Graves’ disease: the importance of TSH receptor antibodies

Thyroid diseases
Endocrine diseases
Graves’ disease is the most common cause of hyperthyroidism and remains challenging to diagnose and treat. Regular measurement of thyroid stimulating hormone receptor antibody (TRAb) levels is essential to monitor disease activity and treatment duration. Medical management is universal at the time of diagnosis and antithyroid drugs are needed initially to restore euthyroidism.
- Thyroid stimulating hormone receptor antibody (TRAb) levels should be measured in all patients with thyrotoxicosis. This is useful for diagnosis and in guiding management.
- Functional isotope thyroid scans may help clarify the cause of thyrotoxicosis.
- Carbimazole is first-line therapy for patients with Graves’ disease, except in early pregnancy.
- Beta blockers improve adrenergic symptoms and are helpful at the start of therapy.
- Close monitoring of the patient with Graves’ disease during pregnancy and the postpartum period is vital.
- Referral of the patient with Graves’ disease to an endocrinologist is advised, especially in women considering pregnancy and in patients who experience recurrence of the disease.
Graves’ disease is the most common cause of hyperthyroidism but remains a challenging scenario for GPs in terms of its diagnosis and therapy. In practice, Graves’ disease and Hashimoto’s thyroiditis can be regarded as different manifestations of the same disease, known for simplicity as autoimmune thyroid disease. They have contrasting test results and therapies but patients may convert from one to the other over time.
Epidemiology
As with many autoimmune diseases, Graves’ disease is more common in women than men (5–10:1), with onset occurring typically between 20 and 60 years of age.1 Several factors predispose to its development. Genetic susceptibility is well established in both forms of autoimmune thyroid disease and clustering in families is common. Graves’ disease is more common in some ethnicities, such as patients of South East Asian and Caucasian descents.1 The genetic basis of this disease remains to be fully elucidated; several studies have implicated human leukocyte antigen alleles on chromosome 6. Environmental risk factors for Graves’ disease include smoking, which worsens Graves’ orbitopathy. Both physical and psychological stress anecdotally can trigger Graves’ disease, although level 1 evidence for this phenomenon is lacking.
Diagnosis
Thyroid stimulating hormone (TSH) testing has the highest sensitivity and specificity for hyperthyroidism. Free thyroxine (FT4) and free triiodothyronine (FT3) should both be ordered concurrently if Graves’ disease is suspected clinically. If the index of suspicion is low then Medicare rebates are such that TSH testing is the appropriate single screening test to exclude thyroid disease. A suppressed TSH level with elevated FT3 and FT4 levels is diagnostic of hyperthyroidism.
Patients can present with a myriad of symptoms that can mimic other diseases. The most common presentations of hyperthyroidism include fatigue (occurs in both hyperthyroidism and hypothyroidism), weight change (usually but not always a decrease in weight), anxiety, heat intolerance, itchy skin, palpitations, increased bowel frequency (not necessarily diarrhoea), proximal muscle weakness and menstrual irregularity (Box).
{kind=link}
GPs remain understandably confused as to which thyroid antibodies should be measured. Thyroid peroxidase antibody (TPOAb) and thyroglobulin antibody (TgAb) – also called thyroid microsomal antibody (TMAb) – are noncausative and nonspecifically elevated in both types of autoimmune thyroid disease. They can fluctuate wildly in titre and should not guide management.
In contrast, TSH receptor antibodies (TRAb) are causative and specific to Graves’ disease. Stimulatory antibodies bind to TSH receptors usually resulting in overproduction of thyroid hormone. Measurement of TRAb is very helpful in guiding both diagnosis and management. Occasionally pathology collectors will incorrectly order a TSH measurement when ‘TSH receptor antibody’ is written so request forms should clearly denote the required tests. A new diagnosis of hyperthyroidism should be accompanied by measurement of TRAb levels even if Graves’ disease is not suspected clinically. This is important as many patients with Graves’ disease have neither a goitre nor the typical eye signs. Between 2 and 6% of patients with florid Graves’ disease will be TRAb negative. If the TRAb status is positive in a patient with thyrotoxicosis a diagnosis of Graves’ disease is confirmed. It is not useful to measure TRAb levels in patients who are euthyroid except when thyroid eye disease is present.
Management decisions are dictated by FT4 and FT3 levels (and less so by the TSH level). The TRAb level is helpful for understanding ongoing disease activity and TRAb status should be negative when drug treatment is ceased.
Differential diagnoses
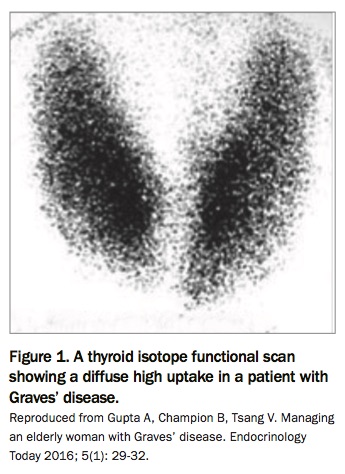
One of the most common referrals to endocrinologists is a newly diagnosed hyperthyroid patient in whom the cause is unclear to the GP. A thyroid isotope functional scan (using 99cTm Technetium) can be helpful to confirm the cause especially if TRAb status is equivocal or negative; however, it is usually not required if TRAb status is positive. This scan will show a diffuse high uptake in Graves’ disease (Figure 1) and low uptake of isotope in thyroiditis. A thyroid ultrasound has limited use in acute hyperthyroidism but may help to exclude nodular thyroid disease if there is clinical concern. Repeated ultrasounds are useful in follow up of patients with nodular thyroid disease but not in those with autoimmune thyroid disease.
{kind=link}
It is possible for patients to have more than one cause of hyperthyroidism operating simultaneously, especially older patients. Graves’ disease may occur in an existing nodular thyroid gland, and the isotope scan will then show diffuse and increased isotope uptake overall but with ‘cold’ areas interspersed. Some patients who are TRAb negative will have a clear ‘hot’ nodule whereby the isotope is concentrated in the nodule itself with complete suppression of uptake in the remaining gland. Careful clarification of the cause is important to select the appropriate therapy.
In tertiary hospital populations the frequency of drug-related thyroiditis caused by a variety of agents (including the iodine-loaded drug amiodarone and the immune-modifying anticancer drugs) has increased. These cases will be associated with low or absent uptake of isotope, in contrast to the diffusely elevated uptake of Graves’ disease. Graves’ disease can be caused by use of drugs (e.g. alemtuzamab used for multiple sclerosis) but it is rare. Isotope scans are not helpful in the assessment of Hashimoto’s thyroiditis, although interestingly they can be associated with either elevated or lowered isotope uptake.
Examining the ratio of T3:T4 can also be useful in the diagnosis of Graves’ disease if the TRAb level is low and/or isotope scanning is contraindicated. In patients with hyperthyroidism from overproduction of the hormone (Graves’ disease), the active hormone T3 is usually overproduced compared with T4; the same can occur in toxic nodular disease.
Management
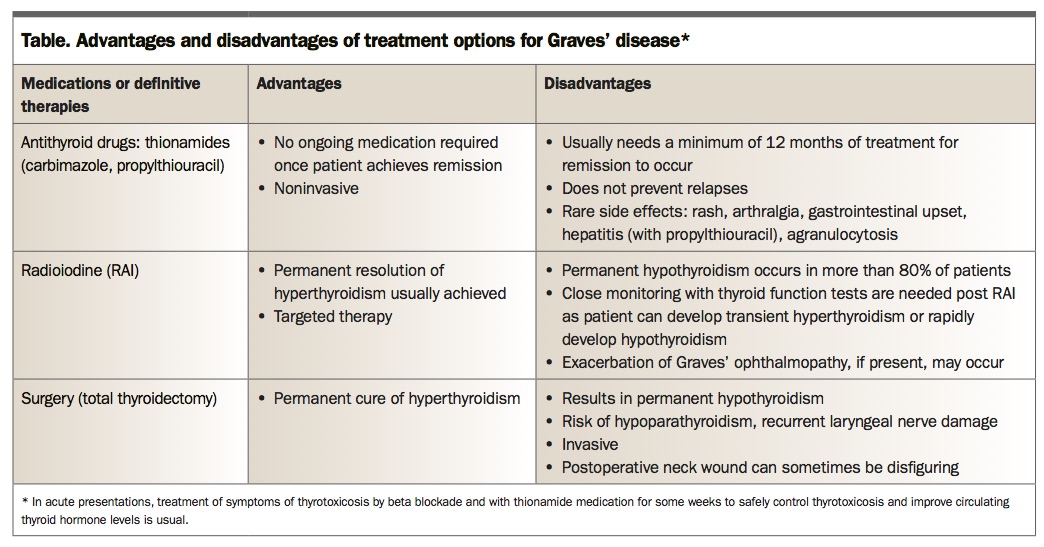
Medical management is universal at the time of diagnosis. Antithyroid drugs are needed initially to restore euthyroidism even if definitive therapy is planned. Carbimazole is the drug of first choice for patients with Graves’ disease. Propylthiouracil should only be used if the patient is allergic to carbimazole or in women during early pregnancy or if pregnancy is contemplated. Carbimazole is given in differing doses depending on the severity of the hyperthyroidism, which can vary from subclinical (low TSH level with normal T4 and T3 levels) to severe (e.g. thyroid hormone levels more than four times the upper limit of normal). The latter may require large doses divided into three or four times daily dosing. The American Thyroid Association guidelines suggest a rough guide for dosing of carbimazole: 5 to 10 mg/day if FT4 levels are 1 to 1.5 times the upper limit of normal; 10 to 20mg/day if FT4 levels are 1.5 to 2 times the upper limit of normal; and 30 to 40mg/day if T4 levels are 2 to 3 times the upper limit of normal.1 Resistant cases can respond to an increase in dose frequency even without an increase in total dose. Thyroid function tests should be carried out at least monthly in the first few months of starting drug treatment and the drug doses tapered rapidly in accordance with reducing FT4 and FT3 levels, noting that the TSH level will remain low for much longer and is not useful in guiding carbimazole dosing at this stage. Medical management at the lowest possible maintenance dose is continued for a minimum of 12 to 18months and until TRAb status becomes negative. Recurrence is lower if these principles are applied. The Table outlines the advantages and disadvantages to drug treatment, as well as surgery and radioiodine therapy, for patients with Graves’ disease.
{kind=link}
Carbimazole is generally effective and very well tolerated. Rarely, patients may be allergic to the drug but a skin rash from the disease itself is common so the timing of onset should be carefully noted so that drug allergy is not blamed inaccurately. Patients taking carbimazole or propylthiouracil must be warned about the rare but serious allergic/toxic event agranulocytosis. They should contact their physician urgently if they get mouth ulcers or sore throat/fever so that an urgent white cell count can be performed. Agranulocytosis is rare but more likely in the first three months of therapy, although it can also occur in subsequent courses of therapy, and with higher doses of drug. There is a 15 to 20% risk of cross-reactivity in terms of low white cell count with use of propylthiouracil. Abnormal liver function occasionally occurs in patients taking carbimazole or propylthiouracil (more common with use of propylthiouracil, which should be avoided in children due to the risk of hepatotoxicity). Complications of this nature would benefit from specialist input. There are complex issues in relation to drug choice in pregnancy (discussed below).
Beta blockade is recommended in all patients with adrenergic symptoms unless they have asthma. The nonselective beta blocker propranolol is often useful, starting at a dose of 10 to 20mg twice daily. Patients can be weaned off propranolol as soon as carbimazole takes effect. The extra-thyroidal manifestations of Graves’ disease (e.g. anxiety, tachycardia, skin itch, weight loss, increased bowel frequency and deranged liver function) will usually resolve as the thyrotoxicosis is corrected. However, eye disease can be persistent (discussed below).
Graves’ orbitopathy
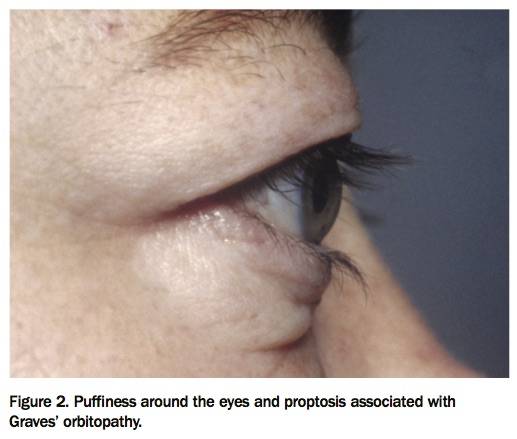
Progress in the management of thyroid eye disease has been disappointing and it remains a source of frustration for both clinicians and patients. Patients with Graves’ disease will usually have nonspecific eye symptoms such as puffiness around the eyes (Figure 2) and a sensation of soreness or grittiness. Patients may present with proptosis, and involvement of extra-ocular muscles. The latter can cause troublesome diplopia. Visual acuity itself is rarely affected (although can be in severe cases) but patients find the cosmetic aspects of thyroid eye disease very distressing and changes may be asymmetric.
{kind=link}
Nonmodifiable risk factors include advanced age, gender (more common in women, more severe in men), race (more common in Caucasians, less common in Asians), high TRAb level and a wider lateral wall orbital angle. Smoking increases progression and severity and needs to be urgently ceased.
Selenium 100 mg twice daily for six months can be helpful in modifying the disease. A course of oral (or intravenous) corticosteroids may be needed in some cases, but this should be managed by a specialist. Early referral of the patient to an ophthalmologist is useful to monitor pressures and assess the need for decompression surgery (or orbital radiotherapy) in refractory cases.
Remission and recurrence
After 12 to 18 months of medical therapy, it is reasonable to cease antithyroid drugs if TRAb status is negative and then monitor with thyroid function tests three monthly for the first year, then six monthly, then yearly. Patients who experience a recurrence of Graves’ disease should be recommenced on carbimazole while awaiting specialist follow up for assessment of definitive therapy.
Definitive options for the treatment of Graves’ disease consist of radioactive iodine ablation (RAI) or surgery. RAI (at doses determined by the endocrinologist) is given to ablate all residual thyroid tissue. Thyroidectomy (performed by a high-volume surgeon) is preferred if the patient has eye disease or a very large goitre. Following RAI or thyroidectomy, patients are required to be on thyroxine lifelong. They will need regular monitoring of thyroid function until their doses are stable, and then yearly monitoring at a minimum thereafter. Prolonged treatment with antithyroid drugs is sometimes used if the total dose is small and the patient elderly.
Graves’ disease and pregnancy
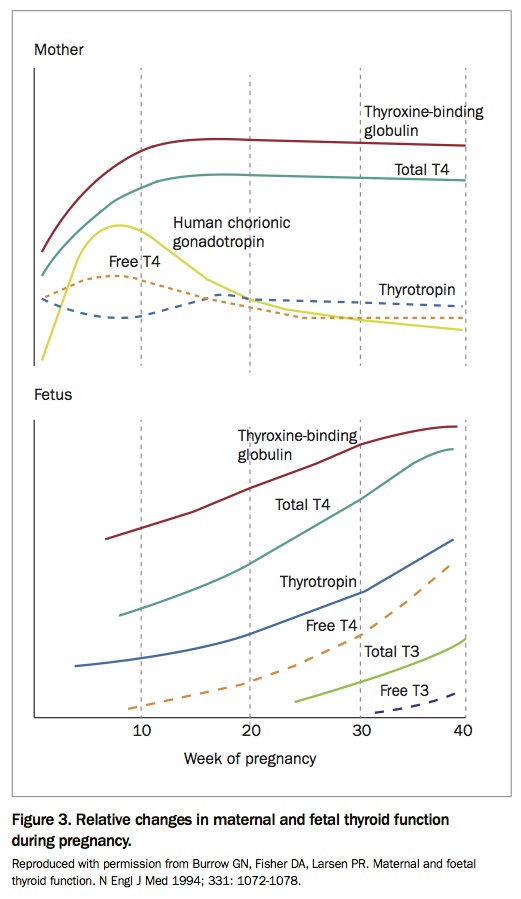
Pregnancy is a state of greater thyroid hormone demand, with fetal neurological development (in the first trimester) dependent on an adequate supply of maternal T4. Rising levels of human chorionic gonadotropin stimulate the thyroid, manifesting in up to a 20% enlargement in thyroid gland size, with a 30 to 50% increase in T3 and T4 production (Figure 3). Thus, TSH levels reduce in pregnancy and can fall below the lower limit of the nonpregnant reference range. Subclinical TRAb negative hyperthyroidism can reflect a normal pregnancy and does not warrant intervention.
{kind=link}
Overt hyperthyroidism (low TSH level with elevated T4 and/or T3 levels) is seen in less than 1% of pregnancies, with Graves’ disease and gestational transient thyrotoxicosis the leading causes. The latter is TRAb negative and drug treatment is not required. As the human chorionic gonadotropin levels plateau in the second trimester the gestational thyrotoxicosis resolves.
Graves’ disease in pregnancy has both maternal and fetal implications and these patients should be referred to an endocrinologist. Transplacental crossing of TRAbs (especially in the second trimester at levels >5 IU/L) can lead to fetal and neonatal hyperthyroidism. Graves’ disease is associated with increased risk of miscarriage and poor fetal growth. Both propylthiouracil and carbimazole have potential toxicities if used in week six to 10 of gestation. If treatment is required, propylthiouracil is preferred in the first trimester during fetal organogenesis as the risks of severe birth defects are lower. Patients are switched to carbimazole from the second trimester. Very rarely, thyroidectomy may be performed in the second trimester, following specialist review. RAI is contraindicated in pregnancy.
Graves’ disease tends to improve during pregnancy but can relapse postpartum as with other forms of autoimmune disease. Careful clinical and biochemical monitoring is thus required, by performing thyroid function tests at six and 12 weeks of gestation and at six and 12 months postpartum. Both carbimazole and propylthiouracil are excreted in breast milk, albeit in small amounts, but carbimazole can be used safely in lactation in low doses (≤20 mg per day). Women are advised to express milk before dosing. RAI is contraindicated during lactation as it is actively taken up into breast tissue.
Women with pre-existing Graves’ disease who are considering pregnancy should avoid conception until they are euthyroid with a low TRAb level and on either low or zero doses of antithyroid drugs. Women who have undergone RAI should typically refrain from conception for six months following treatment.
Summary
Graves’ disease is the most common cause of hyperthyroidism and can cause significant morbidity. Regular measurement of TRAb levels is essential to monitor disease activity and treatment duration. Referral of the patient to an endocrinologist is advised, especially in women considering pregnancy. ET
Reference
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.