Australia, acarbose is subsidised by the PBS and can be prescribed in combination with other agents. For patients on insulin therapy, acarbose can reduce insulin requirements and assist in achieving optimal blood glucose levels.6,7
Disadvantages of acarbose
The most common adverse effects are GI symptoms such as flatulence, diarrhoea and abdominal discomfort. A diet high in carbohydrates may worsen the GI side effects but patients may develop tolerance to these with time. In the landmark STOP-NIDDM trial, 31% of patients in the acarbose treatment arm discontinued treatment early compared with 19% in the placebo arm, predominantly because of GI side effects.5 Acarbose treatment can also cause hepatotoxicity; therefore, consider checking serum transaminase concentrations every three months for the first year of therapy.2
Acarbose in specific patient populations
A meta-analysis found that acarbose was associated with significantly greater weight loss (0.92 kg, p <0.05) in Chinese ethnic populations than Caucasian ethnic populations, in whom there was no difference, compared with placebo.8 This may be because of dietary differences, with Chinese populations typically consuming more carbohydrates.
Acarbose should be used with caution in patients who have chronic liver disease, as it has been associated with hyperammonaemia.9 We suggest avoiding acarbose in patients with chronic intestinal problems such as inflammatory bowel disease or malabsorptive disorders. Studies have not established the safety of acarbose in pregnant women or nursing mothers and it should therefore be avoided in these groups. In patients with a heart condition, acarbose may decrease absorption of digoxin, and this combination should be used with caution. Monitoring of digoxin levels is suggested.10
Thiazolidinediones
Thiazolidinediones decrease insulin resistance directly through activation of peroxisome proliferator-activated receptor gamma (PPARγ).11 Meta-analyses show that pioglitazone and rosiglitazone affect cardiovascular outcomes differently, and this is likely the because of the different extent to which each activates PPARα and PPARγ.12
In 2007, safety concerns were raised about the use of rosiglitazone after a meta-analysis of 42 studies found its use was associated with an increased risk of myocardial infarction and death from cardiovascular causes.13 As a result, rosiglitazone is no longer available in Australia and the main thiazolidinedione used is pioglitazone.
Pioglitazone has not been shown to increase cardiovascular mortality. In the PROactive (Prospective Pioglitazone Clinical Trial in Macrovascular Events) trial, pioglitazone failed to reach the primary endpoint (a composite of all-cause mortality and cardiovascular outcomes); however, the secondary ‘3-point major adverse cardiovascular event’ endpoint, which is used in other cardiovascular outcome trials, was reduced (hazard ratio, 0.84; p = 0.027) and there was a trend toward reducing all-cause mortality and ‘any’ cardiovascular outcome including peripheral vascular disease.14 The IRIS trial studied participants who had a recent transient ischaemic attack or stroke.15 Although the participants did not have diabetes, they had insulin resistance and there was a reduced risk of stroke or myocardial infarction in the pioglitazone arm.15 This provides further support of cardiovascular protection with pioglitazone in patients who have insulin resistance.
Advantages of thiazolidinediones
Pioglitazone reduces HbA1c levels by 0.8% from a baseline of 7.8%.14 It could be argued that the mechanism of action of thiazolidinediones directly targets insulin resistance – a key component of the pathophysiology of type 2 diabetes. There is improvement of dyslipidaemia, with an increase in plasma HDL cholesterol level by 10 to 20% and a reduction in plasma free fatty acid level by 25 to 35%.11
For patients who are on very high doses of insulin, pioglitazone can potentially improve glycaemic control and reduce insulin requirements substantially, which could reduce a patient’s expense on medication if large amounts are spent on insulin therapy.
Pioglitazone has been shown to improve liver biochemical and histologic parameters in patients with nonalcoholic steatohepatitis.16 This is likely due to pioglitazone’s mechanism of action that reduces insulin resistance, a key mediator in the development of nonalcoholic fatty liver disease.
Results from the ADOPT study suggested that rosiglitazone had a more durable glycaemic response compared with a sulfonylurea (glibenclamide) or metformin, with 40% of patients in the rosiglitazone monotherapy group achieving an HbA1c level below 7% compared with 36% in the metformin group and 26% in the glibenclamide group.17 However, in clinical practice, it would be unusual for patients to be on thiazolidinedione monotherapy and this assumes pioglitazone would have a similar result as rosiglitazone. Further research is needed to determine whether combination therapy with thiazolidinediones provides better long-term control of diabetes.
Disadvantages of thiazolidinediones
Congestive cardiac failure is the most significant side effect of treatment with thiazolidinediones and the drug should be avoided in patients with chronic heart failure. Several studies showed an increased risk of hospitalisation for heart failure with thiazolidinediones compared with placebo.11 The cohort of patients considered for thiazolidinedione treatment often have multiple risk factors for congestive cardiac failure so consideration should be given to assessing baseline cardiac function with echocardiography.
Multiple studies have shown an increased risk of fractures in patients treated with thiazolidinediones.11 A longer duration of treatment with thiazolidinediones and higher doses are thought to be associated with a higher risk of fracture. A large study (IRIS trial) showed the absolute fracture risk increased from 5.2% to 9.4% in men and 11.6% to 14.9% in women on pioglitazone.18 Therefore, if a patient is taking or considered for thiazolidinedione treatment, and is at increased risk of fractures, bone health should be assessed with dual-energy x-ray absorptiometry, optimised with calcium and vitamin D supplementation if needed, and antiresorptive treatment considered.
Pioglitazone is associated with dose-related weight gain, particularly when combined with insulin therapy (3.5 to 6 kg of weight gain). It is thought that the weight gain is related to a combination of fluid retention and an increase in subcutaneous fat, with no change or even a small reduction in visceral fat.11
There is controversy over the association between pioglitazone and bladder cancer after 14 cases of bladder cancer were identified in patients in the pioglitazone arm compared with nine in the placebo arm of the PROactive study.14 Subsequent studies showed conflicting results. However, in 2018, a systematic review and meta-analysis of the literature showed a slight but statistically significant increase in the risk of bladder cancer with a suggestion of a time and dose relationship.19 Given the concern regarding this association, we would advise caution with using pioglitazone in patients with risk factors for bladder cancer, such as smoking history or occupational chemical exposure, and in patients with unexplained microscopic haematuria.
A retrospective cohort study showed that, at one year, 1.3% of patients treated with thiazolidinediones had diabetic macular oedema compared with 0.2% of control patients.20 Similarly, a prospective, cohort study found that 2.7% of patients using thiazolidinediones had diabetic macular oedema compared with 1.0% of control patients.21 Although the absolute increase in risk is modest, this is still an important consideration depending on the patient’s occupation and circumstances.
Although pioglitazone has been shown to be beneficial in patients with nonalcoholic steatohepatitis, the thiazolidinedione, troglitazone, was removed from the market because of concern over severe hepatocellular injury.22 Therefore, it is suggested to check a patient’s liver enzymes at baseline and then intermittently monitor liver enzymes during treatment with thiazolidinediones, with the frequency depending on the clinical scenario.
Hypoglycaemia is uncommon in patients on thiazolidinedione monotherapy but, if used in combination with insulin or sulfonylureas, the risk is increased. Because the peak glycaemic effect of thiazolidinediones may take at least a month, onset of hypoglycaemia can be delayed.23, 24
In Australia, under the PBS, GLP-1 agonists, dipeptidyl peptidase-4 (DPP-4) inhibitors and SGLT-2 inhibitors cannot be subsidised if used in combination with pioglitazone. Therefore, the addition of pioglitazone may incur additional financial costs for patients on these medications.
Thiazolidinediones in specific patient populations
As described earlier, pioglitazone can markedly reduce the insulin requirements for patients on very large insulin doses. Pioglitazone is also highly effective for patients who have the rare loss-of-function mutations in PPARγ.25 There is currently insufficient information to support the use of thiazolidinediones in pregnant and breastfeeding women. Fenofibrate or gemfibrozil may inhibit CYP2C8, the major metabolic pathway for thiazolidinediones. Therefore, patients taking these drugs may be at a higher risk of hypoglycaemia.23
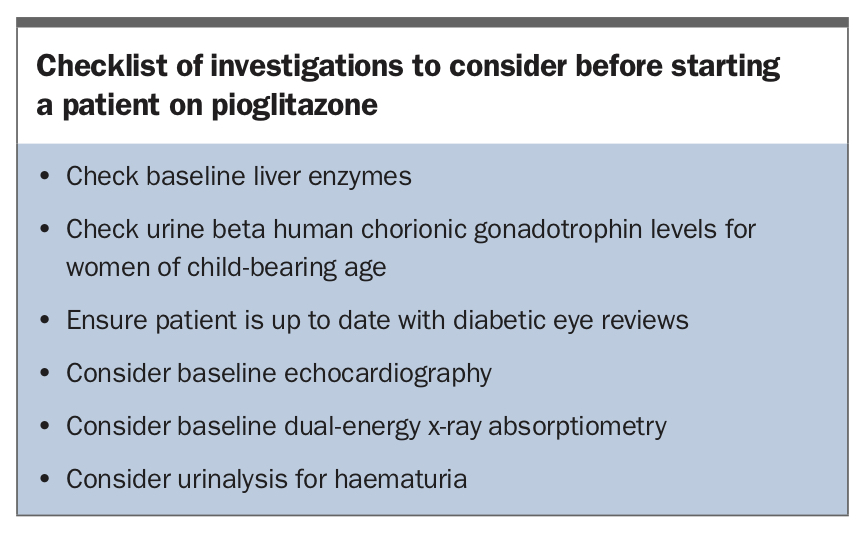
In summary, thiazolidinediones should be used judiciously with careful consideration of comorbidities. Investigations to consider before commencement of thiazolidinediones are shown in the Box. For patients on long-term treatment with thiazolidinediones, consider intermittent assessment with dual-energy x-ray absorptiometry and echocardiography.
{kind=link}
Conclusion
Alpha-glucosidase inhibitors and thiazolidinediones are effective oral treatments for type 2 diabetes and, with an understanding of their risks and benefits, can be used on a case-by case basis. Their use is particularly applicable in situations where patients are reluctant to commence injectable therapy but require an escalation of treatment to achieve adequate control. Given a large proportion of patients with diabetes have significant cardiovascular risk, glucose-lowering drugs that have been shown to reduce cardiovascular mortality should be considered as second-line treatment to metformin. The evidence potentially supports pioglitazone having cardiovascular benefits and acarbose can be a useful adjunct. ET
COMPETING INTERESTS: Associate Professor Stranks receives speaker payments from Sanofi, Lilly and Astra-Zeneca; is on the Advisory Board for Astra-Zeneca; and is the current President of the Australian Diabetes Society. Dr Jalleh: None.