Thyroid nodules: benign or potentially malignant?

Dr Wang is Endocrinology Advanced Trainee in the Department of Endocrinology and Diabetes at Eastern Health, Melbourne. Associate Professor Wong is Clinical Associate Professor (Adjunct) in the Faculty of Medicine, Nursing and Health Sciences at Monash University and Senior Endocrinologist in the Department of Endocrinology and Diabetes at Eastern Health, Melbourne, Vic.
Thyroid cancer
Thyroid diseases
Thyroid nodules are most commonly benign; however, some may be potentially malignant. Avoiding over-investigation of benign nodules while correctly identifying those that may be thyroid cancer is key. In this article, evaluation, management and follow up of patients with thyroid nodules are discussed.
- The evaluation of a patient presenting with a thyroid nodule includes history taking, physical examination, measurement of serum thyroid stimulating hormone levels and thyroid ultrasound examination.
- Patients with a suppressed thyroid stimulating hormone level should undergo 99Tc-radionuclide scanning.
- Patients without a suppressed thyroid stimulating hormone levelor who have ‘cold’ nodules on 99Tc-radionuclide scans should be evaluated with a thyroid ultrasound.
- Thyroid nodule appearance on ultrasound is standardised by using the American College of Radiology Thyroid Imaging, Reporting and Data System (ACR TIRADS) classification system, which guides the need for fine-needle aspiration.
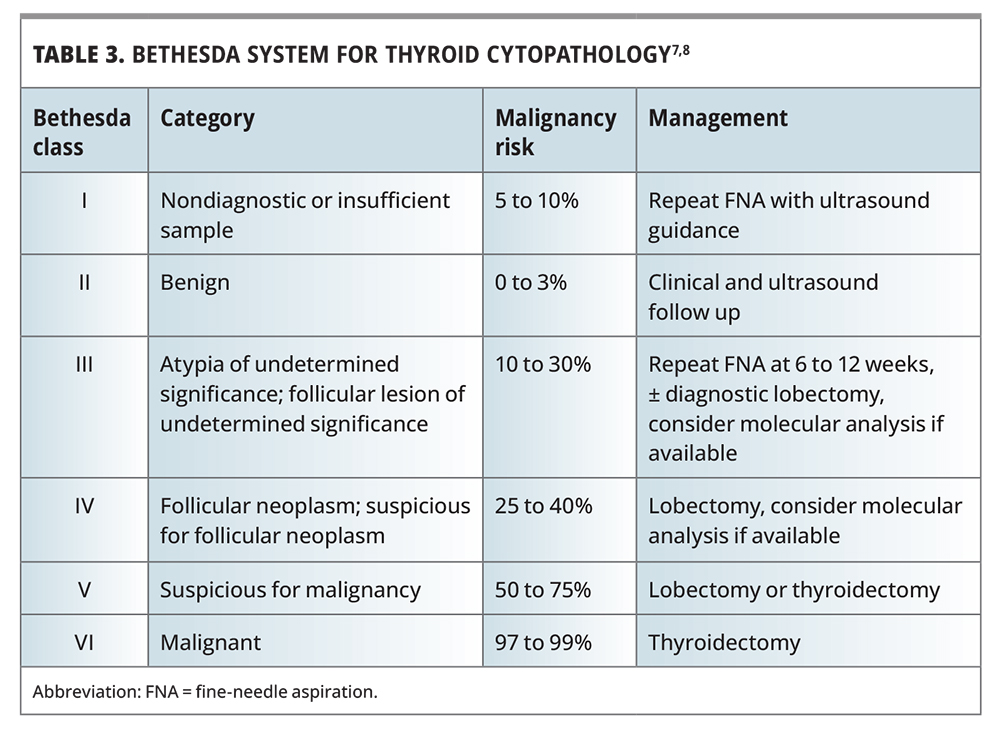
- Fine-needle aspiration results are reported using the Bethesda Criteria to guide subsequent management and follow up.
Patients with thyroid nodules are common in clinical practice, often presenting with a clinically detected nodule or an incidental finding on radiological studies. Thyroid nodules are palpable in 4 to 7% of the population and are visualised in 33 to 68% of people undergoing ultrasound examination, and focal tracer uptake in the thyroid is reported in 2.5% of fluorodeoxyglucose positron emission tomography scans.1-3 Occasionally, patients present because of compressive symptoms. Common causes of thyroid nodules include benign nodules or cysts (80%), benign follicular neoplasms (10 to 15%) and thyroid cancer (5%).4
The management dilemma in people with thyroid nodules is ensuring thyroid cancers are accurately diagnosed and managed in a timely manner, while avoiding unnecessary diagnostic tests or invasive procedures in the majority of patients who have benign nodules. Occasionally, patients experience compressive symptoms from their thyroid nodule, in which case surgical intervention may be warranted regardless of whether the nodule is benign or malignant. This article reviews the evaluation of patients with thyroid nodules and their management.
Initial evaluation of thyroid nodules
The initial evaluation of a patient presenting with a thyroid nodule should include targeted history taking, physical examination, measurement of thyroid stimulating hormone (TSH) level and a thyroid ultrasound examination. After this initial evaluation, nodules that are concerning for thyroid cancer based on ultrasound appearance should undergo fine-needle aspiration (FNA).
History
The key features to elicit on history taking are the presence of any risk factors for thyroid cancer. These include rapid growth of a neck mass, development of a hoarse voice, a history of childhood head or neck irradiation, a family history of thyroid cancer or a cancer syndrome with predisposition to thyroid cancer such as familial adenomatous polyposis, Cowden syndrome and multiple endocrine neoplasia type 2. Other symptoms to enquire about are those of hyper- or hypothyroidism and compressive symptoms such as dyspnoea, dysphagia, a feeling of constriction around the neck or positional neck discomfort.
Examination
On physical examination, features concerning for possible thyroid cancer include a fixed hard thyroid mass or cervical lymphadenopathy, although these may be late findings. Additionally, an assessment for Pemberton’s sign (marked facial plethora with elevation of the arms) is warranted to check for retrosternal thyroid lesions not detected on neck examination causing thoracic outlet obstruction. Signs of hyperthyroidism (e.g. tachycardia, tremor or lid lag) or hypothyroidism (e.g. bradycardia or delayed relaxation of deep tendon reflexes) should also be sought.
Investigations
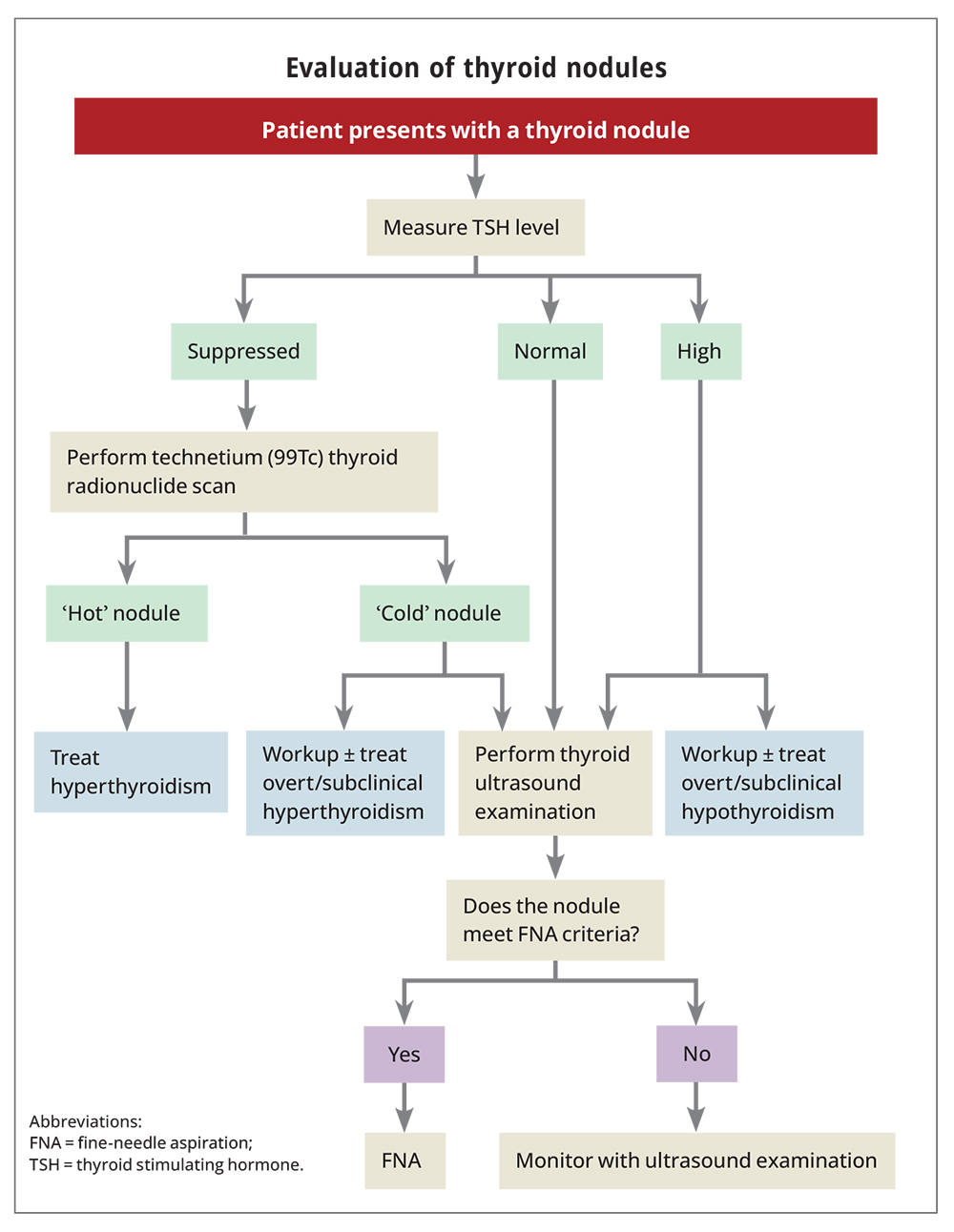
The initial investigations for the workup of patients with a thyroid nodule include measurement of TSH level and thyroid ultrasound examination. The diagnostic pathway is summarised in the Flowchart.
{kind=link}
In patients with a suppressed serum TSH level, the next test to undertake is a technetium (99Tc) thyroid radionuclide scan to investigate whether the corresponding nodule on ultrasound has increased uptake (‘hot’) or not (‘cold’). Hot nodules are nearly always benign and rarely require biopsy. Cold nodules should be correlated with their ultrasound features to determine the risk of malignancy and need for FNA. About 5% of cold nodules will be malignant.4
In patients with a suppressed serum TSH level, hyperthyroidism or subclinical hyperthyroidism should be investigated and treated on its own merits, if the aetiology is not evident on radionuclide scan. This may include testing for TSH-receptor antibodies to look for Graves’ disease and then treatment, if warranted, with antithyroid drugs, radioactive iodine or thyroid surgery. Referral to an endocrinologist should be considered for patients with symptomatic thyrotoxicosis, or for those with subclinical hyperthyroidism (TSH level below the reference range with normal thyroid hormone levels) and concomitant factors warranting treatment such as atrial fibrillation and osteoporosis.
In patients with a normal TSH level, thyroid ultrasound examination is performed to assess for ultrasound features suggestive of thyroid cancer. In patients with an elevated TSH level, in addition to performing thyroid ultrasound examination to assess for cancer risk, evaluation and treatment of hypothyroidism is warranted as appropriate. For patients with subclinical hypothyroidism who have a TSH level between 5.0 and 10.0 mIU/L, levothyroxine treatment may or may not be required depending on the degree of TSH level elevation, age, symptoms and pregnancy-related considerations.
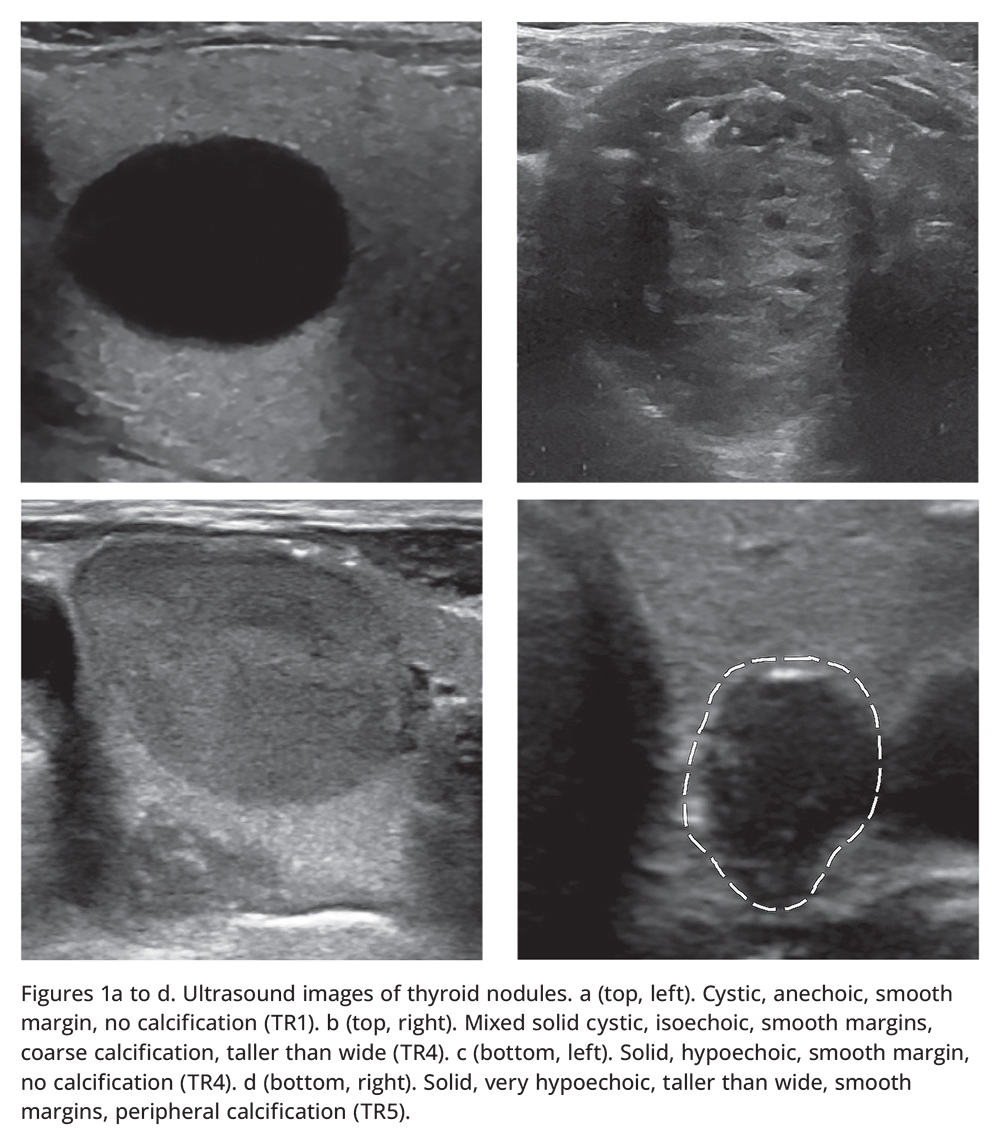
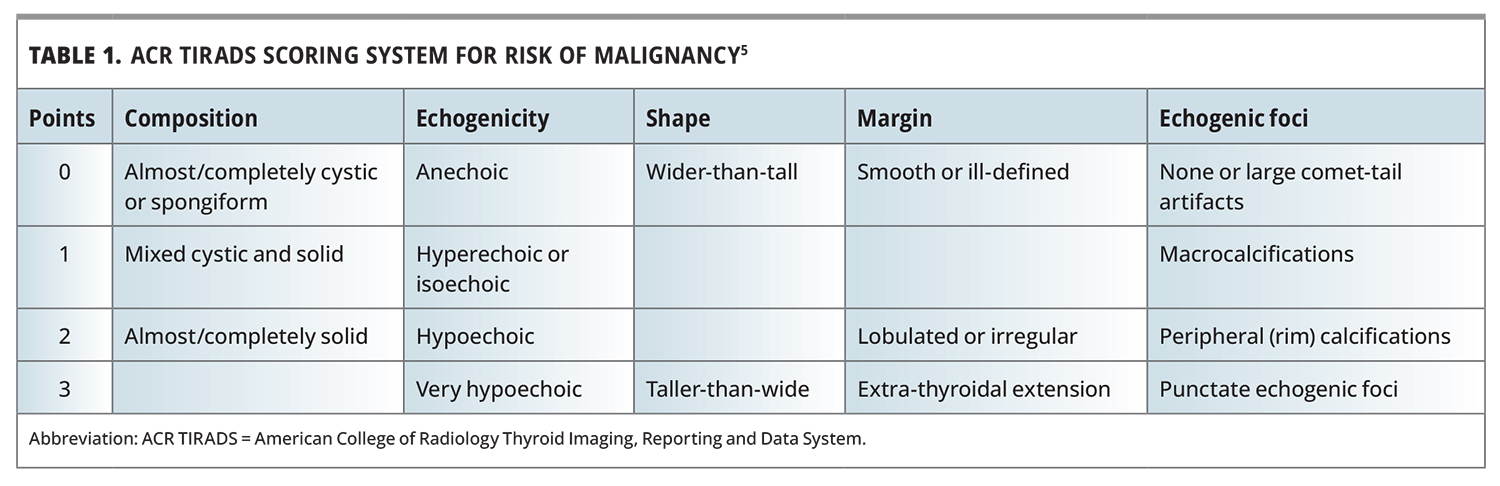
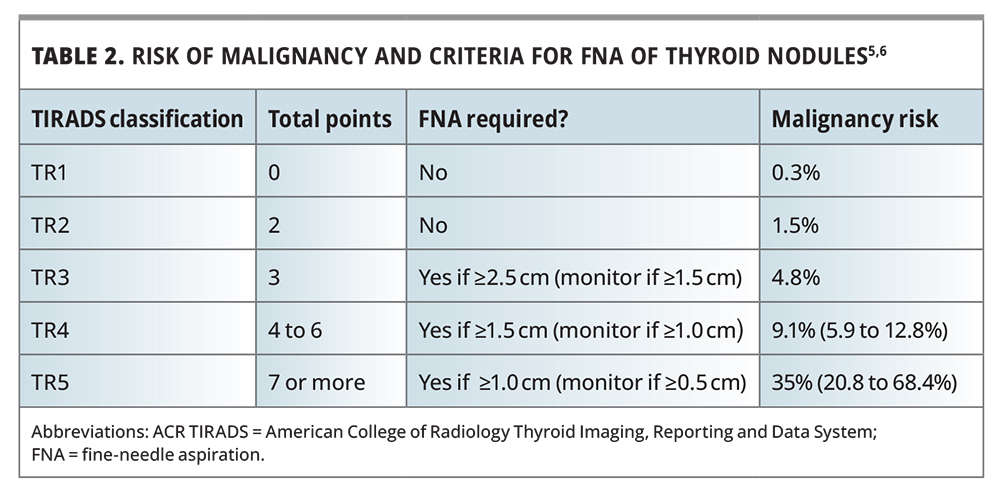
If a thyroid ultrasound examination is performed to assess for a nodule’s risk of cancer, a variety of ultrasound features are considered in determining a nodule’s risk of being malignant (Figures 1a to d). Several radiological reporting systems are established around the world to report on these features. The most commonly encountered reporting system in Australia is the American College of Radiology Thyroid Imaging, Reporting and Data System (ACR TIRADS).5,6 ACR TIRADS classifies the risk from the lowest TIRADS-1 (TR1) to the highest TIRADS-5 (TR5) based on five nodule features (composition, echogenicity, shape, margin and echogenic foci) that are each scored from 0 to 3 points (Table 1).5 The risk of malignancy as well as size thresholds to undergo FNA in each ACR TIRADS risk category are shown in Table 2.5,6 Nodules that meet or exceed the size threshold for biopsy should undergo ultrasound-guided FNA.
{kind=link}
{kind=link}
{kind=link}
Subsequent evaluation of thyroid nodules
Fine-needle aspiration
For thyroid nodules that undergo FNA based on their ultrasound risk of malignancy, their cytopathology result is reported according to the Bethesda system.7 The Bethesda system categorises thyroid FNA cytology results based on their risk of malignancy (Table 3). 7,8 The risk of malignancy ranges from low (Bethesda II) to high (Besthesda VI). It is worth noting, however, that a Bethesda I result is not a reassuring result and corresponds to a nondiagnostic specimen, for example because of an insufficient sample. Bethesda III and IV are often considered indeterminate results as cytology does not distinguish well between some hyperplastic nodules, follicular adenomas, follicular carcinoma and some cases of follicular variants of papillary thyroid cancer or noninvasive follicular thyroid neoplasm with papillary-like nuclear features.9 Benign cytology (Bethesda II) is seen in 70% of FNAs, indeterminate (Bethesda III or IV) in 10 to 15%, nondiagnostic (Bethesda I) in 15%, and malignant (Bethesda V or VI) in a small number of FNAs.8
{kind=link}
In the case of multiple thyroid nodules, evaluation of each nodule should proceed individually based on its own risk of malignancy (using the ultrasound features with FNA if meeting biopsy criteria). If multiple nodules meet FNA criteria, then the two nodules with the highest ACR TIRADS point totals should be biopsied, even if they are not the largest.5
It is worth noting that false-negative FNA results can be seen in 5 to 10% of cases, especially with larger nodules, inadequate samples and inexperienced cytopathologists.8
Ultrasound surveillance
For thyroid nodules that do not require FNA but are recommended to undergo monitoring, serial surveillance imaging should ideally be performed at the same radiology centre to allow for interval comparisons.10 The principle of radiological surveillance is that benign nodules generally do not increase in size.11 Thus, nodules that appear to be growing or that develop new suspicious features on serial ultrasound imaging have a greater chance of being malignant. Detection of these potentially malignant nodules allows for appropriate management.
Timing for ultrasound surveillance of nodules not initially meeting FNA criteria is not evidence-based, and varies according to the radiological reporting system. Based on the ACR TIRADS classification, it is suggested that TR5 nodules undergo annual ultrasound examination for five years, TR4 nodules should have repeat ultrasound at one, two, three and five years, and TR3 nodules should have repeat imaging at one, three and five years.5 Surveillance imaging can stop at five years if there has been no change in size. If, however, a nodule’s TR category increases on repeat imaging, then the next ultrasound examination should be performed in one year, assuming FNA criteria have not already been met.
Management of thyroid nodules after FNA
The management of thyroid nodules that have undergone FNA will depend on the FNA result (Table 3).7,8,12 For nodules with a nondiagnostic cytology result (Bethesda I), a repeat ultrasound-guided FNA is indicated, and if this is still nondiagnostic then subsequent management options include close observation, molecular testing (not readily available at present) or a diagnostic surgical resection. Diagnostic surgical resection, such as lobectomy, may be the preferred option if there is a high suspicion ultrasound pattern, if the patient has significant risk factors for thyroid cancer, if nodule growth has been detected on interval imaging (>20% increase in two dimensions with an increase of at least 2 mm; or >50% increase in nodule volume) or based on patient preference.12
For nodules with a benign cytology result (Bethesda II), if a high suspicion ultrasound pattern is present then repeat ultrasound and FNA is recommended within 12 months.12 If a low-to-intermediate suspicion ultrasound pattern is present then repeat ultrasound in 12 to 24 months is recommended. Repeat FNA should be considered if there is nodule growth (20% increase in a least two dimensions with minimal increase of 2 mm; or 50% increase in volume) or the development of new suspicious ultrasound features. If a very low suspicion ultrasound pattern is present, there is limited use for surveillance ultrasound. Additionally, if a Bethesda II nodule undergoes repeat FNA and returns a second benign cytology result, ultrasound surveillance is no longer needed.
For Bethesda III nodules, it is recommended that FNA be repeated in six to 12 weeks (with molecular testing depending on local availability), with a benign result meaning ultrasound surveillance can be undertaken, whereas a repeat indeterminate result may warrant consideration of diagnostic lobectomy.12 For Bethesda IV nodules, diagnostic lobectomy should be considered in consultation with the patient. For Bethesda V and VI nodules, lobectomy or thyroidectomy is recommended.
Management of nodules larger than 4 cm with a benign FNA result is controversial. However, depending on patient preference, these should be considered for excision because of a potentially higher risk of cancer and the potential for false-negative cytology results.8
Referral to an endocrinologist should be considered for patients who have a suppressed TSH level, suspicious ultrasound features or an indeterminate FNA result. Referral to a thyroid surgeon for either diagnostic or therapeutic surgery should be considered for patients with Bethesda IV, V or VI nodules, or for those who have compressive symptoms.
Conclusion
Evaluation of patients with thyroid nodules should include history taking and physical examination followed by measurement of TSH level and thyroid ultrasound examination. Reporting of Thyroid nodule appearance on ultrasound is standardised using the ACR TIRADS classification system. Ultrasound appearance of the nodule will guide the need for FNA, except for hot nodules in patients with a suppressed TSH level in which FNA is rarely required. FNA cytology results will guide the need for surveillance or surgical intervention. Patients in whom results are concerning for possible malignancy or those with indeterminate results should be referred to a specialist for evaluation and management. MT
COMPETING INTERESTS: None