Thyroid eye disease: preserving vision and function

Thyroid diseases
Vision impairment and blindness
Thyroid eye disease can cause severe chronic eye discomfort, vision loss and appearance changes that may lead to reclusive behaviour. Early identification and prompt management of thyroid eye disease may reduce symptoms, preserve sight and allow patients to continue or resume normal activities of daily living.
- Hallmarks of thyroid eye disease (TED) are eyelid retraction, proptosis and restriction of ocular movements; however, patients with TED may also present with symptoms of chronic eye irritation alone.
- Removal of the thyroid has little impact on the development of TED.
- It is important to note that uctuations of thyroid function can exacerbate the course of TED.
- Initial management of patients with TED comprises: – ensuring that the cornea is protected – ruling out optic neuropathy – correcting thyroid dysfunction – advising smokers to cease smoking with cessation programs.
- Referral to an ophthalmologist is reasonable for any patient suspected to have TED as this disease potentially causes vision loss.
Thyroid eye disease (TED) is the most common cause of both bilateral and unilateral proptosis in adults, with an incidence of 2.9 cases per 100,000 population per year for men and 16.0 cases per 100,000 population per year for women.1 Although middle-aged women are most likely to present with Graves’ disease, older men tend to develop more severe TED.2-5 Young patients with Graves’ disease are less likely to develop TED.6,7 Patients with TED may experience severe and chronic ocular discomfort, loss of visual function and changes in their appearance, which often result in socially reclusive behaviour. Early recognition and treatment of TED may restore vision and help patients return to their activities of daily living.
How do patients present?
Patients with TED often present with thyrotoxicosis secondary to Graves’ disease. The classic presentation of Graves’ disease is bilateral proptosis, lid retraction and diffuse goitre. However, patients with TED can also present without any associated signs of Graves’ disease. Most (85%) of patients with TED are hyperthyroid, but 10% of patients with TED are euthyroid and a small proportion have Hashimoto’s thyroiditis.8,9 Patients with TED who are euthyroid have a significantly increased risk of developing hyperthyroidism within 18 months.8 As a result, regular six-monthly thyroid function tests are prudent. Family history of thyroid disease is a major risk factor for TED, found in over 60% of reported cases.10
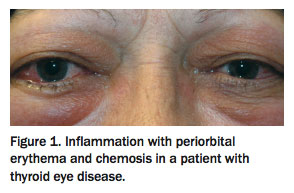
Patients presenting with proptosis and concurrent thyroid dysfunction are easily diagnosed with TED. However, patients who have normal thyroid function test (TFT) results and present with symptoms of chronic eye irritation are often treated for months for allergic conjunctivitis or dry eye syndrome before TED is diagnosed. Symptoms of chronic eye irritation in TED include red eye, chemosis, grittiness, epiphora, contact lens intolerance, orbital ache, periorbital or orbital swelling and erythema that is usually more severe in the morning than in the afternoon (Figure 1).
{kind=link}
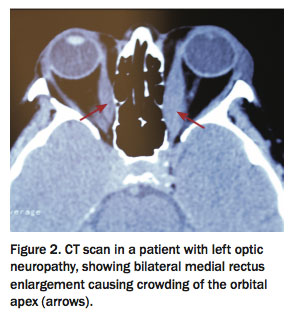
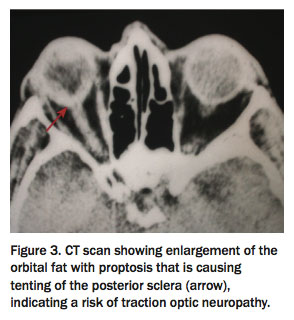
Blurred vision and a foreign body sensation from ocular surface disease are common complaints that may be due to impaired goblet cell and lacrimal gland function, reduced blink frequency, incomplete blink cycle, malposition of the eyelid from proptosis, epiphora due to reflex tearing from surface inflammation and exposure.11,12 Blurred vision from these causes clears transiently on blinking. If blurred vision does not improve with blinking then optic nerve compression from enlarged extraocular muscles and corneal ulceration or scarring from exposure should be considered, and patients should be referred for assessment of best corrected vision, the cornea and optic nerve. Patient reports of washed out or reduced colour perception are another worrying sign of optic neuropathy. This can be caused by enlargement of the extraocular muscles crowding the orbital apex, or by traction and tenting of the posterior sclera despite normal extraocular muscles (Figure 2 and Figure 3).
{kind=link}
{kind=link}
The hallmarks of TED are:1
- eyelid retraction (present in 90% of patients) with temporal flaring (Figure 4)
- proptosis (60%; Figures 5a to c)
- restriction of ocular movements (40%; Figures 6a to e).
{kind=link}
{kind=link}
{kind=link}
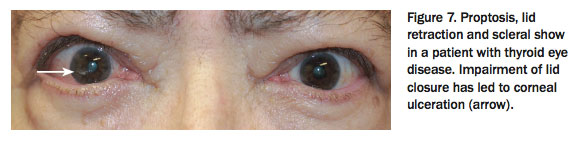
If lid closure is impaired then corneal ulceration may be present (Figure 7).
{kind=link}
Smoking increases the risk of TED seven to eightfold and also results in poorer treatment responses.13 Smoking is the single most important modifiable risk factor.14
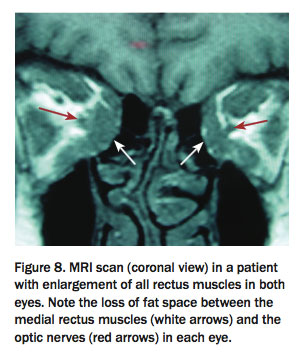
If patients present with the above hallmark features then a diagnosis of TED is highly likely. However, atypical presentations include unilateral disease, diplopia worsening towards the end of the day, divergence strabismus or the absence of lid retraction. These presentations warrant orbital imaging with CT or MRI, looking for rectus muscle enlargement (Figure 2 and Figure 8). The presence of thyroid antibodies increases the risk of TED but does not exclude other disorders such as allergic conjunctivitis, myasthenia gravis, orbital myositis, orbital tumours and carotid–cavernous fistula, which are potential differential diagnoses.
{kind=link}
Laboratory testing
Ophthalmologists treating patients with TED work closely with the GPs or endocrinologists managing the thyroid dysfunction. Although stable thyroid biochemistry does not in itself lead to resolution of TED, significant or recurrent swings in TFT results are likely to adversely affect the eye disease.
Autoantibody tests such as measurement of antithyroid peroxidase antibody (anti-TPO Ab) and thyrotropin receptor antibody (TRAb) levels can help clarify the clinical diagnosis, with anti-TPO Ab more commonly associated with Hashimoto’s thyroiditis and TRAb with Graves’ disease. Furthermore, the TRAb level can help determine, in conjunction with clinical assessment, whether TED is likely.15-18 Although there is not a linear correlation between TED activity and TRAb levels (as some patients in the active phase of TED have normal TRAb levels), in our experience TRAb level is loosely correlated with clinical activity in a significant group of patients and can give a hint as to when TED is entering the inactive phase. We strongly prefer to delay any orbital surgery until the TRAb level has normalised, as we have observed recrudescence of TED in patients with apparently inactive disease but raised TRAb levels who undergo orbital surgery. Anecdotally, many of our oculoplastic colleagues report the same. It is therefore helpful to the ophthalmologist if the treating physician and GP include measurement of TRAb level when monitoring thyroid dysfunction.
Pathogenesis of thyroid eye disease
A current hypothesis proposes that TED is an autoimmune disorder in which autoantigens are expressed on both orbital fibroblasts and thyroid epithelium.19-21 This leads to the production of pro-inflammatory cytokines and ultimately to infiltration of lymphocytes into the extraocular muscles and retro-ocular connective tissues. This causes interstitial oedema and inflammation of the extraocular muscles, resulting in the hallmark signs described above.
As a result of the dual expression of the autoantigens by orbital and thyroid tissue, removal of the thyroid has little impact on the development of TED. Also, there is no direct correlation between thyroid function (hypothyroidism, euthyroidism or hyperthyroidism) and TED. However, a stable background thyroid hormone status gives the best chance of shortening the active phase of TED.
In our experience, patients who have had remitting and recurring thyroiditis with multiple separate courses of carbimazole and neomercazole and those with fluctuating TFT results causing difficulty in stabilising drug dosages are more likely to develop TED or to have exacerbations of pre-existing TED. If patients are taking thyroxine (e.g. after radioactive iodine treatment or progression to Hashimoto’s disease) and the dose is difficult to titrate then erring on the side of overtreatment (i.e. aiming for a low thyroid-stimulating hormone [TSH] level) is preferable in the management of TED.
Natural history of thyroid eye disease
The course of TED comprises an active phase, which may last from six months to three years, followed by an inactive or chronic phase. The pathophysiology of TED is a multifaceted process that is not fully understood. The current theory states that during the active phase of TED, autoantibodies are activated to TSH receptors, which appears to be the inciting event as TSH receptors are overexpressed in retrobulbar tissues.22-24 Autoantibody activation leads to expansion of adipose tissue, resulting in congestion within the orbit and cicatricial changes.23-25
These cicatricial changes in the eyelid muscles cause retraction and lagophthalmos, while changes in the extraocular muscles cause diplopia. Cicatricial changes in the apex of the orbit and muscle enlargement can put direct pressure on the optic nerve and affect orbital venous outflow, resulting in venous congestion with further proptosis and vessel engorgement. Changes in appearance and function caused by enlargement of the extraocular muscles, retro-orbital fat and periorbital and orbital connective tissue and ongoing release of inflammatory mediators may continue for up to three years.
The thyroid-stimulating immunoglobulin level may show some correlation with TED activity during the active phase of the disease.26 However, there is no specific serological test to determine when a patient has reached the inactive or ‘burnt out’ phase of TED, and this is diagnosed from the history and clinical examination. The inactive phase is defined as no change in the physical signs on examination over a six-month period. Day-to-day fluctuations in symptoms are common, caused by changes in ambient temperature, humidity and stress levels, making diagnosis of the inactive phase challenging.
Importantly, in the inactive phase of TED, the fat hypertrophy and cicatricial changes that cause enlarged and restricted extraocular muscles, lid retraction and proptosis may persist. Patients with inactive TED can still have significant symptoms that severely reduce their quality of life and potentially cause vision loss. During the inactive phase, the swelling caused by inflammatory infiltrate and glycosaminoglycan-driven oedema settles, and the residual problem depends on the amount of scar tissue laid down during the active phase.
Because of the absence of inflammation in the inactive phase of TED, symptoms will not respond to any form of immunosuppression or deep x-ray therapy, and certainly in this phase of the disease the risks of these therapies outweigh the potential benefits. Although ongoing symptoms related to chronic lid retraction and proptosis in the inactive phase can be severe, these often fluctuating symptoms should not be treated with corticosteroids. In this phase, however, TED is stable, and reconstructive surgery is offered if the impact of TED is significant.
Management of thyroid eye disease
Initial management of patients with TED should:
- ensure that the cornea is protected
- rule out optic neuropathy
- correct thyroid dysfunction
- advise smokers to cease with cessation programs.
The cornea may be protected with lubricants, preferably without preservatives, comprising drops during the day and ointment at night if there are signs or symptoms of corneal exposure. Concomitant inflammation in the lacrimal gland can affect the quality and quantity of tears produced.27
Advice from specialist centres, with co-management of patients by an ophthalmologist and physician treating the thyroid disorder, should be sought early to optimise patient management.
When to refer
Initially, TED can be difficult to diagnose as many patients present with nonspecific ocular symptoms such as dry eye and ocular erythema and no symptoms of vision loss. A trial of use of nonpreserved lubricants is warranted in these patients. However, if symptoms persist for more than four to six weeks then referral to an ophthalmologist is indicated.
For any patient suspected to have TED, referral to an ophthalmologist is reasonable as this disease potentially causes vision loss. In the early stages of TED, it is impossible to identify which patients will have a severe course. Therefore, baseline testing of optic nerve function is warranted to allow treatment to be titrated should the patient’s condition deteriorate.
Active phase of TED
Management of patients during the active phase of TED depends on whether the disease threatens vision.
Vision-threatening TED
If TED is causing any loss of vision then treatments may include intravenous methylprednisolone, radiotherapy to orbital tissues and surgical decompression of the orbits. Loss of vision is diagnosed as a reduction in best-corrected vision, formal colour vision or visual fields.
If any vision loss is noted then intravenous methylprednisolone should be commenced at a dose of 500 mg weekly for six weeks, followed by 250 mg weekly for another six weeks.28 The patient’s vision parameters should be closely monitored. We use the response to corticosteroid therapy to indicate whether radiotherapy is likely to have a beneficial effect and aim to start radiotherapy immediately after vision improvement is noted.
Any vision improvement from methylprednisolone treatment will usually occur within one to two weeks. Studies have shown that patients receiving combined methylprednisolone and radiotherapy have significantly better outcomes than those receiving standalone radiotherapy.29,30 Methylprednisolone suppresses the immune response, whereas radiotherapy ablates inflammatory cells, preventing the ongoing inflammatory immune process.31,32 In effect, corticosteroids suppress inflammation only, but radiotherapy inactivates the inflammatory process.
The usual radiotherapy is given over a two-week period with a cumulative dose of 20 Gy per orbit, fractionated in 10 daily doses.33 Radiotherapy will take six to 12 weeks for a beneficial effect and may initially exacerbate the inflammatory response, but this will be dampened by the corticosteroid therapy. If radiotherapy is delayed and the patient has already completed the 12-week course of methylprednisolone before radiotherapy has its maximal effect then the optic neuropathy may relapse. This would necessitate surgical decompression of the orbits, which could have been avoided.
If there is no improvement in vision after two weeks of methylprednisolone treatment then urgent orbital decompression surgery should be considered.34 Surgical decompression addresses the mismatch between the enlarged volume of orbital soft tissue in patients with TED and the fixed bony volume of the orbit.
Patients who require surgical decompression to treat optic neuropathy in the acute phase of TED should receive adjuvant radiotherapy. If these patients are treated with decompression alone then up to 30% will have recurrent optic neuropathy as a result of ongoing inflammation, which causes continued enlargement of the orbital soft tissue volume.35 This can eventually fill the post-decompression bony orbital cavity.
Enlargement of orbital contents due to inflammation usually responds to corticosteroid and radiotherapy. A subgroup of patients, however, have optic neuropathy due to fibrosis at the orbital apex causing venous congestion rather than inflammation. These patients do not respond to corticosteroids and radiotherapy, and symptoms will improve only from surgical decompression of the orbital apex, thereby reducing venous congestion.
Nonvision-threatening TED
Patients with nonvision-threatening TED should be treated with supportive eye lubricants. Preservative-free lubricating eye drops are recommended. Patients who experience diplopia may benefit from either patching of one eye (alternating daily between each eye) or prisms mounted on spectacles, as this may allow them to return to activities of daily living.
Thyroid dysfunction
Treatment of systemic thyroid dysfunction aims to correct thyroid function and minimise recurrence and complications. The options are antithyroid medication, radioactive iodine treatment and thyroidectomy. All three options are effective, and the decision should be made by the patient after careful discussion.36
In our experience, thyroidectomy is likely to be the treatment of choice in patients with TED when there has been a relapsing–remitting course requiring multiple courses of antithyroid medication. Certainly, in patients with active TED receiving radioactive iodine treatment, corticosteroid cover is essential.33,37 There may be some long-term association between radioactive iodine treatment and exocrine gland disturbances, affecting the lacrimal, salivary glands and pancreas, leading to increased ‘dry eye’.38
Antithyroid medications such as carbimazole and propylthiouracil are the main treatment for blocking thyroid hormone synthesis and reducing autoimmune reactions. However, these medications do not alter the course of TED or provide any benefits to existing TED.28,39
Radioactive iodine can be administered to induce an inflammatory response and necrosis of thyroid follicular cells. This can be done during the active phase of TED if a prophylactic corticosteroid (0.2 mg/kg per day) is administered concurrently to reduce the risk of TED progression. The corticosteroid cover is tapered until withdrawal over six weeks.40 Patients who are in the inactive phase of TED can receive radioactive iodine without corticosteroid cover as long as they have no other risk factors for TED such as smoking or high TRAb levels.28,41,42
The aim of thyroidectomy is to correct thyroid function and minimise recurrences and the complication rate. Thyroidectomy should be considered if antithyroid medications have been trialled over one to two years and the patient continues to experience fluctuations of thyroid function. We believe these patients are more likely to develop TED. Thyroidectomy, similar to antithyroid medication, does not improve TED but provides better long-term control of thyroid function.28 It is important to note that fluctuations of thyroid function can exacerbate the course of TED.
If the patient is experiencing only mild TED of relative short duration then a watch and wait approach over six months with selenium supplementation may be recommended, as selenium can improve ocular symptoms and quality of life and prevent progression to more severe TED.28 It is important to discuss with patients the side effect profile of selenium and recommended daily intake as selenium toxicity is possible. It is reasonable to measure the baseline selenium level, and some practitioners institute selenium supplementation (in the form of sodium selenite 100 µm twice daily) only if the initial level is low.
Other medical treatments include intraorbital triamcinolone injections for active and recent-onset TED.43-45 Treatments that have not been shown to produce improvement or are awaiting further studies include azathioprine, the selective immune modulator ciamexone, immunosuppressants such as mycophenolate, biologics such as tocilizumab, monoclonal antibodies, tumour necrosis factor alpha and somatostatin analogues.46-52
Inactive phase of TED
In general, surgical reconstructive management is reserved for patients with TED in the inactive phase who are still experiencing significant symptoms. Reconstructive surgery may require three separate operations: orbital decompression, followed by strabismus surgery and finally lid surgery.
Orbital decompression surgery involves either bony or fat decompression or a combination of both.53-58 In bony decompression, portions of the medial wall, lateral wall and/or floor of the orbit are removed to enlarge its volume. The most common significant complication of orbital decompression surgery is onset of new diplopia. If diplopia does not resolve spontaneously within three to six months postoperatively then squint (strabismus) surgery is indicated to correct it. As squint surgery may affect the position of the eyelid (e.g. recession of the inferior rectus muscle can reduce upper lid retraction but increase lower lid retraction), lid retraction and blepharoplasty surgery may be required to reposition the eyelids and ensure the cornea is well protected.59,60
Conclusion
The early identification of ocular symptoms of TED and prompt management of the disease may reduce symptoms, preserve sight and allow patients to remain socially integrated. Although TED may progress over a few years, with appropriate management patients can return to normal activities of daily living.
References
- Bartley GB, Fatourechi V, Kadrmas EF, et al. The incidence of Graves’ ophthalmopathy in Olmsted County, Minnesota. Am J Ophthalmol 1995; 120: 511-517.
- Wall JR, Lahooti H. Pathogenesis of thyroid eye disease – does autoimmunity against the TSH receptor explain all cases? Endokrynol Pol 2010; 61: 222-227.
- Wiersinga WM, Smit T, van der Gaag R, Mourits M, Koornneef L. Clinical presentation of Graves’ ophthalmopathy. Ophthalmic Res 1989; 21: 73-82.
- Bartels EX, Irie M. Thyroid function in patients with progressive exophthalmos: study of 117 cases requiring orbital decompression. In: Pitt- Rivers R, ed. Advances in thyroid research. Transactions of the Fourth International Goiter Conference. London: Pergamon Press; 1961. p. 163-170.
- Horace K, Iv Y. Medical approach to ophthalmopathy of Graves’ disease. Mayo Clinic Proc 1972; 47: 980-985.
- Young LA. Dysthyroid ophthalmopathy in children. J Pediatr Ophthalmol Strabismus 1982; 16: 105-107.
- Metz HS, Woolf PD, Patton ML. Endocrine ophthalmopathy in adolescence. J Pediatr Ophthalmol Strabismus 1982; 19: 58-60.
- Burch HB, Wartofsky L. Graves’ ophthalmopathy: current concepts regarding pathogenesis and management. Endocr Rev 1993; 14: 747-793.
- Soeters MR, van Zeijl CJ, Boelen A, et al. Optimal management of Graves orbitopathy: a multidisciplinary approach. Neth J Med 2011; 69: 302-308.
- Bartley GB. The epidemiologic characteristics and clinical course of ophthalmopathy associated with autoimmune thyroid disease in Olmsted County, Minnesota. Trans Am Ophthalmol Soc 1994; 92: 477-588.
- Verity DH, Rose GE. Acute thyroid eye disease (TED): principles of medical and surgical management. Eye (Lond) 2013; 27: 308-319.
- Selter JH, Gire AI, Sikder S. The relationship between Graves’ ophthalmopathy and dry eye syndrome. Clin Ophthalmol 2014; 9: 57-62.
- Boboridis K, Perros P. General management plan. In: Wiersinga WM, Kahaly GJ, eds. Graves’ orbitopathy. A multidisciplinary approach. Basel: Karger; 2008. p. 88-95.
- Thornton J, Kelly SP, Harrison RA, et al. Cigarette smoking and thyroid eye disease: a systematic review. Eye (Lond) 2007; 21: 1135-1145.
- Lytton SD, Ponto KA, Kanitz M, Matheis N, Kohn LD, Kahaly GJ. A novel thyroid stimulating immunoglobulin bioassay is a functional indicator of activity and severity of Graves’ orbitopathy. J Clin Endocrinol Metab 2010; 95: 2123-2131.
- Ponto KA, Hommel G, Pitz S, Elflein H, Pfeiffer N, Kahaly GJ. Quality of life in a German Graves orbitopathy population. Am J Ophthalmol 2011; 152: 483-490, e481.
- Diana T, Brown RS, Bossowski A, et al. Clinical relevance of thyroid-stimulating autoantibodies in pediatric Graves’ disease – a multicenter study. J Clin Endocrinol Metab 2014; 99: 1648-1655.
- Kahaly GJ, Diana T, Glang J, Kanitz M, Pitz S, Konig J. Thyroid stimulating antibodies are highly prevalent in Hashimoto’s thyroiditis and associated orbitopathy. J Clin Endocrinol Metab 2016; 101: 1998-2004.
- Bahn RS. Graves ophthalmopathy. N Engl J Med 2010; 362: 726-738.
- Khoo TK, Bahn RS. Pathogenesis of Graves’ ophthalmopathy: the role of autoantibodies. Thyroid 2007; 17: 1013-1018.
- Orgiazzi J. Pathogenesis. In: Wiersinga WM, Kahaly GJ, eds. Graves’ orbitopathy. A multidisciplinary approach. Basel: Karger; 2008. p. 41-56.
- Douglas RS, Gupta S. The pathophysiology of thyroid eye disease: implications for immunotherapy. Curr Opin Ophthalmol 2011; 22: 385-390.
- Stan MN, Garrity JA, Bahn RS. The evaluation and treatment of Graves ophthalmopathy. Med Clin North Am 2012; 96: 311-328.
- Shannon J, Shan C, Douglas RS. The pathophysiology of thyroid eye disease. J Neuro-Ophthalmol 2014; 34: 177-185.
- Papageorgiou KI, Hwang CJ, Chang SH, et al. Thyroid-associated periorbitopathy: eyebrow fat and soft tissue expansion in patients with thyroid-associated orbitopathy. Arch Ophthalmol 2012; 130: 319-328.
- Dragan LR, Seiff SR, Lee DC. Longitudinal correlation of thyroid-stimulating immunoglobulin with clinical activity of disease in thyroid-associated orbitopathy. Ophthal Plast Reconstr Surg 2006; 22: 13-19.
- Bruscolini A, Abbouda A, Locuratolo N, Restivo L, Trimboli P, Romanelli F. Dry eye syndrome in non-exophthalmic Graves’ disease. Sem Ophthalmol 2015; 30: 372-376.
- Bartalena L, Baldeschi L, Boboridis K, et al; 2016 European Thyroid Association/European Group on Graves’ Orbitopathy. Guidelines for the management of Graves’ orbitopathy. Eur Thyroid J 2016; 5: 9-26.
- Shams PN, Ma R, Pickles T, Rootman J, Dolman PJ. Reduced risk of compressive optic neuropathy using orbital radiotherapy in patients with active thyroid eye disease. Am J Ophthalmol 2014; 157: 1299-1305.
- Shamsa PN, Mab R, Picklesb T, Rootmana J, Dolman PJ. Reduced risk of compressive optic neuropathy using orbital radiotherapy in patients with active thyroid eye disease. Am J Ophthalmol 2014; 157: 1299-1305.
- Donaldson SS, Bagshaw MA, Kriss JP. Supervoltage orbital radiotherapy for Graves’ ophthalmopathy. J Clin Endocrinol Metab 1973; 37: 276-285.
- Prummel MF, Mourits MP, Blank L, et al. Randomized double-blind trial of prednisone versus radiotherapy in Graves’ ophthalmopathy. Lancet 1993; 342: 949-954.
- Martalena L, Marcocci C, Manetti L, et al. Orbital radiotherapy for Graves’ ophthalmopathy. Thyroid 1998; 8: 439-441.
- Hart RH, Kendall-Taylor P, Crombie A, Perros P. Early response to intravenous glucocorticoids for severe thyroid-associated ophthalmopathy predicts treatment outcome. J Ocul Pharmacol Ther 2005; 21: 328-336.
- Spinasanta S. Graves’ orbitopathy and surgical decompression. 15th International Thyroid Congress, 85th Annual Meeting of the American Thyroid Association. Available online at: https://www.endocrineweb.com/professional/meetings/graves-orbitopathy-surgical-decompression (accessed June 2017).
- Bartalena L, Macchia PE, Marcocci C, Salvi M,Vermiglio F. Effects of treatment modalitiesfor Graves’ hyperthyroidism on Graves’ orbitopathy: a 2015 Italian Society of Endocrinology Consensus Statement. J Endocrinol Invest 2015; 38: 481-487.
- Bartalena L, Marcocci C, Tanda ML, et al. Orbital radiotherapy for Graves’ ophthalmopathy. Thyroid 2002; 12: 245-250.
- Solans R, Bosch JA, Galofré P, et al. Salivary and lacrimal gland dysfunction (sicca syndrome) after radioiodine therapy. Nucl Med 2001; 42: 738-743.
- Marcocci C, Bartalena L, Bogazzi F, Bruno-Bossio G, Pinchera A. Relationship between Graves’ ophthalmopathy and type of treatment of Graves’ hyperthyroidism. Thyroid 1992; 2: 171-178.
- Lai A, Sassi L, Compri A, et al. Lower dose prednisone prevents radioiodine-associated exacerbation of initially mild or absent Graves’ orbitopathy: a retrospective cohort study. J Clin Endocrinol Metab 2010; 95: 1333-1337.
- Eckstein AK, Plicht M, Lax H, et al. Thyrotropin receptor autoantibodies are independent risk factors for Graves’ ophthalmopathy and help to predict severity and outcome of the disease. J Clin Endocrinol Metab 2006; 91: 3464-3470.
- Perros P, Kendall-Taylor P, Neoh C, Frewin S, Dickinson J. A prospective study of the effects of radioiodine therapy for hyperthyroidism in patients with minimally active graves’ ophthalmopathy. J Clin Endocrinol Metab 2005; 90: 5321-5323.
- Alkawas AA, Hussein AM, Shahien EA. Orbital steroid injection versus oral steroid therapy in management of thyroid-related ophthalmopathy. Clin Experiment Ophthalmol 2010; 38: 692-697.
- Ebner R, Devoto MH, Weil D, et al. Treatment of thyroid associated ophthalmopathy with periocular injections of triamcinolone. Br J Ophthalmol 2004; 88: 1380-1386.
- Lee SJ, Rim TH, Jang SY, et al. Treatment of upper eyelid retraction related to thyroid-associated ophthalmopathy using subconjunctival triamcinolone injections. Graefes Arch Clin Exp Ophthalmol 2013; 251: 261-270.
- Perros P, Weightman DR, Crombie AL, Kendall-Taylor P. Azathioprine in the treatment of thyroid-associated ophthalmopathy. Acta Endocrinol (Copenh) 1990; 122: 8-12.
- Kahaly G, Lieb W, Muller-Forell W, et al. Ciamexone in endocrine orbitopathy. A randomized double-blind, placebo-controlled study. Acta Endocrinol (Copenh) 1990; 122: 13-21.
- Dickinson AJ, Vaidya B, Miller M, et al. Double-blind, placebo-controlled trial of octreotide long-acting repeatable (LAR) in thyroid-associated ophthalmopathy. J Clin Endocrinol Metab 2004; 89: 5910-5915.
- Wemeau JL, Caron P, Beckers A, et al. Octreotide (long-acting release formulation) treatment in patients with Graves’ orbitopathy: clinical results of a four-month, randomized, placebo-controlled, double-blind study. J Clin Endocrinol Metab 2005; 90: 841-848.
- Chang TC, Liao SL. Slow-release lanreotide in Graves’ ophthalmopathy: a double-blind randomized, placebo-controlled clinical trial. J Endocrinol Invest 2006; 29: 413-422.
- Stan MN, Garrity JA, Bradley EA, et al. Randomized, double-blind, placebo-controlled trial of long-actingrelease octreotide for treatment of Graves’ ophthalmopathy. J Clin Endocrinol Metab 2006; 91: 4817-4824.
- Perez-Moreiras JV, Alvarez-Lopez A, Gomez EC. Treatment of active corticosteroid-resistant Graves’ orbitopathy. Ophthal Plast Reconstr Surg 2014; 30: 162-167.
- Trokel S, Kazim M, Moore S. Orbital fat removal: decompression for Graves’ orbitopathy. Ophthalmology 1993; 100: 674-682.
- Goldberg RA, Perry JD, Hortaleza V, Tong JT. Strabismus after balanced medial plus lateral wall versus lateral wall only orbital decompression for dysthyroid orbitopathy. Ophthal Plast Reconstr Surg 2000; 16: 271-277.
- Kikkawa DO, Pornpanich K, Cruz RC Jr, Levi L, Granet DB. Graded orbital decompression based on severity of proptosis. Ophthalmology 2002; 109: 1219-1224.
- Unal M, Leri F, Konuk O, Hasanreisoglu B. Balanced orbital decompression combined with fat removal in Graves’ ophthalmopathy: do we really need to remove the third wall? Ophthal Plast Reconstr Surg 2003; 19: 112-118.
- Olivari N. Transpalpebral decompression of endocrine ophthalmopathy (Graves’ disease) by removal of intraorbital fat: experience with 147 operations over 5 years. Plast Reconstr Surg 1991; 87: 627-641.
- Leong SC, Karkos PD, Macewen CJ, White PS. A systematic review of outcomes following surgical decompression for dysthyroid orbitopathy. Laryngoscope 2009; 119: 1106-1115.
- Neoh C, Eckstein A. Eyelid surgery. In: Wiersinga WM, Kahaly GJ, eds. Graves’ orbitopathy. A multidisciplinary approach. Basel: Karger; 2008. p. 188-200.
- Baldeschi L. Rehabilitative surgery. In: Wiersinga WM, Kahaly GJ, eds. Graves’ orbitopathy. A multidisciplinary approach. Basel: Karger; 2008. p. 160-175.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.