TIRADS classification for thyroid nodules: application in practice

Thyroid cancer
Thyroid diseases
Thyroid nodules are increasingly diagnosed on ultrasound and, although most are benign, they still require appropriate assessment and follow up. The Thyroid Imaging, Reporting and Data System (TIRADS) offers structured assessment of thyroid nodules based on five sonographic features, while the Australian Modified Bethesda Criteria (AMBC) may assist with cytological assessment. Together, the TIRADS classification and the AMBC provide a validated framework for use in the approach to assessment and management of thyroid nodules.
- Although thyroid nodules are common and most are benign, widespread use of diagnostic imaging has led to high rates of nodule detection and an increased need for clinicians to provide appropriate management.
- The Thyroid Imaging, Reporting and Data System (TIRADS) classification was published in 2015 by the American College of Radiology to promote standardised terminology in the ultrasound reporting of nodules and to provide evidence-based recommendations for clinician action.
- The TIRADS classification assists in assessing the risk of cancer in thyroid nodules based on ultrasound characteristics. It is sensitive but not highly specific; although it is unlikely to miss a clinically significant malignant nodule, it is likely to result in biopsy and follow up of a high number of nodules that turn out to be benign.
- Using the TIRADS classification to select more suspicious nodules for fine needle biopsy refines risk assessment and selection for surgery. The Australian Modified Bethesda Criteria are useful in cytological assessment and management.
- Nodules selected for observation using ultrasound rather than biopsy should ideally be monitored at the same imaging practice to allow for comparison, preferably by the same clinician, to reduce interobserver variability.
- Application of the TIRADS classification does not subtract from the need for clinicians to explore patient concerns, preferences, comorbidities and prognosis when deciding on the management of a thyroid nodule.
Thyroid nodules are common and increase in prevalence with age. They can present to the GP as a neck lump that has been seen or felt by the patient or may be detected incidentally on clinical examination. However, they are more frequently seen on imaging, usually on an ultrasound scan performed for an unrelated reason. Such incidental findings may nevertheless be important and a validated framework for assessment can help guide further investigation.
Palpable nodules have a prevalence of 4 to 7% in iodine-replete adult populations, whereas ultrasonographically-detected nodules are reported at a prevalence of up to 68%.1,2 Most nodules are benign, and less than 5% of nodules detected on ultrasound are malignant. The increased detection of thyroid nodules relates mostly to the increased use of diagnostic imaging and facilitates timely diagnosis of thyroid cancer and early, potentially curative treatment. However, the accurate diagnosis of cancer needs to be balanced with the avoidance of overinvestigation and overtreatment. Considerations with regards to overtreatment include:
- repeated imaging and other diagnostic procedures
- unnecessary invasive treatment
- risks of complications from invasive procedures
- increased costs to the patient and healthcare system
- potential toll on the mental health of patients and their family.
The decision to subject patients with a thyroid nodule to biopsy may lead to unnecessary thyroid surgery for nodules that are ultimately benign.
This article reviews the current approach to assessing thyroid nodules using the Thyroid Imaging, Reporting and Data System (TIRADS) and its role in clinical practice.3
Presentation and initial assessment of thyroid nodules
Causes of thyroid nodules can be benign or malignant. Benign causes include colloid nodules, subacute thyroiditis, Hashimoto’s thyroiditis, a simple cyst and follicular adenoma; malignant causes include primary thyroid cancer (papillary, follicular, anaplastic, medullary), lymphoma and metastases. Surgical series report malignancy rates of 7 to 15% in referred populations but the rate of malignancy in primary care is under 5%. Malignant thyroid nodules are often asymptomatic and may be detected incidentally on ultrasound, CT, MRI or fluorodeoxyglucose-positron emission tomography. If a thyroid nodule is symptomatic, a patient may feel a lump in the neck, pain or discomfort when swallowing, shortness of breath or a change in voice, depending on the size of the nodule. In the presence of such symptoms, a detailed clinical neck examination should follow, including evaluation for lymphadenopathy. Classical findings suggesting malignancy such as a hard, fixed lump are rare. The absence of a lump does not exclude malignancy.
Measuring serum thyroid-stimulating hormone (TSH) levels may be informative, and a low, especially suppressed serum TSH level (<0.1 mU/L) in the presence of a nodule should prompt consideration of a thyroid radionuclide scan. A hyperfunctioning (‘hot’) nodule is highly unlikely to represent a malignancy.4 However, routine use of radionuclide scans is no longer appropriate because of poor diagnostic utility for the most common types of nodules: low- or nonfunctioning (‘cool’ or ‘cold’) nodules.
What is TIRADS?
Neck ultrasonography with a structured reporting process is now the standard process for evaluating thyroid nodules. Multiple systems are in use internationally, and all use similar criteria for nodule assessment. One of the most widely used and validated systems is the American College of Radiology TIRADS, which has been adopted by ultrasonographers in Australia.3 Proposed in 2015, this classification system is based on numerical scores that are assigned to five ultrasound characteristics and used to estimate the risk of cancer in thyroid nodules and suggest a management strategy.
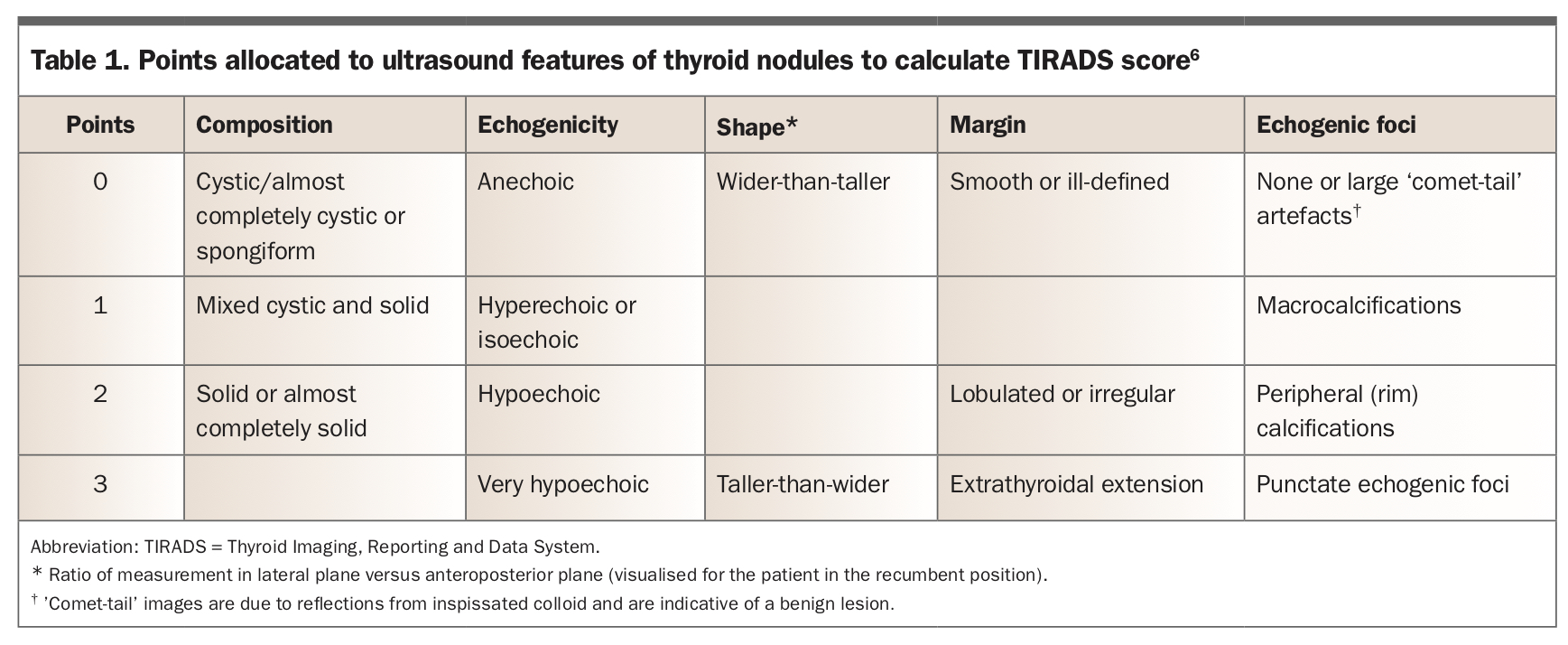
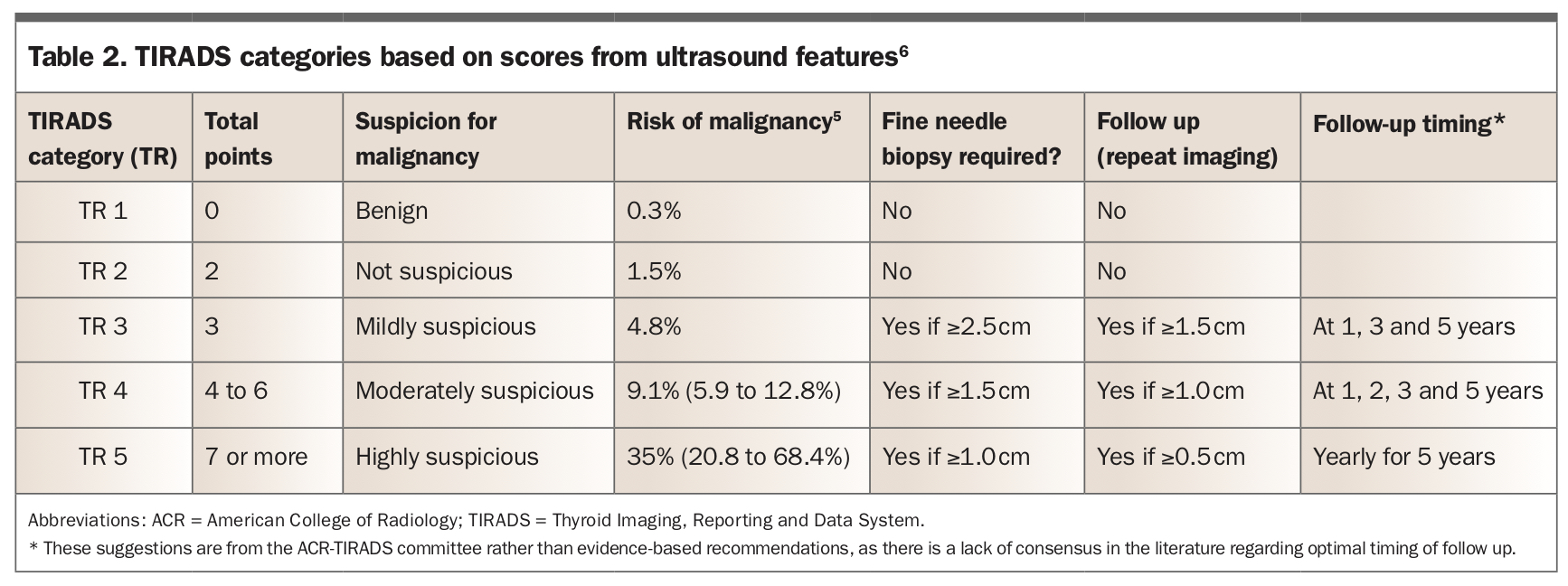
Ultrasonographic features of interest (composition, echogenicity, shape, margins and echogenic foci) are assigned a score that forms the basis of the TIRADS point score, as outlined in Table 1. The summation of these scores gives a TIRADS category (TR) for malignancy risk.5 TIRADS categories, suspicion for malignancy, requirement for fine needle biopsy (FNB) and follow up are summarised in Table 2.6 Where multiple nodules are seen, the four highest scoring nodules are followed up. The published risk of cytological malignancy increases with each score.5 FNB for cytological diagnosis is advised for TR 3 to TR 5 lesions when these meet size criteria (Table 2). In a large study of 3422 thyroid nodules, TIRADS assessment resulted in 65% of benign nodules being either biopsied or followed up (47% of benign nodules biopsied).7 This reinforces that the classification is not highly specific.
{kind=link}
{kind=link}
Interobserver variation in the assessment and reporting of ultrasound imaging is well acknowledged, but using a classification system such as TIRADS has been shown to enhance interobserver concordance in the decision to proceed to FNB.8 The value of TIRADS therefore lies in standardisation of reporting and identification of nodules that need further attention.
Application of TIRADS
The American College of Radiology TIRADS classification is a points-based system that performs well and is the most commonly used classification system in Australia.7 However, many other systems are used internationally, such as Korean TIRADS, European TIRADS, American Thyroid Association grading, American Association of Clinical Endocrinologists grading and British Thyroid Association classification. Although beyond the scope of this article, a detailed comparison of the strengths, weaknesses and pitfalls of the various systems has been recently published.9
The clinician’s interpretation of any TIRADS score must take into consideration its low threshold for prompting concern of malignancy and factor in the patient context. An apparent escalation of TIRADS scores over serial ultrasounds can be a cause for concern, and interobserver variation in ultrasound assessment and interpretation can contribute to this variability. Reports produced by two separate radiologists (with images taken by two different sonographers) and directly compared on the basis of the TIRADS score alone can result in more pronounced variability. Therefore, it is worth requesting a direct comparison of ultrasound images from the same clinician to better assess the presence and degree of progression. Requesting a comparison at the outset and organising repeat imaging with the same imaging provider so that previous images can be accessed may minimise the issue of interobserver variation. Systems incorporating machine learning have been shown to assist in risk stratification, and may be used more often in the future to assess thyroid nodules.10
Acting on the TIRADS category
The TIRADS score offers guidance for the clinician to provide the patient with a management plan (Table 2). The options are to offer reassurance and advise on further intervention, proceed to FNB or plan for a follow-up ultrasound scan. No further intervention is advised for a TR 1 or TR 2 nodule or a subcentimetre nodule detected in the absence of previously confirmed malignancy. Nodules that prompt suspicion but do not meet the size criteria for FNB may be followed up with repeat imaging. Serial imaging intervals of less than one year are considered excessive, with the exception of active malignancies being planned for intervention.11
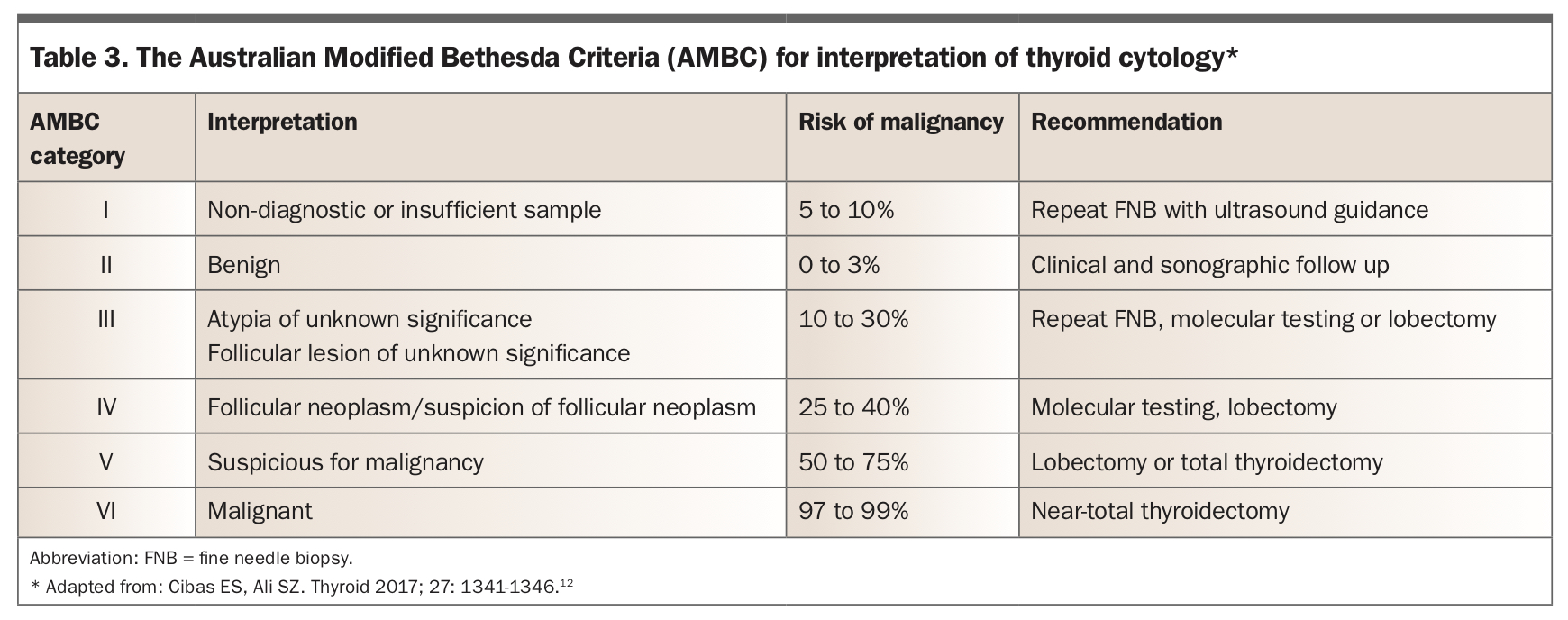
FNB provides nodule material for cytopathological examination to help determine whether a nodule is benign, malignant or in need of further assessment to reach a definitive diagnosis. The risks associated with FNB are very low but include bleeding, infection and damage to surrounding structures. The main problem is a non-diagnostic outcome. The Bethesda System for Reporting Thyroid Cytopathology is the grading system that serves to standardise terminology used in thyroid cytopathology reporting. In Australia, the system used is the Australian Modified Bethesda Criteria (AMBC). This system comprises six cytopathological categories that are linked to a risk of malignancy, a set of recommendations and a clinical management strategy, as outlined in Table 3.12
{kind=link}
A stronger evidence-base is needed to determine the duration and frequency of surveillance to detect erroneous classification after a nodule has been rated as benign using the ultrasonographic TIRADS categorisation or on cytopathological assessment. The follow-up timing recommended by the ACR-TIRADS committee, as shown in Table 2, offers a guide but may be unnecessarily frequent.6 The expert recommendation for follow up of cytologically benign lesions after one to two years is challenged by data showing that it is safe to extend the follow-up interval to three years without any adverse effect on morbidity or mortality.13 The nuances of follow up have recently been well-reviewed.14 As an example, a nodule classified as high risk (TR 5) with benign cytology should have repeat cytological examination within 12 months, whereas low-intermediate risk nodules (TR 3 and TR 4) that are stable on repeat ultrasonography should have a lengthened re-evaluation period and cessation of follow-up at five years, while growth or an unfavourable change in ultrasonographic characteristics should prompt repeat FNB.
Understanding the potential next steps after FNB is useful for the clinician and patient. The information provided by the TIRADS score should not dictate management but instead serve as a tool, in the discussion with the patient, to provide education and allow autonomy in agreeing on the next steps. Patient-specific factors, including patient wishes, risk factors for malignancy, comorbidities, use of anticoagulants, suitability for surgery and overall prognosis, must be considered. For instance, in some situations, the TIRADS score may recommend FNB, but considering the aforementioned factors, it may be more appropriate to repeat ultrasound imaging within a period of time before committing to the decision. Any uncertainty in these situations may be resolved by a referral to an endocrinologist to aid clinical decision-making. Challenging cases of thyroid nodules may also benefit from review in a multidisciplinary meeting, which referral to a specialist service may facilitate.
Conclusion
The TIRADS classification provides a guide for interpreting the malignancy risk of thyroid nodules based on ultrasound appearance. It is a useful evidence-based tool that general practitioners and other clinicians can use to guide a discussion with the patient and determine the approach to further assessment. It should be used in combination with clinical judgment and patient involvement in decision-making, bearing in mind that it is lacking in specificity and promotes follow up of benign nodules. Application of TIRADS is, however, far preferable to decision-making without an evidence base. In the future, routine use of machine-based learning systems that incorporate the results of imaging and cytology into reporting processes will likely enhance management of thyroid nodules. ET
COMPETING INTERESTS: None.