Hashimoto’s thyroiditis. A case study of overt hypothyroidism

Thyroid diseases
Endocrine diseases
This case describes a 32-year-old man who presents with subtle symptoms and signs but has florid Hashimoto’s thyroiditis. The diagnosis and treatment of Hashimoto’s thyroiditis are straightforward; however, there can be some complexities in how levothyroxine therapy is used.
- Primary hypothyroidism is easy to diagnose if clinically suspected: an elevated thyroid stimulating hormone level on screening is followed by testing of free thyroxine levels, free triiodothyronine levels and antimicrosomal antibodies (at the outset only, to confirm the cause).
- Routine imaging of the thyroid is not required in the setting of hypothyroidism unless there is clinical nodularity or asymmetry of the thyroid gland on examination.
- Therapy with levothyroxine replacement is straightforward unless there are issues with absorption or compliance.
- Remission may eventually be achieved in younger patients.
Case scenario
A 32-year-old man presents to his GP with fatigue, which has been gradual in onset over the past six to 12 months. There has been no weight or appetite change, but he has mild constipation. His sleep patterns are unchanged.
He works in IT, is single and lives alone, following a break up one year prior. His past medical history is unremarkable, except for glandular fever at age 17 years. He is prone to mild anxiety but has not needed formal treatment for this. He has a healthy lifestyle; he exercises regularly and is a nonsmoker who drinks alcohol on weekends only (weekly intake of <60 g). There is a family history of hemithyroidectomy for benign thyroid nodular disease in his mother and his paternal grandfather had pernicious anaemia.
On examination, he is clinically euthyroid with normal blood pressure of 110/70 mmHg and a resting pulse of 60 beats per minute. Neck examination reveals a diffuse nontender goitre, just above normal thyroid size. Eye examination is normal apart from mild periorbital puffiness. There are no peripheral rashes. Cardiovascular, neurological and gastroenterological examinations are unremarkable.
Blood tests reveal a raised thyroid stimulating hormone (TSH) level of 105 mIU/L (reference range [RR] 0.4 to 4.0), free triiodothyronine (FT3) level within the reference range at 3.4 pmol/L (RR 2.6 to 6.0), a low free thyroxine (FT4) level of 8.9 pmol/L (RR 9 to 19) and an antithyroid peroxidase (anti-TPO) antibody titre of greater than 1300 mIU/L (RR <40). Full blood count, serum calcium and biochemistry are normal.
A diagnosis of autoimmune thyroid disease (AITD), specifically Hashimoto’s disease, is made.
What levothyroxine dose is needed initially?
This presentation is consistent with overt hypothyroidism secondary to Hashimoto’s thyroiditis. Thyroid hormone replacement with levothyroxine is indicated. A reasonable starting dose of levothyroxine is 1.6 mcg/kg body weight, with typical starting doses of 50 to 75 mcg daily, although a lower starting dose should be considered in older patients and those with a history of cardiac disease.1 The dose is related to lean body mass and this generally translates to 75% measured body weight.
When should TSH be remeasured and how should the levothyroxine dose be titrated?
TSH levels can take four to six weeks to fully respond to any adjustments in levothyroxine dosage. It is important to remember that if thyroid function tests are repeated earlier than this the values will not be at steady state.
Which thyroid autoantibodies should be tested in the context of an elevated TSH level? Please advise how to interpret their presence or absence.
Anti-TPO antibodies, also known as thyroid microsomal antibodies (TMAbs), and antithyroglobulin antibodies (TgAbs) are tested at the outset, noting that the former are more likely to be raised. Some authors have suggested that measurement of TgAbs is not needed in AITD (except in the context of monitoring serum thyroglobulin in patients who have had total thyroidectomy for thyroid cancer).2
Not all patients with AITD will have positive antithyroid antibodies.3 Serial monitoring of antithyroid antibodies is not recommended as the levels do not guide the effectiveness of therapy; this is done by monitoring the TSH level. In contrast, measurement of TSH-receptor antibodies can be performed every four to six months in the follow up of patients with Graves’ disease as it helps to guide management and predict remission.
What are the indications for arranging imaging in the setting of hypothyroidism and which imaging investigation(s) are appropriate?
Thyroid imaging is not routinely required when diagnosing hypothyroidism unless there is clinical asymmetry or suspected nodularity on clinical examination. The imaging of choice to evaluate this would be a thyroid ultrasound scan.4 This would not need to be followed by further imaging unless there was a clinical change or new indication, such as nodular disease.
Thyroid isotope functional scanning is not needed in Hashimoto’s disease and can cause confusion as it may show a diffuse increased pattern of isotope uptake (as seen in Graves’ disease). Thyroid isotope scanning is most useful in distinguishing Graves’ from thyroiditis (e.g. subacute or drug-induced), and from toxic nodules.
When would a pituitary or hypothalamic cause of hypothyroidism be suspected?
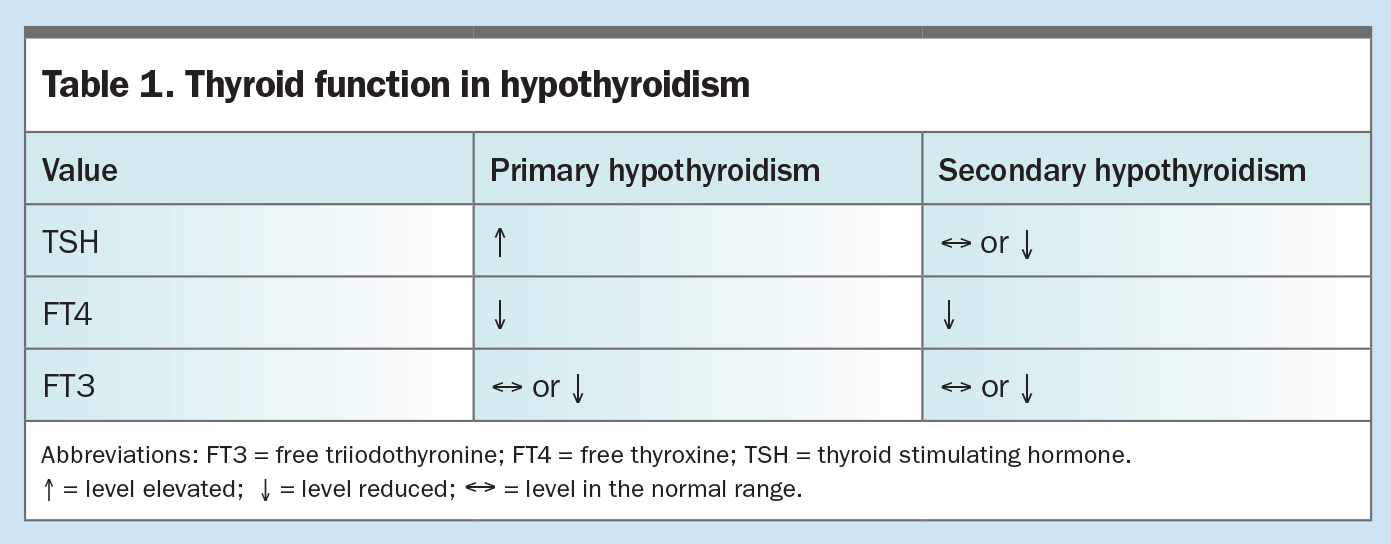
Secondary hypothyroidism is characterised by a TSH level in the low end of the normal range or below normal, and a FT4 level also low or low-normal (i.e. the TSH level is inappropriately low for the FT4 level). In some healthy individuals, a low-normal TSH level and low-normal FT4 level can be observed. Careful history needs to be evaluated and specialist input should be considered. In secondary hypothyroidism, FT3 levels tend to be low-normal and can be preserved in the normal range until the very late stages of both primary and secondary hypothyroidism (unless the patient is very sick or is taking amiodarone). Trends of thyroid function in different causes of hypothyroidism are outlined in Table 1.
{kind=link}
In hospitalised patients who are unwell, it is important to remember that thyroid function abnormalities can occur transiently as a sick euthyroid picture. This may resemble a pattern of secondary hypothyroidism. In sick euthyroid picture, the FT3 level is often low, with either normal or suppressed TSH and FT4 levels. Unless there is clinical suspicion of secondary hypothyroidism, in which case treatment should be considered, thyroid function should be repeated when the patient is well again.
What initial dose is appropriate for elderly patients or those with cardiac disease?
A starting dose of 25 to 50 mcg levothyroxine per day is recommended, depending on the age, body weight and degree of cardiac dysfunction. In most forms of cardiac disease, including arrhythmia, cardiac failure and ischaemic heart disease, gentle up-titration of levothyroxine should be considered, aiming to avoid over-replacement.5
Anecdotally, some patients (including young people) experience anxiety symptoms, including palpitations, when levothyroxine is first commenced; even before the TSH has corrected down to normal. It may be necessary to reduce the starting levothyroxine dose further and then titrate upwards more gradually. There are occasional rare cases where TSH normalisation causes intolerable anxiety, and in these cases, a higher TSH level target of above 10 m IU/L might be acceptable, as long as the FT4 level is normal.
When could weekly dosing of levothyroxine be considered?
Ideally levothyroxine should be taken daily but its half-life of one week means that occasional missed doses are not problematic. If compliance is difficult, then the total dose for one week may be taken as a single dose. This approach is sometimes adopted under supervision for patients with psychiatric illness.6
Should patients use the same type of levothyroxine (i.e. Eutroxsig vs Oroxine vs Eltroxin vs Levoxine) throughout their treatment in case of differences between the brands?
It is generally recommended that patients should continue with the same brand as anecdotally there can be minor differences in the bioavailability of different brands (e.g. a bigger dose of the newer non-refrigerated brand, Eltroxin, is sometimes needed).7 However, the literature suggests that overall the bioavailability differences between brands are minimal.
What is the appropriate initial treatment target?
The treatment is targeted to achieve a TSH level in the normal range, ideally with resolution of symptoms. Exceptions to this would be in the case of a high-risk thyroid cancer patient, where post-thyroidectomy TSH level targets are individualised according to the evidence-based guidelines. Pregnancy is another circumstance where TSH level targets will differ, especially in relation to trimester and presence of positive anti-TPO antibodies (although this is an area where there is lack of general consensus).2 Occasionally, patients have poor tolerance of levothyroxine symptomatically, for example those with intercurrent cardiac arrhythmias or significant anxiety, as mentioned earlier; in these cases, it may be acceptable to have a higher TSH level target (e.g. <10 mIU/L) as long as the FT4 level is in the normal range.
If the TSH level is still elevated after four to six weeks of levothyroxine treatment, what are the possible explanations and what is the suggested management?
It may take several months to reach target TSH levels in some patients, requiring ongoing titration of levothyroxine dosing. It is important to check adherence at each dose titration. Adherence should be checked by questioning the patient on when and how they take their tablets. It is advised that levothyroxine is usually taken in the morning on an empty stomach with no food or other medications for at least 30 minutes (or at bedtime, at least two hours after dinner). It is important to avoid calcium and iron tablets at the same time.8 Impaired absorption may also be a contributing factor in some cases where it is difficult to normalise the TSH level on standard doses of levothyroxine (e.g. levothyroxine absorption in the small bowel may be affected in patients with coeliac disease).
Sometimes the TSH level may normalise but the FT4 level is elevated; this might be explained by the patient having their blood drawn soon after taking their morning levothyroxine dose. Ideally thyroid function testing should be performed pre-dose or six hours after their levothyroxine dose.
A significant change in body weight, especially of lean body mass, may explain a sudden change in levothyroxine dose requirement. It is wise to avoid too high an incremental change in dose at each dose adjustment.
Once the TSH level is in the target range and symptoms have resolved, what is the recommended frequency of monitoring the thyroid function tests?
When stability is achieved, it is acceptable to monitor the TSH level annually (or sooner if symptoms develop in the interim).4 If frequent recent dose adjustments have been required then the TSH level will need more frequent monitoring. If a woman is considering pregnancy, thyroid function should be checked before conception and then at regular intervals (e.g. four to six weekly, throughout pregnancy). The woman should be advised that once a pregnancy test is positive, she should increase her levothyroxine dose by 30%, to reflect what happens in normal euthyroid women during pregnancy.9 This is required because thyroid binding globulin levels rise during pregnancy.
What are the indications for referral of patients to a specialist in the setting of hypothyroidism?
Patients who have instability in levothyroxine dosing and persistence of symptoms, such as fatigue, may benefit from specialist referral. Patients may also need reassurance that rising antithyroid antibody titres are not sinister and do not need serial measurement. Levothyroxine requirements can rise by 30% in the first trimester in pregnancy and specialist input should be considered at this crucial stage to maintain the TSH level in the normal range.4
In cases where patients are using or considering liothyronine (T3) replacement, either alone or in combination with T4 replacement, they should be referred for specialist input as this requires careful evaluation.7 There is also an emergence of thyroid extract being used by the general population. This is not endorsed by the Therapeutic Goods Administration or the Endocrine Society of Australia.7
When would you suspect poor adherence to treatment and can you provide some strategies for how to best manage this problem?
If there is significant instability in levothyroxine dosing without clear cause, adherence should be assessed. Persistently elevated TSH levels despite dosage adjustments, or significantly higher levothyroxine doses compared to a weight-based predicted dose requirement should trigger the clinician to question if there is poor adherence.10
Ways to increase adherence include asking patients to set a reminder for their medication, either as a physical reminder or on their phone. Most refrigerated forms of thyroid hormone replacement come in a metal strip, thus cutting out the weekly required dose and keeping this separate can help keep track of the dose. Nonrefrigerated forms of thyroid hormone replacement can be kept in a weekly pill organiser to help increase compliance. Given the long half-life of thyroid hormone replacement, it is possible to dose every second day or even once a week to help improve compliance.6
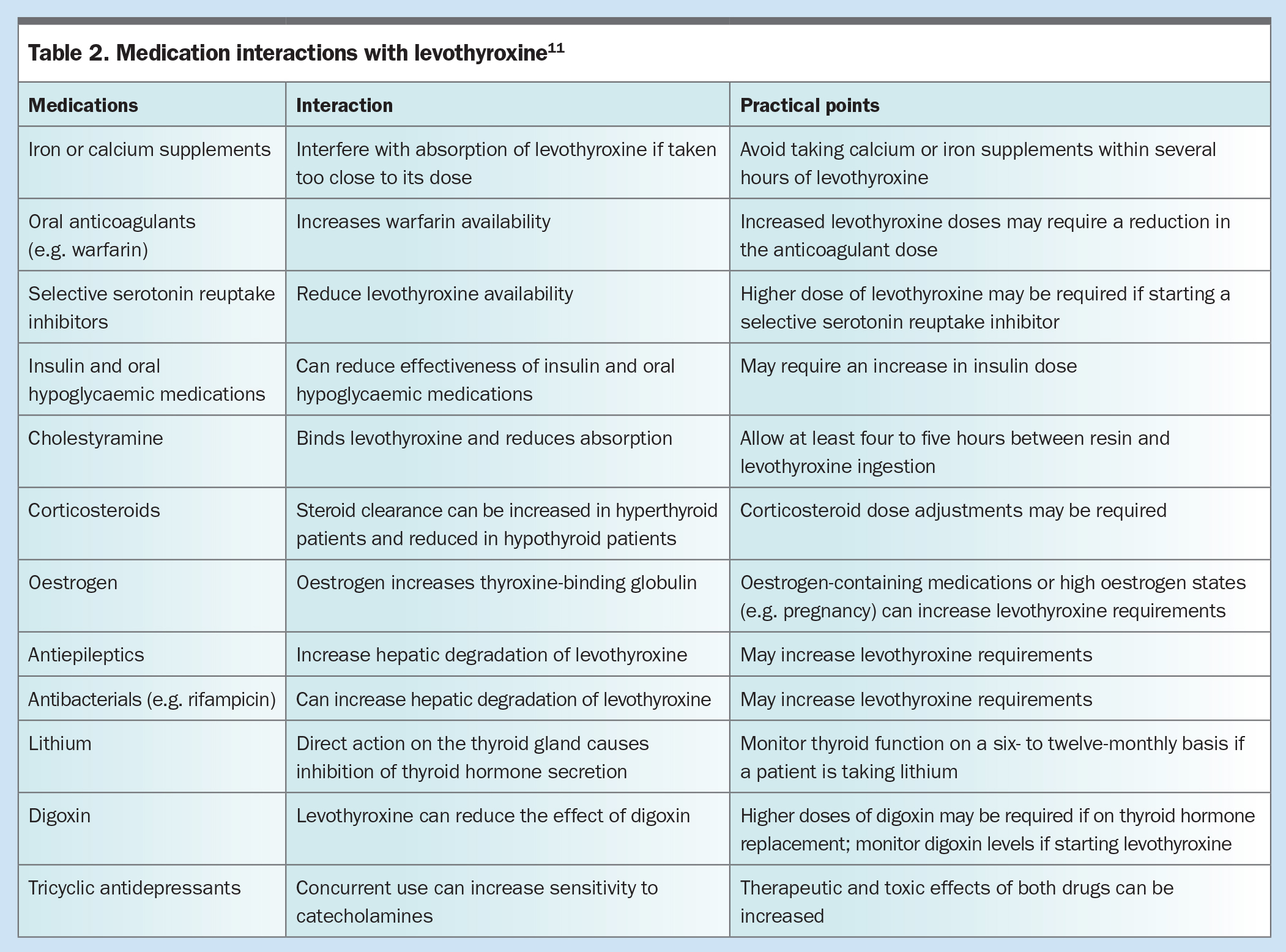
What are some potential drug interactions with levothyroxine and how might these affect the thyroid function test results? What should be the advice to patients taking these medications?
There are multiple medications that may interact with levothyroxine absorption, action or metabolism. Possible drug interactions with levothyroxine and some practical points are outlined in Table 2.
{kind=link}
Case continued
The patient achieves euthyroidism with levothyroxine replacement. His siblings are keen to be evaluated for hypothyroidism and both his brother and sister (aged 23 and 30 years respectively) are found to have normal TSH levels but mildly positive anti-TPO titres. With gradual dose weaning and monitoring of TSH levels, the patient is able to stop taking levothyroxine after three years. He has ongoing annual TSH level surveillance.
Summary
A 32-year-old man is diagnosed with florid Hashimoto’s thyroiditis after presenting with fatigue and a small diffuse goitre. His TSH and TMAb levels are very high but his FT3 level remains in the normal range, with a FT4 level just below the normal range. He becomes euthyroid with levothyroxine replacement and achieves remission over three years. TSH level surveillance allowed appropriate levothyroxine adjustment whilst on therapy and also appropriate monitoring to ensure the level remained in the normal range after levothyroxine weaning and cessation. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.