Diabetes in older people: how does management change?

Diabetes type 2
Diabetes medicines
Diabetes in older adults is a growing health burden in Australia and presents various challenges. The heterogeneity of older people, ranging from the robust to the frail, should be strongly considered when developing treatment goals and strategies. Diabetes care in older people generally has a greater emphasis on maintaining quality of life, delivering personalised care, achieving comfort, and preventing symptoms and acute complications of hyperglycaemia.
- The heterogeneity of older individuals merits strong consideration when establishing treatment goals and strategies.
- Older adults with diabetes are more susceptible to adverse drug effects, hypoglycaemia and infections due to a myriad of factors.
- Clinical manifestations of diabetes in older people are atypical.
- Diabetes care in older people typically has less emphasis on strict numerical targets and more focus on symptomatic wellbeing, avoidance of treatment complications, personalised care, pharmacovigilance and rationalisation of medications.
- Therapeutic agents with proven tolerability and safety, and minimal hypoglycaemic risk should be preferred.
- Individualised therapeutic approaches and glycaemic target ranges are crucial in providing safe and effective diabetes care to older people.
Australia’s population is ageing as a result of increasing life expectancy.1 The expected dramatic rise in the number of older adults living with diabetes over the next few decades is a cause for considerable concern for healthcare systems here and around the world. The distinct metabolic characteristics of older adults, coupled with the paucity of data for diabetes care in older people due to under-representation in clinical trials, pose challenges to determining safe and effective intervention strategies for diabetes in the older age group. The heterogeneity of older individuals is essential to consider when establishing treatment goals.2,3 This article describes the salient features of diabetes in older adults and delineates key issues in the management of older people with diabetes.
Definition of older people
Most developed countries including Australia have accepted the chronological age of 65 years as a definition of ‘aged’ or older person.4 In 2017, 15% of the Australian population (3.8 million people) were aged 65 years and older. However, it is projected that 22% (8.8 million people) and 25% (12.8 million people) of the population will be aged 65 years and over by 2057 and 2097, respectively.1 As ageing progresses, clinical characteristics of older people and pathophysiological changes vary by age. Thus, the older age group can generally be divided into young-old (65 to 74 years), old (74 to 84 years), and old-old (over 85 years) given the diversity of old age.5
Epidemiology of diabetes in older adults
The prevalence of diabetes among adults in Australia aged 65 years and older has doubled over the past two decades, with an estimated one in six adults in this age group being affected.1 The rising epidemic of diabetes in older people is attributable to an ageing population and other factors such as an increased prevalence of risk factors, greater public awareness and better diabetes detection methods.
The incidence of diabetes (new cases over time) tends to increase with age whereas the prevalence (proportion in the population) of all types of diabetes is highest in people aged 85 years and older, closely followed by the 75- to 84-year-old age group, according to reports published by the Australian Institute of Health and Welfare.1 Older adults may be diagnosed with diabetes incidentally after the age of 65 years or may have had longstanding disease diagnosed in middle age or earlier.6
In line with the general population, type 2 diabetes is the most common type of diabetes in people aged 65 years and older, accounting for more than 90% of cases.1 Due in part to the success of modern diabetes management, people with type 1 diabetes are living longer, contributing to the growing population of older people with type 1 diabetes.7
Presentation of diabetes in older people: how do they differ?
The clinical presentation of diabetes in older people may be insidious and patients may present with vague symptoms such as fatigue, weight loss or mood changes.8,9 Up to half of older people with diabetes are unaware of their illness, suggesting that the usual symptoms of hyperglycaemia are not often present in this population. Potential contributory factors include a higher renal threshold for glucose in older people and thus glycosuria may not develop until the blood glucose concentration is significantly elevated.2,8
As thirst mechanisms can be impaired with ageing, polydipsia may be absent in older people with marked hyperglycaemia. More often than not, diabetes presents for the first time in an older person who is hospitalised with a condition that may be related to diabetes, such as a stroke, myocardial infarction or foot infection. In frail older nursing home patients, hyperosmolar hyperglycaemic state may be the first sign of diabetes.3,10 Furthermore, the signs and symptoms of hyperglycaemia can be obscured by cognitive changes and dementia.
Geriatric syndromes occur at a higher frequency in older adults with diabetes and can have an impact on independence, chronic disease self-management and quality of life (Box).6,11 Diabetes can contribute to these syndromes, either directly through its complications or by delaying the resolution of other comorbid conditions. The coexistence of these conditions poses additional challenges and complexities in the provision of diabetes care to older adults.9,11
{kind=link}
Considering the atypical and less classic presentation of diabetes in older people, clinicians should maintain a high index of suspicion for diabetes in the assessment of older patients presenting with nonspecific symptoms.
Older adults with diabetes are at higher risk of microvascular and macrovascular complications, potentially owing to the more prolonged duration of disease and decreased end-organ reserve due to concomitant comorbid illnesses. They may also experience more abrupt and severe end-organ disease. Furthermore, adults older than 75 years with diabetes are more likely to have higher rates of death from hyperglycaemic crises and an increased rate of emergency department presentations for hypoglycaemia.12,13
As we become more successful at increasing longevity in people with diabetes, hypoglycaemia may emerge as a dominant sequela in older people, and the risk increases exponentially with age. The reduced counter-regulatory glucagon response to hypoglycaemia due to ageing renders older adults susceptible to hypoglycaemia.3 Besides, other factors often seen in older people, such as polypharmacy, reduced clearance of antihyperglycaemic agents due to impaired kidney function, erratic eating patterns and cognitive impairment, can also contribute to the increased risk of hypoglycaemia, which is associated with an elevated risk of falls and fall-related injuries.14,15 In addition, symptoms of hypoglycaemia change with age and can be atypical in older people.
Screening for diabetes in older adults: what are the pitfalls?
Glucose tolerance progressively declines with age due to alterations in glucose homeostasis. Loss of first-phase insulin release secondary to defective carbohydrate metabolism, as well as impaired beta-cell compensation to age-related insulin resistance, lead to postprandial hyperglycaemia, a pathognomonic feature of diabetes in older adults.16,17 This explains why isolated postchallenge hyperglycaemia, defined as an elevated two-hour glucose level using the oral glucose tolerance test (OGTT) with a normal fasting plasma glucose level, is particularly common in people above 60 years of age.16 OGTT detects many more older adults with undiagnosed diabetes mellitus who would otherwise be missed compared with using fasting plasma glucose testing alone.2
A glycated haemoglobin (HbA1c) level of 6.5% (48 mmol/mol) can be used to establish the diagnosis of diabetes.18 HbA1c reflects the average plasma glucose concentration over the preceding two to three months, which is the lifespan of the red blood cells.19 Therefore, some of the factors often seen in older people such as anaemia, recent blood transfusion, chronic kidney disease and erythropoietin therapy can affect red blood cell lifespan and falsely lower HbA1c. If any of these conditions are thought to exist, the diagnosis of diabetes should be made on measurement of blood glucose levels.12,20
In view of the aforementioned factors, one-third of older individuals with diabetes are undiagnosed when HbA1c or fasting plasma glucose level is used as a screening modality.6 Therefore, an OGTT may be a better screening test for diabetes in this age group.9,14 However, practical issues such as pretest preparation, overnight fasting and poor tolerance should be taken into account when referring older adults for an OGTT.20 On balance, the current NHMRC guidelines used for screening diabetes in the general population should also be used in older people.21
Therapeutic options for older people with diabetes
Nonpharmacological and pharmacological therapies for diabetes in older age do not differ fundamentally from treatment for younger adults.9,14 In February 2020, the Australian Diabetes Society released a revised treatment algorithm and a summary of available therapies for type 2 diabetes for the general population, outlining the properties, benefits, risks and costs of each drug class and providing an approach for incorporating older and newer agents (see: http://t2d.diabetessociety.com.au/plan/).22
Lifestyle modification is important for patients of all ages with diabetes. Very restrictive diets are not recommended for older adults and advice to avoid large carbohydrate loads at any one meal can reduce glucose excursions. Physical activity is an integral part of diabetes management even in older people, and should be guided by patients’ functional capacities.12,23 Type 2 diabetes with onset later in life is characterised by defects in beta-cell function, suggesting therapeutic attention to beta-cell function and adequacy of insulin release, along with a focus on insulin resistance and hepatic glucose overproduction.
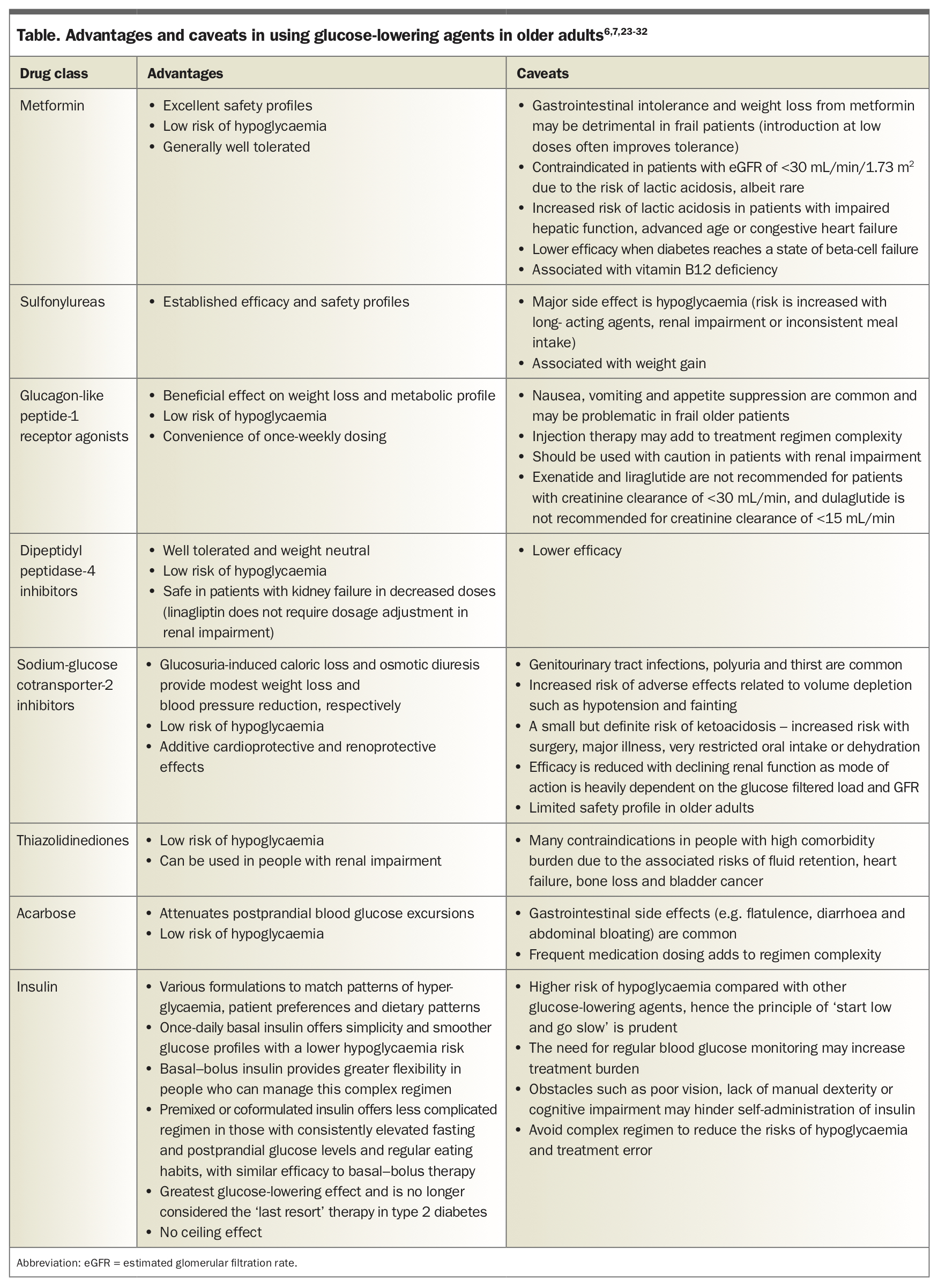
Older patients are at increased risk of adverse drug effects due to age-related changes in pharmacokinetics (reduced renal elimination) and pharmacodynamics (increased sensitivity to medications), potentially compounded by polypharmacy.6 It is essential for healthcare providers to be cognisant of these factors as well as the pros and cons of each drug class to help develop suitable pharmacotherapeutic strategies.12 An overview of the age-specific factors that should be considered when selecting glucose-lowering therapy for older patients, outlining the advantages and caveats in using these agents in the older population, is shown in the Table.6,7,23-32
{kind=link}
Certain groups of glucose-lowering medications need to be used with extreme caution in older people. Sulfonylureas should generally be avoided in patients with frailty, irregular eating patterns or impaired kidney function due to the increased risk of hypoglycaemia.6,24
Acarbose is unpopular with patients due to its common gastrointestinal side effects and frequent medication dosing.
Thiazolidinediones are the less preferred oral agents nowadays as they are associated with weight gain, fluid retention, heart failure, bone loss and possibly bladder cancer, so may not be suitable for use in older adults.6
Vigilance is needed when using sodium-glucose cotransporter-2 (SGLT-2) inhibitors in people with advanced age due to the increased risk of genitourinary tract infections, urinary frequency, ketoacidosis, dehydration and orthostatic hypotension with resultant falls.12,23 Furthermore, the use of SGLT-2 inhibitors in older people is not recommended in the product information of this class of drugs.
When prescribing insulin therapy in older adults, due consideration should also be given to the risk of hypoglycaemia and obstacles that hinder insulin self-administration. Cognitive impairment can interfere with the ability to safely administer insulin therapy. The use of insulin therapy requires that patients or their caregivers have good visual and motor skills as well as cognitive ability.6
Principles and treatment goals of diabetes in older adults
Diabetes management in older people requires regular assessment of various domains and it is increasingly important that treatment of diabetes in older people is more closely aligned with individual characteristics.3,7 As far as possible, treatment should be simple, with minimal treatment burden and tailored to a patient’s individual needs and preferences. Attention to the selection of medications with a strong benefit-to-risk ratio is crucial to promote efficacy and safety.6
Management of diabetes in older people generally has a greater emphasis on maintaining a patient’s quality of life, delivering personalised care, achieving comfort, and preventing symptoms and acute complications of hyperglycaemia. Intensive glycaemic control may increase the risk of adverse events and mortality, and only reduces microvascular rather than macrovascular complications.9,33 Overtreatment of diabetes in older people is common in clinical practice and should be avoided. Periodic adjustment of glycaemic goals and deintensification of treatment regimens based on comorbidities and functional status are essential.
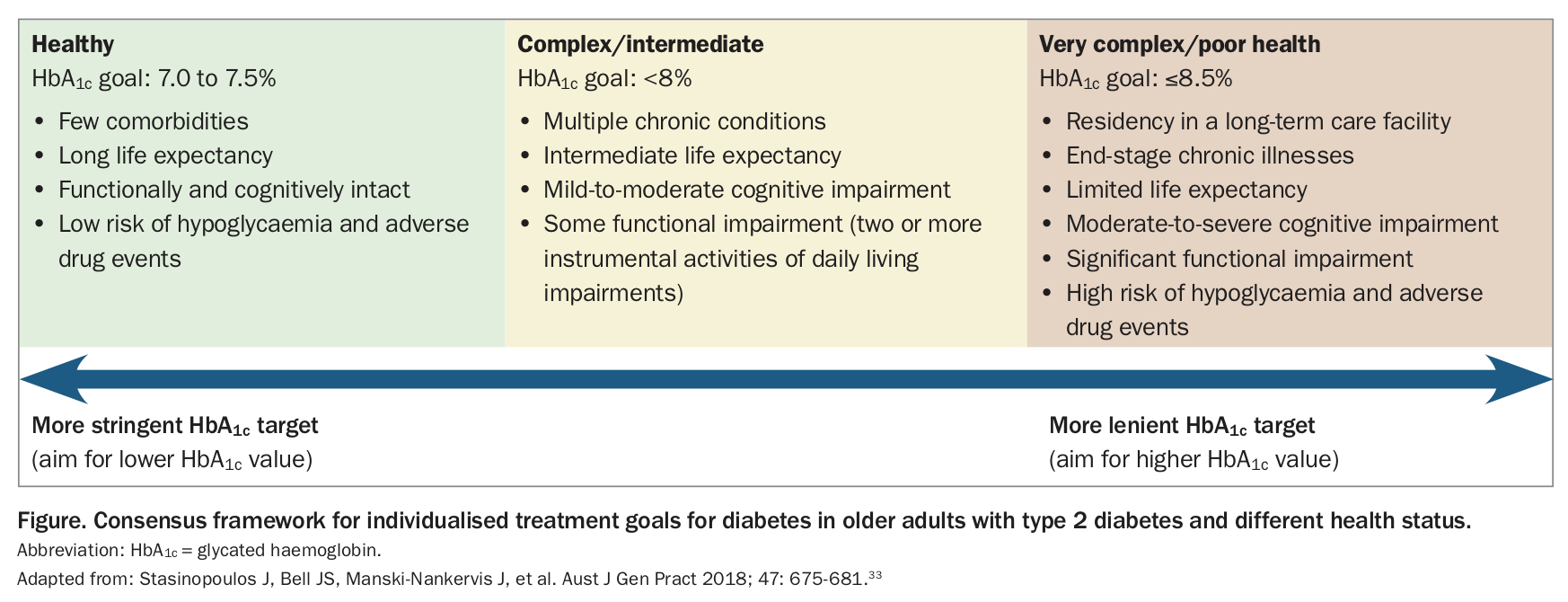
Along with recommendations from major international organisations,7,34,35 local guidelines from the Australian Diabetes Society, Diabetes Australia and the McKellar Centre recommend personalised HbA1c targets based on comorbidity profiles, functional status and life expectancy (Figure).33,36-38 Based on these parameters, older patients are divided into three major health categories: those who are relatively healthy; those with complex comorbidities in whom self-care may be difficult; and those with very significant multimorbidity and functional impairment. The suggested blood glucose target range for most older people is 6 to 15 mmol/L, although this should be tailored to each individual.37 The fundamental aims are avoiding hypoglycaemia and preventing symptoms of hyperglycaemia.
{kind=link}
The management of diabetes in the long-term care setting has its own challenges and the treatment of older people with diabetes receiving palliative care is unique. Strategies for diabetes management in these settings include relaxing glycaemic targets, decreasing complexity of treatment, using low-risk medications and individualising treatment. It is crucial to have timely discussions about the goals and intensity of care, individual preferences, advance care directives and ethical issues. Early identification of older adults who require end-of-life care is crucial, with a view to promoting comfort, controlling symptoms, and preserving dignity and quality of life. It is important to respect a patient’s wishes to withdraw therapy if desired in the setting of palliative care. Many older adults with diabetes rely on their family members or next of kin to help them with their treatment decisions or administration of daily treatments. Family carers may be more familiar with the management of their relatives’ diabetes than healthcare providers and can often provide important information when they are involved in the decision-making process.
Conclusion
Older adults with diabetes are a heterogeneous population ranging from the robust to the frail and represent unique challenges for patients, healthcare providers and families. Recognising the contemporary clinical course of diabetes in this population is crucial for establishing evidence-based clinical practice recommendations, identifying research priorities and setting healthcare policies. Clinicians should be vigilant of the clinical, functional and psychosocial aspects when developing treatment plans for patients in this age group while preserving quality of life. Treatment regimens must be individualised, simple, sustainable and safe to best mirror patients’ preferences, wishes and needs. ET