A clinical approach to subclinical hyperthyroidism
Thyroid diseases
Endocrine diseases
Subclinical hyperthyroidism can present with or without clinical symptoms of hyperthyroidism and is diagnosed biochemically. Treatment decisions are based on patient-specific factors, such as comorbidities and the presence of symptoms, and the degree of thyroid stimulating hormone suppression. Referral to an endocrinologist is recommended if there is uncertainty regarding diagnosis, or if specialist input is needed to guide further investigation and management.
- Subclinical hyperthyroidism is a biochemical diagnosis with low thyroid stimulating hormone (TSH) but normal serum thyroxine and triiodothyronine levels.
- There are differences in both aetiology and outcome for people with TSH levels between 0.1 and 0.4 mIU/L compared with those with a TSH level below 0.1 mIU/L.
- Other causes of low TSH (e.g. secondary hypothyroidism) should be considered.
- Treatment for subclinical hyperthyroidism depends on the aetiology, and follows the same general principles for treating overt hyperthyroidism from the same cause.
- Referral to an endocrinologist should be considered to guide further investigation and management as needed.
Subclinical hyperthyroidism is a biochemical diagnosis defined by thyroid stimulating hormone (TSH) levels below the reference range but serum thyroxine (T4) and triiodothyronine (T3) levels within the reference range, with or without clinical symptoms of hyperthyroidism.1 In contrast, overt hyperthyroidism, which is also a biochemical diagnosis, is characterised by serum T4 or T3 levels above the reference range as well as TSH levels below the reference range.1
The term subclinical hyperthyroidism is misleading, as ‘subclinical’ implies the absence of symptoms, which is not true for some patients. For instance, previous studies have shown that decreased TSH levels are associated with an increased risk of atrial fibrillation, even in the context of normal T4 and T3 levels.2 Some clinicians may be unsure of what to do when a patient has a mildly decreased TSH level (0.1 to 0.4 mIU/L) with normal T4 and T3 levels, especially if they are seemingly asymptomatic. This article aims to bridge the gap by outlining the epidemiology, diagnosis and current management recommendations for subclinical hyperthyroidism.
Epidemiology
Subclinical hyperthyroidism has an estimated prevalence between 0.7 and 6%, and varies with age, sex, ethnicity, the TSH assay used, iodine intake and local screening practices.3-6 Exogenous subclinical hyperthyroidism is common, with some form of subclinical hyperthyroidism or low TSH levels reported in 20 to 40% of patients taking thyroid hormone replacement.4,7,8 The National Health and Nutrition Examination Survey (NHANES III) estimated that, between 1988 and 1994, hyperthyroidism was present in 1.3% of the US population, of which 0.5% was overt and 0.7% was subclinical.3 This study also found that serum TSH concentrations were significantly lower among Black Americans than White and Mexican Americans.3 The prevalence of low serum TSH levels (below 0.4 mIU/L) increased between the ages of 20 and 39 years and again after 79 years of age.3 A study conducted in Tayside, Scotland found that 0.63% of the local population had subclinical hyperthyroidism (defined as having at least two measurements of TSH below the reference range for at least four months from baseline and normal free T4 or total T4 and total T3 levels at baseline).9 There are limited epidemiological data on the prevalence of subclinical hyperthyroidism in Australia. A cross-ectional study of 2033 participants (17 to 89 years of age, predominantly white, iodine-sufficient population with no history of thyroid disease) from Busselton, Western Australia, reported that subclinical hyperthyroidism was present in 1.7% of participants.10
Progression to overt hyperthyroidism
If left untreated, patients with subclinical hyperthyroidism can either remain stable, revert to euthyroidism spontaneously or progress to overt hyperthyroidism. The degree of TSH suppression is considered the best parameter for predicting the likelihood of progressing from subclinical to overt hyperthyroidism.11,12
The National Institute for Health and Care Excellence (NICE) Management of Subclinical Thyrotoxicosis Evidence Review reported differences in both aetiology and outcome for people with TSH levels between 0.1 and 0.4 mIU/L compared with those with a TSH level below 0.1 mIU/L.12 People with TSH levels 0.1 to 0.4 mIU/L tend to have a transiently low TSH level that is associated with nonthyroidal illness, medication use or older age.12 In contrast, those with subclinical hyperthyroidism and a completely suppressed TSH are more likely to have mild thyroid autonomy or be in the early stages of thyrotoxicosis. Longitudinal studies showed that Grade I subclinical hyperthyroidism (i.e. TSH levels between 0.1 and 0.39 mIU/L) may normalise in 25 to 50% of patients on repeated testing, whereas 5 to 8 % of individuals with untreated Grade II subclinical hyperthyroidism (i.e. TSH level below 0.1 mIU/L), may progress to overt disease each year.11
Differential diagnoses
Before diagnosing subclinical hyperthyroidism, other causes of low TSH level and normal T4 and T3 levels should be considered. Differential diagnoses include:
- central hypothyroidism due to pituitary or hypothalamic dysfunction (where TSH level is low and T4 and T3 levels are usually low or low-to-normal)
- nonthyroidal illness
- resolving hyperthyroidism after starting treatment (e.g. in a patient treated with antithyroid medications for Graves’ disease, the recovery of TSH levels can lag behind the normalisation of T4 and T3 levels)
- recovery phase of hyperthyroidism due to thyroiditis
- physiological lowering of TSH levels due to a shift in the distribution of ‘normal’ TSH values (e.g. trimester-specific reference ranges are used because of dynamic changes to the TSH during pregnancy13)
- use of medications or substances that could impact the TSH level (e.g. iodine, amiodarone)
- use of medications or substances that could cause interference with the TSH assay (e.g. biotin).
Toxic multinodular goitre is the most common endogenous cause of subclinical hyperthyroidism, particularly in older people.14,15 Graves’ disease is the second most common cause of subclinical hyperthyroidism, and is more prevalent in younger people and iodine-sufficient regions.1,15 Less common causes of subclinical hyperthyroidism include solitary autonomous functioning nodules and various forms of thyroiditis (Box).1,16
{kind=link}
Investigations
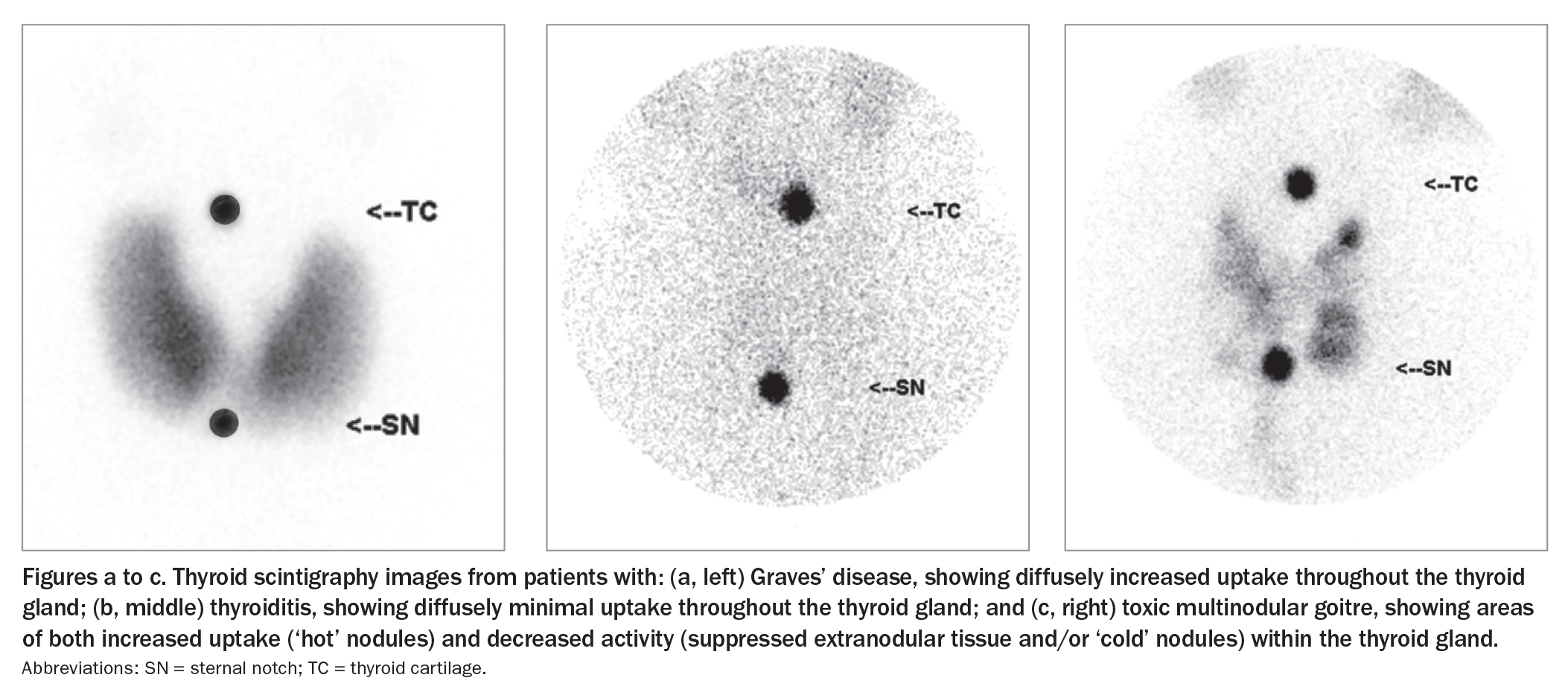
An algorithm for investigating subclinical hyperthyroidism is presented in the Flowchart.1,11,12 If the TSH level is below the reference range, check the free T4 and free T3 levels to differentiate between subclinical and overt hyperthyroidism. If a diagnosis is not apparent after careful assessment of the clinical presentation and initial biochemical evaluation, it is important to measure the TSH receptor antibody (TRAb). A positive TRAb result suggests Graves’ disease. If the TRAb result is negative, or a thyroid nodule or nodular goitre is present on physical examination, consider arranging a nuclear medicine thyroid uptake scan (thyroid scintigraphy; Figures a to c). Thyroid scintigraphy should not be performed in women who are pregnant or breastfeeding, and measurement of thyroidal blood flow on ultrasonography could be considered instead. If a ‘cold’ nodule is identified on thyroid scintigraphy or if a thyroid nodule is found on palpation, perform a thyroid ultrasound to further evaluate the thyroid nodule using the American College of Radiology Thyroid Imaging, Reporting and Data System (TIRADS) criteria.17
{kind=link}
Complications of subclinical hyperthyroidism
Subclinical hyperthyroidism is associated with an increased risk of atrial fibrillation, congestive heart failure and death from coronary heart disease, particularly in postmenopausal women, older men and those with a TSH level below 0.10 mIU/L.15,18-23 In people 60 years of age and older, a low serum TSH level was associated with a threefold higher risk of atrial fibrillation in the subsequent decade.18 The Rotterdam Study found that higher free T4 levels within the normal range were associated with a higher risk of atrial fibrillation in people with T4 levels in the highest quartile than in those with T4 levels in the lowest quartile.24 Higher free T4 levels within the reference range were seen in those younger than 65 years of age.24 Importantly, the absolute 10-year risk increased from 1 to 9% in participants younger than 65 years, whereas individuals 65 years of age and older had an increase in risk from 6 to 12%.24 Similarly, in euthyroid people with normal serum TSH levels, serum free T4 concentration was independently associated with risk of atrial fibrillation.25 However, no significant difference was seen in TSH concentration between individuals with and without atrial fibrillation.25 These results suggest that increasing levels of thyroid hormone may confer a continuum of atrial fibrillation risk, and that the risk of atrial fibrillation may be responsive to even very minor relative thyroid hormone excess.
An observational cohort study in people taking thyroxine replacement reported that suppressed TSH was associated with increased risks of cardiovascular disease, arrhythmias and bone fractures.26 Small uncontrolled studies have reported that restoration of a euthyroid state can lead to improved cardiac parameters.27,28 However, there is a lack of data from randomised controlled trials to conclusively show that treatment of subclinical hyperthyroidism prevents atrial fibrillation, heart failure or death from coronary heart disease. There are no conclusive data at present on whether subclinical hyperthyroidism is associated with an increased risk of stroke.15,29
Subclinical hyperthyroidism is associated with an increased risk of osteoporosis, especially when there is severe subclinical hyperthyroidism (i.e. the TSH level is below 0.1 mIU/L).15,30-35 Some evidence suggests that subclinical hyperthyroidism may be associated with an increased risk of hip fractures and vertebral fractures, particularly in postmenopausal women, older men, people with other risk factors for low bone density, those with TSH levels below 0.1 mIU/L, and if the subclinical hyperthyroidism is endogenous in aetiology.30-32,36 A small nonrandomised study in postmenopausal women with subclinical hyperthyroidism (due to a nodular goitre) found that spine bone mineral density decreased by about 2% (of baseline values) per year compared with a 1 to 2% decrease in euthyroid postmenopausal women.37 Radioiodine treatment (resulting in normalisation of serum TSH level) prevented this decrease in bone mineral density for at least two years.37 Another small prospective follow-up study reported that treatment with methimazole (the active form of the pro-drug carbimazole) in postmenopausal women with endogenous subclinical hyperthyroidism (due to multinodular goitre) prevented excessive loss of bone mass, at least in the distal forearm.38 There is no conclusive evidence at this stage to show whether treatment of subclinical hyperthyroidism translates into reduced fracture risk.
There are no conclusive data on the effects of mild subclinical hyperthyroidism on mood, cognitive function and mortality.20,33,39-41 A review of meta-analyses data found that severe subclinical hyperthyroidism was associated with cognitive dysfunction and dementia, but there was insufficient evidence to determine whether treatment of subclinical hyperthyroidism improved clinical outcomes.15 A meta-analysis found that absolute excess mortality after diagnosis of subclinical hyperthyroidism was likely age-dependent, with increased risk beyond the age of 60 years, and this age-dependent effect may explain the conflicting results from previous studies.19,42-44
How should subclinical hyperthyroidism be treated?
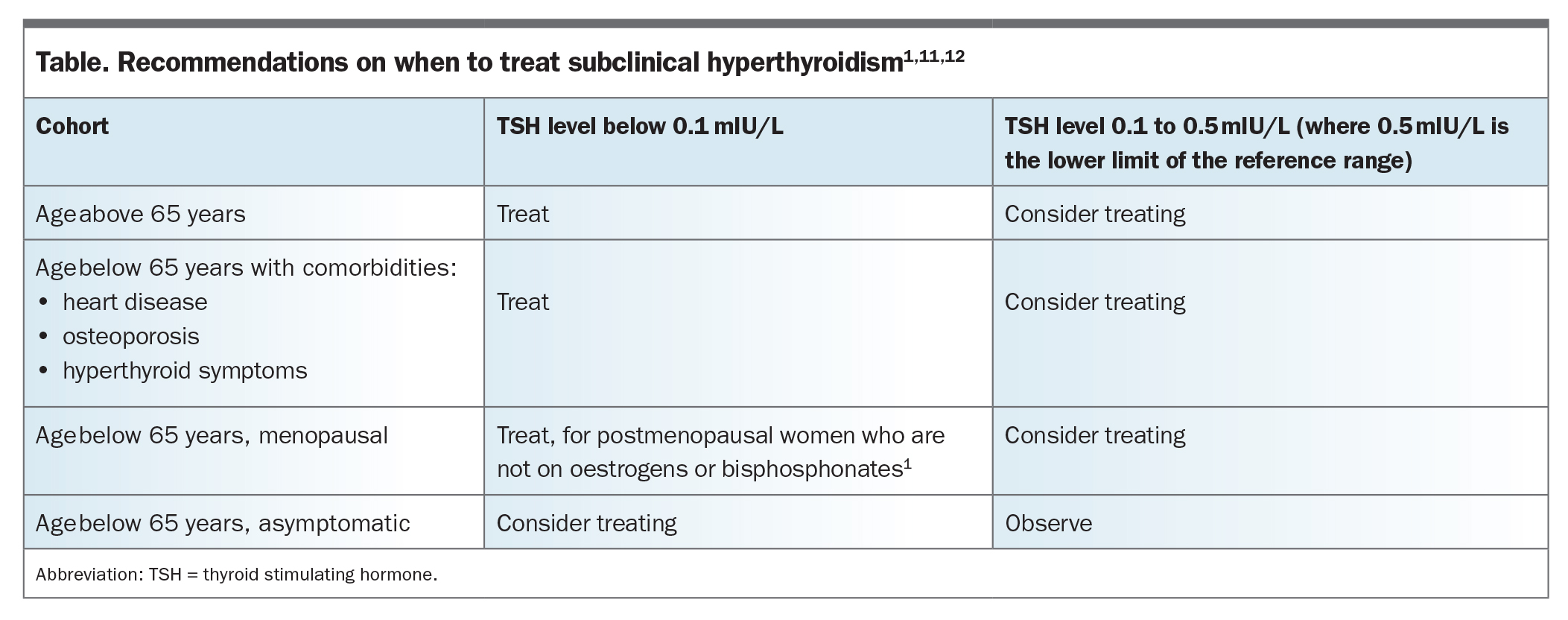
Early treatment of subclinical hyperthyroidism can prevent the development of known adverse effects of overt hyperthyroidism.15 Treatment of severe subclinical hyperthyroidism may also provide relief from symptoms, based on data from nonrandomised studies in young adults.15 However, there is a lack of conclusive data from prospective randomised controlled studies regarding whether the treatment of subclinical hyperthyroidism (especially in those with a mildly low TSH) leads to reduced risk of complications such as cardiac disease and osteoporosis. Therefore, treatment recommendations are mostly based on the well-established effects of overt hyperthyroidism on key endpoints.45 The Table summarises the treatment recommendations for subclinical hyperthyroidism based on the American Thyroid Association (ATA) guidelines, the ETA guidelines and the NICE evidence review.1,11,12 Treatment decisions are based on factors such as the patient’s age, comorbidities, the presence of symptoms and the degree of TSH suppression.
{kind=link}
If treatment is warranted, the specific treatment modality will depend on the aetiology of the thyroid dysfunction. The following are based on recommendations from the ATA guidelines.1
Radioactive iodine is appropriate for patients with toxic multinodular goitre or toxic thyroid adenoma, provided there is adequate suppression of background thyroid tissue on thyroid scintigraphy to minimise risk of damaging normal thyroid tissue. In people with subclinical hyperthyroidism and either compressive symptoms from a multinodular goitre or concern for malignancy, thyroidectomy should be considered.
For those with subclinical hyperthyroidism secondary to mild Graves’ disease, low-dose antithyroid medication is a reasonable choice (especially in younger patients), as remission rates are highest in this cohort. Some patients with subclinical hyperthyroidism due to mild Graves’ disease may experience spontaneous remission without treatment, so careful observation without therapy is also a reasonable option in this cohort.
To manage cardiovascular-related morbidity (especially atrial fibrillation) related to subclinical hyperthyroidism, treatment with beta-adrenergic blockade should be considered.
Referral to a specialist cardiology service should be considered for patients with symptoms of cardiovascular disease or new-onset atrial fibrillation, heart failure or coronary heart disease. In people with atrial fibrillation, complete an assessment of risk factors for stroke. In postmenopausal women, men over the age of 65 years and people with risk factors for low bone density, consider arranging a bone density scan.
Conclusion
Subclinical hyperthyroidism is a common condition often encountered in clinical practice. General practitioners should consider referring the patient to a thyroid specialist if there are diagnostic or management uncertainties. Treatment for subclinical hyperthyroidism depends on the aetiology and follows the same general principles for treating overt hyperthyroidism due to the same cause. ET
COMPETING INTERESTS: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.