Diabetes-related foot ulcers: the role of pressure offloading

Diabetes complications
Ulcers will not heal if subjected to repetitive trauma. Individualised wound-management plans must prioritise identification and management of infection, ischaemia and trauma. Prevention and management of diabetes-related foot ulcers also relies on reducing trauma to the foot, particularly through pressure offloading.
- Most foot ulcers are related to neuropathy, which reduces sensation in the feet and hence patients will be unaware of the harm they do by continuing to walk on an ulcer.
- It is not generally recommended that a patient continues to wear their regular footwear when they have an active foot ulcer.
- Treatment for foot ulcers comprises individualised strategies including reducing walking, using a pressure-offloading device and gaining a commitment from the patient to wear the device.
- If the wound is on the plantar aspect (sole) of the foot, a total contact cast or removable cast walker (ideally rendered irremovable), if they can be worn safely, are used in conjunction with an insole.
- Most podiatrists have some expertise in treating foot ulcers but it is recommended they enlist the care of a specialised multidisciplinary high-risk foot service if it is available at the local public hospital.
- Ulcer recurrence is common; long-term foot protection including appropriate footwear, regular treatment by a podiatrist, ongoing foot checks and education is needed.
If a patient with diabetes mellitus presents with a foot ulcer or signs of tissue injury of the foot, the GP has a valuable opportunity to reduce the risk of more harm. The natural history of diabetes-related foot ulcers is often one of delayed presentation with infection and ischaemia, associated with poor prognosis.1 Typically, the underlying peripheral neuropathy causes loss of protective sensation, which impairs the patient’s ability to recognise injury to their feet, whether it is chronic pressure leading to callus or a more acute injury such as a footwear rub or a burn. Furthermore, when a foot lesion becomes infected, loss of sensation masks the presence and severity of infection and ulceration from the patient, leading them to delay seeking treatment. Much of the morbidity, cost and lost quality of life associated with foot ulcers and amputation can be avoided with early detection. Useful evidence-based practice guidelines for assessment, prevention and management of diabetic foot disease are freely available (Box).
{kind=link}
Early prevention
Stepping back, the opportunity for early detection starts with annual foot screening. Education in foot care and daily self-checks and preventive treatment are recommended for people with diabetes who are screened and found to have ‘at risk’ feet. The most important predictor of future foot ulceration is past ulceration; but when there is no previous ulcer history, the most important risk factors are loss of protective sensation, foot deformity and/or ischaemia. Instituting regular foot checks for people known to be at risk means both the patient and doctor are alert to the possibility of foot ulceration and the need to present early for treatment.
Treatment approach
Once a foot ulcer is identified, the key principles for treatment are:
- identify and mitigate infection, ischaemia and trauma
- provide local wound care involving skilled sharp debridement (when there is adequate blood flow), cleaning and dressing of the wound.
Education, psychological support and modification of other factors such as poor metabolic control and nutrition also play a part in successful treatment.
Large or complex wounds associated with ischaemia or deteriorating infection, or ulcers that fail to reduce in size in the initial couple of weeks should be referred to a specialised multidisciplinary team, such as a high-risk foot service or wound clinic if available locally.2 High-risk foot services operate in most major hospitals.
The recurrence rate for diabetes-related foot ulcers is around 50%, meaning lifelong foot protection is needed after healing.3,4 This article addresses the role of pressure offloading in promoting healing and preventing recurrence of foot ulcers in patients with diabetes.
Overarching principles of offloading to protect an ulcer from trauma
Offloading strategies aim to protect an ulcer from trauma to promote healing. The strategy is individualised to the patient’s clinical presentation, taking into account ulcer location, foot biomechanics, balance and mobility, together with their circumstances (e.g. work) and addresses the overall cumulative stress on the ulcer. Burns (such as from heaters or walking on hot surfaces) often present initially as blisters, and infection and deeper tissue injury are seen subsequently. Like ulcers, burns also need protection from trauma.
Cumulative stress is considered to be the pressure (force over area) on the ulcer combined with the amount of time the patient spends walking and standing on the foot.5 A device that can offload pressure from the ulcer site needs to be prescribed and fitted. To reduce stress overall, the device must be worn (virtually always) and weight-bearing activity minimised. Sheer stress is less measurable but is also likely to cause harm and needs to be considered.
Adherence with wearing the device is made difficult by loss of sensation, which reduces postural stability and impacts the way patients perceive their ulcer and the need for treatment.6 Although some will follow treatment advice, it is more common for people with neuropathy not to understand the need for offloading and to resist making changes that are difficult to make. People with poor mobility or postural stability will have more difficulty with some devices and may need additional aids such as walking frames to support the overall strategy and prevent falls. These devices include casts and removable walking braces. The high prevalence of mental health problems and cognitive impairment in patients with diabetes-related foot complications means that clinicians need to be alert to this and consider the impacts on health literacy and capacity to adhere with treatment plans.
To gauge the success of offloading treatment and to set treatment goals, ulcer size should be measured and recorded. Aim for a weekly reduction in wound size as this is predictive of healing.7 If the wound size is not reducing, review all aspects of treatment and/or refer the patient for more specialised care.
Toe and nonplantar forefoot ulcers
Footwear is a frequent cause of injury to the dorsum of toes (over the interphalangeal joints), medial aspect of the first metatarsal head and lateral aspect of the fifth metatarsal. Clawing of the toes, common in older people and those with diabetes, is caused by muscle imbalance. The tops and end of clawed toes are exposed to trauma in regular-fitting shoes. Ulcers between the toes may be due in part to footwear, but interdigital tinea pedis and secondary bacterial infection can also contribute to tissue breakdown. The offending shoes must not be worn (and preferably be discarded) and a healing sandal or postoperative shoe be worn until the wound heals (Figure 1). Patients will often have difficulty accepting that their regular footwear has caused harm, but the need to eliminate the causative footwear is urgent. Toe ulcers are close to bone and can deteriorate rapidly. Ulcers on the back of the heel where shoes can rub require the same approach.
{kind=link}
Offloading plantar (except heel) ulcers
Injuries and ulcers on the plantar aspect of the foot represent half of all ulcers. Trauma can be acute (for example a penetration injury) or chronic (from an area of high pressure).
Penetration injury may have a small portal of entry but, as with burns, deep tissue injury and infection become evident in the ensuing days, hence close follow up is needed. If the injury is to a nonweight-bearing structure (e.g. the arch) then a healing sandal may suffice for offloading.
Chronic repetitive plantar pressure results in skin callus build up, which if left untreated may progress to ulceration. The presence of callus over or around an ulcer indicates that repetitive trauma is the cause. Offloading starts with complete debridement of callus (Figures 2a and b). Notably, this step, which is best performed by the podiatrist, will reveal the true extent of ulceration and may lead people to assume incorrectly that debridement was the cause. If severe arterial disease is suspected on clinical assessment (pedal pulses must be palpated as a minimum), hold off from debridement and urgently seek the opinion of a vascular specialist.
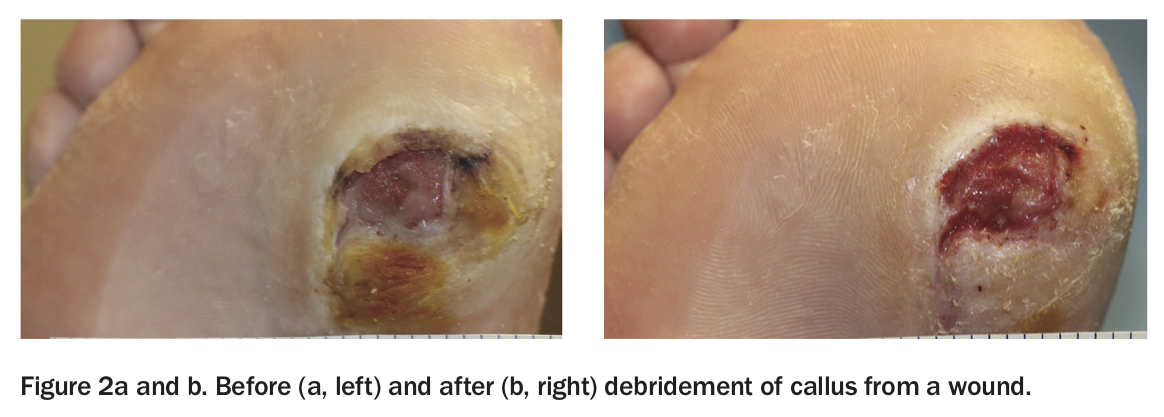{kind=link}
There is good evidence that both total contact casts (TCCs) and removable cast walkers (RCWs), with the addition of a suitable insole, offload and facilitate healing. Techniques which render the ‘removable’ cast walker irremovable force adherence and increase efficacy.8,9
A TCC redistributes pressure and may reduce the overall force to the foot. Furthermore, patients cannot remove the cast and will reduce their activity. In practice, TCCs require access to equipment and skilled practitioners such as podiatrists working specifically in this field. TCCs are provided by high-risk foot services. They carry some risk of iatrogenic trauma and are not suitable for or tolerated by all patients, such as those with poor balance or those who must continue to drive. They are traditionally changed weekly, but some are made removable. Patients using TCCs or RCWs cannot drive with the device and must take extra precautions to avoid falls and keep the cast dry.
RCWs can be applied with less skill than TCCs, and are therefore more widely accessible, but may not accommodate all foot shapes safely (Figures 3a and b). The risks and patient advice are otherwise the same as for TCCs.
{kind=link}
If the wound is large or deep, or associated with significant deformity, consider referral to a service that can provide a TCC or RCW, but in the interim a postoperative or healing sandal with a cushioned sole can be issued. This must only be used in combination with minimal weight-bearing. Both TCCs and RCWs provide superior offloading to healing sandals in protecting the foot, if tolerated.10
Other options for offloading plantar ulcers
When the offloading methods mentioned above cannot be used, consider the following practical alternative solutions.
- Small (<1 cm), shallow ulcers, uncomplicated by arterial disease and without undermining may benefit from therapeutic felt deflective padding kept dry and reapplied every four to seven days.11,12 Although commonly used, the risks of felt involve transfer lesions if not correctly applied, and maceration and skin breakdown if they get wet and are not removed. Some experience is needed to apply felt padding safely.11,12
- Cushioning insoles provide some pressure relief. Suitable products include 7 mm orthotic urethane foam (Poron) alone or with polyethylene foam (Plastazote), available commercially alone or in combination; however, a custom-moulded orthosis which accommodates the foot shape and provides some pressure relief is superior.13,14
Felt, cushioning and custom orthoses can rarely be fitted into a regular shoe; hence, they are used in combination with healing sandals or an RCW. These devices need to accommodate the bulk of the paddings and insoles and can work well in combination.
Surgical offloading, through the surgical correction of specific foot deformities, may be considered in some cases.10
Plantar heel ulcers
There is less evidence for methods of offloading plantar heel ulcers and potential for worse prognosis. It is almost impossible to avoid walking on the heel. Careful use of cushioning and arch fill may transfer some load to the midfoot, and RCWs and casting are sometimes used; however, complete offloading of the heel with bedrest, wheelchair or knee-scooters may be needed. Escalate for more specialised care rapidly if there is no improvement.
Footwear, education and podiatry
Once healed, patients can return to wearing appropriate sports or ‘comfort’ footwear. To minimise the risk of ulcers from new footwear, professional fitting, use of socks and gradual wear-in are important.
If the shape of the foot, toe height, increased width, or hallux valgus or other deformities prevent the foot from being safely accommodated in these shoes, then medical grade footware (MGF), either off the shelf or custom made, is indicated (Figures 4a and b). MGF is designed to fit abnormally shaped feet and can be modified to alter pressure distribution.15,16
{kind=link}
Patients often do not accept the transition to MGF and may not understand the benefits, so education is important. A well-informed compromise may be better for patients who are unwilling to wear MGF, as they can only be of benefit if worn most of the time.
Custom insoles to accommodate and cushion pressure areas are often needed and are best supplied together with MGF to optimise effectiveness. Podiatrists, orthotists and pedorthists are trained in prescribing (and/or fabricating), supplying and fitting orthoses and MGF.
The cost of MGF is high and obtaining funding requires a good understanding of local criteria and processes. Involving a podiatrist who is experienced in this area is important. Options that may be available to patients include state government-funded equipment and mobility schemes (e.g. ENABLE in NSW), supplementary services for Aboriginal people, My Aged Care and National Disability Insurance Scheme funding, private health insurance rebates and Department of Veterans’ Affairs funding.
Conclusion
Regular treatment and prevention of preulcerative pathology such as callus, heel fissures and pathological toenails by a podiatrist, together with self-care education and foot checks by all members of their health care team is recommended for lifelong foot protection in people with diabetes. ET
COVID-19 and diabetes-related foot ulcers
In the context of COVID-19 impacts on healthcare services, the need for identification and management of diabetes-related foot ulceration remains constant to avoid unnecessary hospitalisation. Some useful resources, provided by the authors of this article, are listed in the Box.
{kind=link}
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.