Diabetic foot disease – managing cardiovascular risk

Diabetes complications
Diabetic foot disease (DFD) not only causes foot-related morbidity, it is also a marker of elevated cardiovascular risk. Annual foot screening is recommended for all patients with diabetes and presents an opportunity to assess cardiovascular risk. Where possible, patients with active DFD should be referred to a high risk foot service for multidisciplinary specialist care. Managing contributing factors for cardiovascular risk – including controlling hypertension, ensuring statin use, counselling smoking cessation and appropriate physical activity, and tailoring pharmacotherapies for diabetes control to each patient – reduces rates of future cardiovascular events.
- Diabetic foot disease (DFD) causes foot-related morbidity and is a marker of elevated cardiovascular risk.
- People with DFD have a longer duration of diabetes with suboptimal control, elevated blood pressure and lipid levels, prior or current smoking status and higher rates of other diabetes-related complications and previous cardiovascular disease.
- Mortality forth is group is high; however, presentations of DFD – whether acute, with increased frequency of consults, or as part of annual diabetes screening – represent opportunities for clinicians to screen for and address cardiovascular risk factors.
- Improving blood pressure control and prescribing a statin and antiplatelet therapy can significantly reduce long-term cardiovascular disease risk.
- Diabetes and metabolic management should be tailored to each patient’s glycaemic control and diabetes complication status.
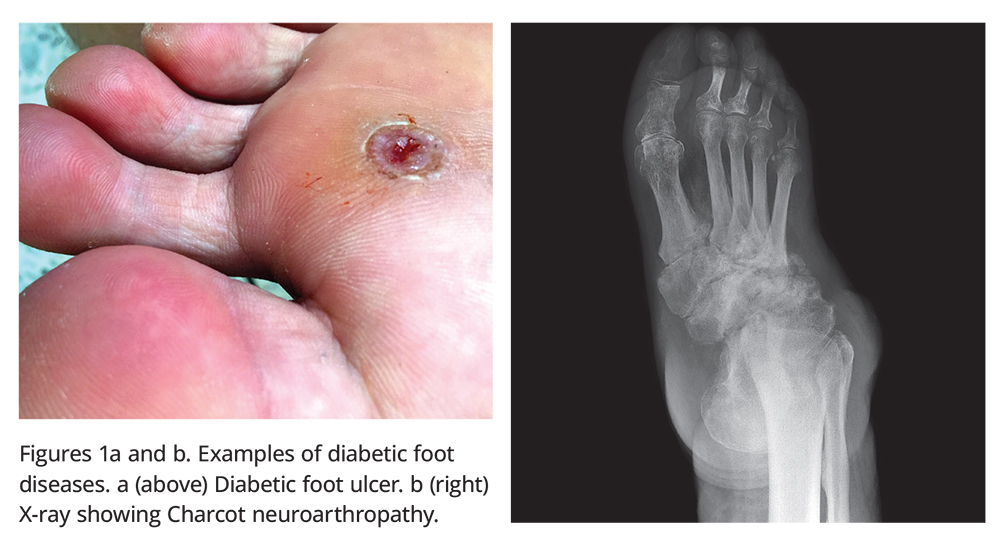
Diabetes mellitus is a well-recognised risk factor for cardiovascular disease (CVD). It is also associated with significant morbid burden from complications of diabetic foot diseases (DFD), with the clinical spectrum ranging from peripheral neuropathy causing significant sensory loss and, in high-risk feet, acute diabetic foot ulceration (DFU); infection; sepsis and lower extremity amputations; and the uncommon but potentially deforming neuropathy/inflammatory condition of Charcot neuroarthropathy (Figure 1). In Australia annually over 27,000 hospital admissions, 4,400 lower extremity amputations and over 1700 deaths are related to DFD.1
{kind=link}
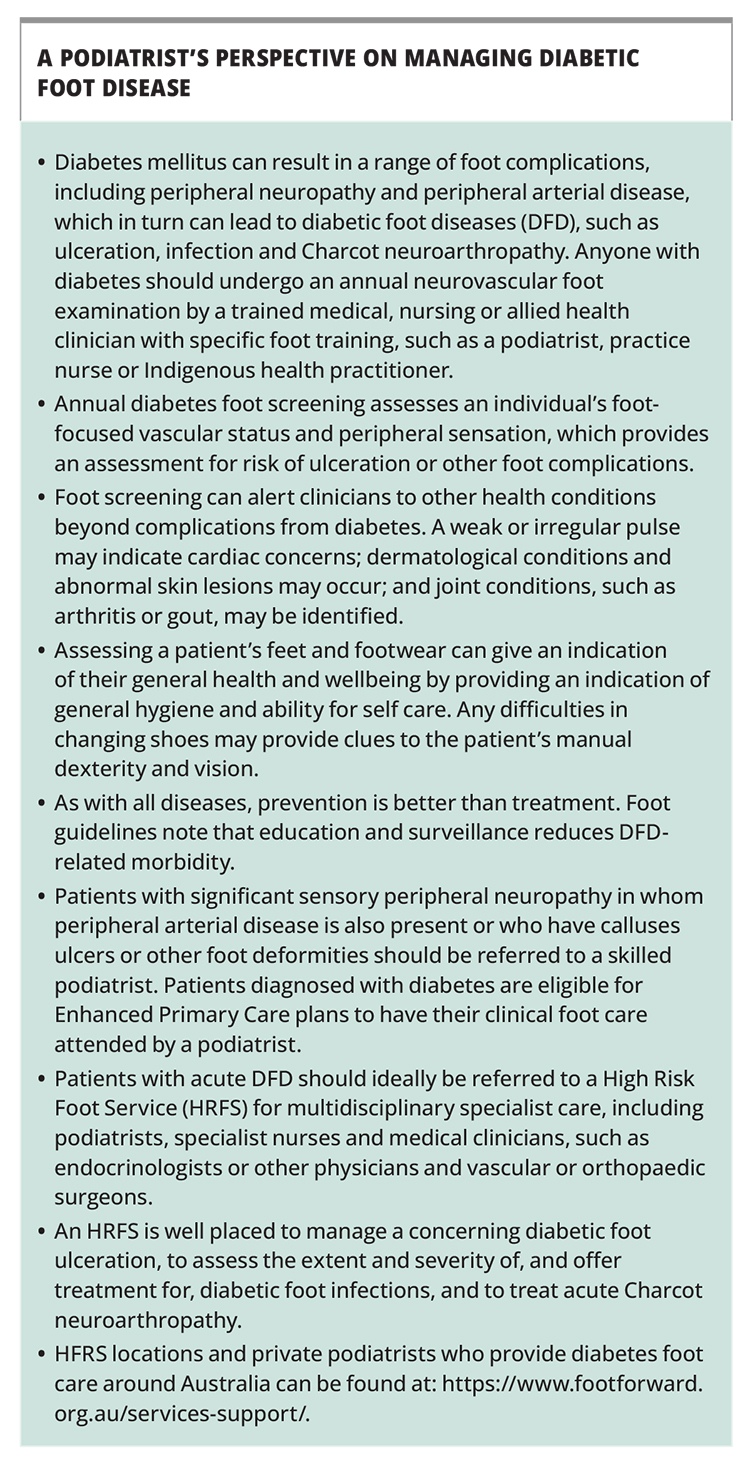
This article outlines the evidence for the association between DFD and CVD risk, and discusses the recommendations for managing CVD risk factors in people with DFD. Anyone diagnosed with diabetes should undergo an annual neurovascular foot exam by a trained clinician, such as a podiatrist and doctor, or nurses and community health workers with specific foot training. Where possible, patients with acute DFD should be referred to a high risk foot service (HRFS) to receive multidisciplinary specialist care, with teams made up of podiatrists, specialist nurses and medical clinicians, including endocrinologists, other physicians and vascular or orthopaedic surgeons. A podiatrist’s perspective on managing DFD is presented in the Box.
{kind=link}
DFD and cardiovascular risk
Beyond foot-related morbidity, the presence of DFD is a significant cardiovascular risk factor. In people with DFD, five-year mortality from CVD conditions approaches 50%, in part due a higher CVD risk burden.2-5 Additionally, there is evidence that the presence of DFD independently elevates cardiovascular risk through influencing immune and inflammatory pathways.6-8 Consistent with these findings, our research examining people with diabetes with or without DFD also found the DFD group associated with higher rates of chronic renal disease, being a current or ex-smoker, and with more elevated blood pressure and lipid levels. Over one-third of the DFD cohort had a cardiac or stroke history and their diabetes was undertreated.9,10 Similar to other studies, our cohort had a higher representation of known at-risk populations, including Indigenous Australians, those from lower socioeconomic backgrounds and those not born in Australia.
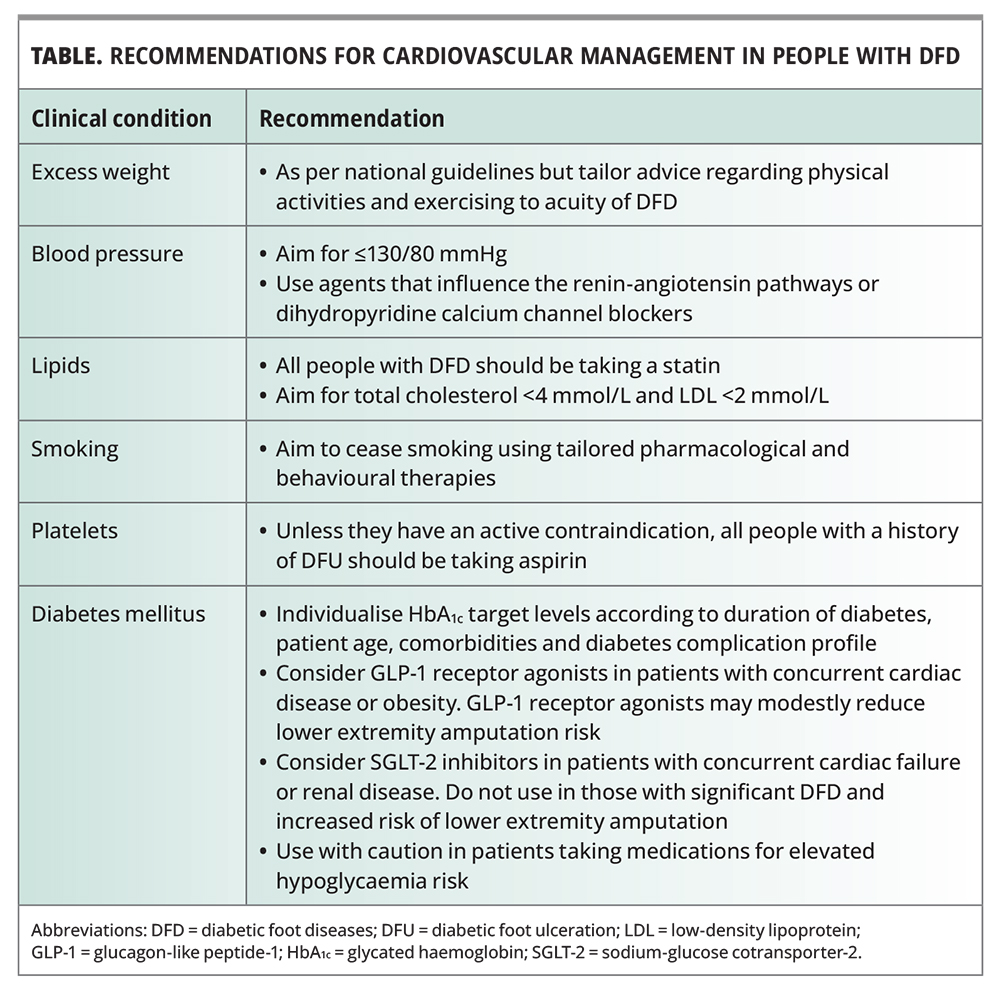
Although international diabetic foot guidelines for managing vascular disease note a lack of evidence for CVD risk management to directly mitigate diabetes-related foot conditions, they emphasise that rigorous treatment of CVD risk reduces CVD-related death, and strongly support prompt investigation and management of cardiovascular risk in people with DFD.11,12 Recommendations for cardiovascular management of people with DFD are summarised in the Table and discussed below.
{kind=link}
Antihypertensive therapy
People with DFD should be treated in accordance with national blood pressure targets for diabetes, with prompt antihypertensive therapy initiated if systolic blood pressure (BP) is 140 mmHg or above.13 One study showed that reducing BP variability, especially systolic BP, and targeting a BP level of 130/80 mmHg and below, reduced the incidence of new onset DFU and for people without any neuropathic or vascular diabetic complications, early use of dihydropyridine calcium channel blockers was associated with a reduced risk of DFU.14 Furthermore, DFD is strongly associated with other diabetes complications, especially renal disease.3,9 Therefore, we suggest using antihypertensive therapies that influence the renin-angiotensin pathways or dihydropyridine calcium channel blockers and to target blood pressure to 130/80 mmHg and lower as a reasonable approach.
Smoking cessation
The deleterious effects of regular cigarette smoking, as well as the importance of smoking cessation, on rates of new or relapse DFU and ulcer healing, and the relationship between cigarette smoking and the whole gamut of diabetes- and CVD-related complications, are well established.15 People with DFD should be strongly encouraged to use the well-validated strategies of behaviour therapy and pharmacological support to assist them to stop smoking. Behaviour therapies include government initiatives such as the My QuitBuddy app and support services such as Quitline. Pharmacotherapies to help quit smoking include nicotine replacement therapy in the form of patches, gums, sprays and inhalers, and a range of prescription medicines that reduce the craving for nicotine, which, to the authors’ knowledge have no specific guidelines relating to their use in people with DFD.13 Choice of pharmacotherapy is guided by individual preferences and clinical considerations.
Antiplatelet therapy
There is good evidence that routine use of antiplatelet (and statin) therapy reduces CVD-related mortality in people with DFU and, unless contraindicated, all people with a history of DFU should be commenced on antiplatelet therapy.12 For people with DFU alone, and no known CVD or other indications for specific antiplatelet therapies, there is little evidence to guide the choice of antiplatelet therapy or to support using novel anticoagulant agents over other antiplatelet drugs. For such patients, we suggest a clinical review of their medical history to exclude those at elevated risk of bleeding events and to consider initiating aspirin therapy for all other patients.
Lipid lowering therapy
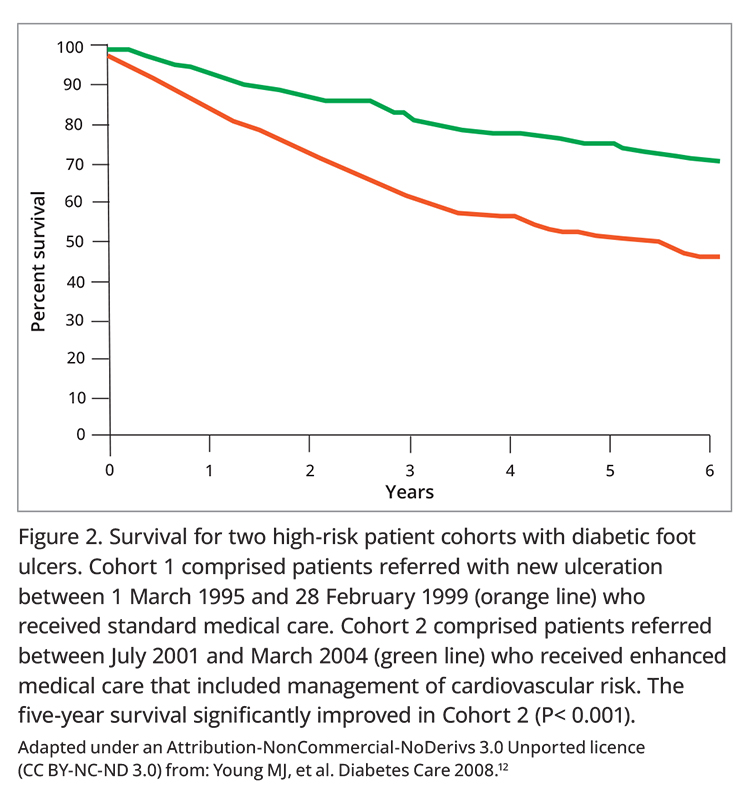
Diabetic foot guidelines recommend that all people with DFD be prescribed a statin agent.11 These recommendations are based on the same landmark study that showed high rates of statin and antiplatelet use were among the key management tools that achieved an almost 50% decrease in the five-year CVD mortality of people with DFD (Figure 2).12 Lipid targets levels should follow national guidelines, including:
{kind=link}
- total cholesterol below 4.0 mmol/L
- low-density lipoprotein levels below 2.0 mmol/L and below 1.8 mmol/L if CVD is present
- high-density lipoprotein level 1.0 mmol/L or higher.13,16
There is some evidence that achieving at-target total cholesterol levels may contribute to measured reduction in CVD mortality.12 There is currently no data to support greater efficacy from nonstatin lipid agents in terms of CVD risk in people with DFD and we recommend all people with DFD be prescribed a statin.
Lifestyle management and physical exercise
Overweight and obesity are strongly linked to type 2 diabetes and lifestyle management that incorporates dietary change, increased incidental activity and regular exercise remain the cornerstone of obesity management.17 However, in the presence of DFU, reducing the trauma of pressure to the feet is a cornerstone of DFD management. As such, we recommend that people with overweight or obesity who have DFUs should be encouraged to undertake nonambulatory forms of exercise, such as the use of resistance bands and weights. Water-based exercise should not be recommended until DFUs are healed.
Glycaemic control and therapeutics
The latest national and international diabetes management guidelines for both type 1 and type 2 diabetes emphasise individualising glycated haemoglobin (HbA1c) targets according to clinical parameters that include age, duration of diabetes, the risk from hypoglycaemia events and diabetes complication and other comorbidities.13,16,18,19 The average patient attending our HRFS has type 2 diabetes with advanced DFD, is older and has an extensive CVD and diabetes complication profile when compared with those attending our diabetes clinics. Clinically we individualise their HbA1c targets according to these parameters.9,10
Over the past decade, the range of therapeutics available for the management of type 2 diabetes has increased and, as per the most recent management guidelines, the choice of second-line diabetes agent after metformin should account for glycaemic efficacy and cardiac or renal risk, other metabolic parameters and the risk of side effects or harm from the therapy. For our own clinical practice, after metformin we favour using the weekly glucagon-like peptide-1 (GLP-1) receptor agonists, oral dipeptidyl peptidase-4 (DPP-4) inhibitors and, with caveats, sodium-glucose cotransporter-2 (SGLT-2) inhibitors as per the patient’s clinical profile and current national prescribing guidelines. We are mindful of the risk of harm from hypoglycaemia associated with insulin and sulfonylurea use.
Glucagon-like peptide-1 receptor agonists
Two recent meta-analyses assessed the use of GLP-1 receptor agonists, SGLT-2 inhibitors, DPP-4 inhibitors and sulfonylureas in lowering the risk of extremity amputation. The analyses cautiously found that GLP-1 receptor agonists may be more effective than the other agents, especially SGLT-2 inhibitors in reducing amputation risk.20,21
Sodium-glucose cotransporter-2 inhibitors
The most recent TGA criteria allow SGLT-2 inhibitors to be prescribed for specific cardiac and renal indications, which increases their flexibility for use alongside the other novel diabetes agents. However, at least one type of SGLT-2 inhibitor, canagliflozin, is clearly associated with an increased risk of lower extremity amputation in patients with prior amputation, peripheral vascular disease or neuropathy.22,23 A pharmacological data driven cohort analysis of lower limb amputations found lesser and attenuated associations for empagliflozin and dapagliflozin, respectively.24 Our own practice is to withhold or stop any prescribed SGLT-2 inhibitors for people with DFU and an elevated risk for lower extremity amputation (i.e. presence of known PVD, prior amputation history, recurrent ulceration) and for those with any significant diabetic foot infection. When the foot wounds have completely healed, we reassess patient safety to restart SGLT-2 inhibitors.
DFD is an opportunity to manage cardiovascular risk
People with DFD attend their primary health practitioners to manage other comorbid conditions as part of their diabetes cycle of care (which includes regular foot screening) or to assess a new DFU, foot infection or as part of ongoing care for chronic DFD. Although we have previously noted the value of a specialist HRFS, primary health practitioners are a key partner for the long-term management of DFUs and infections as these conditions need increased clinical contact to review the ulcer, assist in wound dressing and to assess the efficacy of antimicrobial therapies. These interactions represent opportunities for clinicians to review their patient’s cardiovascular risk profile and management, and increased frequency of clinical visits allows the v to sequentially or concurrently refine the management of the patient’s individual CVD risk factors.
In our own practice, as part of the initial review of acute DFD presentations, we monitor blood pressure and measure baseline lipid and HbA1c levels to determine the need to initiate blood pressure targets and revise or refine statin and glycaemic therapies. We take a smoking history and encourage smoking cessation. We also review antiplatelet therapy and, if the patient is not on therapy, review any contraindications to initiating aspirin. Lifestyle advice to help manage overweight and obesity, including acceptable physical activities, is tailored to each patient’s acute DFD presentation.
Conclusion
People with DFD face an increased burden of diabetes complications and CVD risk factors and conditions. Although these patients are at very high risk for future CVD events, there is good evidence that prompt and aggressive CVD risk modification, incorporating blood pressure control, lipid-lowering and antiplatelet therapies and smoking cessation, can nearly halve future CVD events. Diabetes therapeutics should be reviewed according to a patient’s glycaemic control and diabetes complication status. Management may need to be altered for those with an active diabetes foot infection and elevated risk of lower extremity amputation. MT
COMPETING INTERESTS: Dr Lau reports honoraria for educational sessions from AstraZeneca and Eli Lilly. Ms Shwarzer: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.