Osteoporosis: enhancing management in primary care

Dr Bennett is a Staff Specialist in the Department of Endocrinology at Sutherland Hospital; Visiting Medical Practitioner in the Department of Endocrinology at St Vincent’s Hospital; and Conjoint Associate Lecturer and PhD Student at UNSW Sydney, Sydney. Professor White is a Senior Staff Specialist in the Department of Endocrinology at Prince of Wales Hospital Randwick; Director of Research at South Eastern Sydney Local Health District; and Conjoint Associate Professor at UNSW Sydney, Sydney. Professor Lin Perry is Professor of Nursing Research and Practice Development at Prince of Wales Hospital and Faculty of Health, University of Technology Sydney, Sydney, NSW.
Osteoporosis
Bone diseases
Osteoporosis is a common condition in Australia with effective treatments available, yet it is mostly only identified after a fragility fracture and often not even then. Detection and management in general practice are essential for secondary and primary fracture prevention.
- Osteoporosis is a common lifelong condition that requires long-term management and monitoring.
- GPs have a key and enduring role in osteoporosis management, often in partnership with hospital-based services.
- Identification of at-risk patients using a systematic approach and arranging timely investigation enables best practice assessment and initiation of treatment.
- Opportunistic screening with bone health assessments should be incorporated into general health assessments for high-risk populations, with assistance, where possible, of practice nurses.
- Management of osteoporosis in primary care includes a personalised treatment regimen, education and monitoring.
- Allied health practitioner involvement, use of online resources and referral to osteoporosis community programs can enhance osteoporosis management.
Osteoporosis is a common systemic skeletal disease characterised by low bone mass and microarchitectural deterioration in bone with an increase in bone fragility and fracture risk.1 Estimated to affect 1.3 million Australians, it is often silent and only identified after a fragility fracture.2 Between 2017 and 2018, there were 93,321 hospitalisations in Australia for fragility fractures in people aged over 50 years.3 Despite the availability of safe, effective and affordable treatments for osteoporosis, most people remain undiagnosed and untreated.4 Many hospitals provide Osteoporosis Refracture Prevention (ORP) services that can identify and initiate treatment for those at greatest risk of refracture; however, this is only a small proportion of the osteoporosis population and these individuals also require long-term management in primary care. Hence GPs have an essential role in managing osteoporosis, both for primary and secondary fracture prevention. This article provides an overview of osteoporosis detection and management in primary care, including identifying patients at high risk of fractures, investigations, diagnosis, treatment options and monitoring.
Most osteoporosis care is secondary fracture prevention, to reduce the incidence of subsequent fractures by identifying and treating individuals who present with an initial osteoporosis-related fracture. However, ideally, individuals with osteoporosis are identified and treated ahead of any fragility fractures, as fracture risk escalates with each subsequent fracture if primary prevention is not delivered or its treatments are not adhered to.
Identification of fracture risk
Individuals presenting with a fragility fracture are at greatest risk of osteoporosis-related morbidity and mortality, and have the most to gain from interventions that reduce fracture risk. Dual-energy x-ray absorptiometry (DXA) measurement of bone mineral density (BMD) is used to support the clinical diagnosis of fragility fracture but is not essential in cases of hip or vertebral fracture. Any fragility fracture doubles the risk of a subsequent fracture and vertebral fractures are associated with a fourfold increased risk of further vertebral fracture.5,6 Fracture risk is greatest in the year after fracture and remains above that of the general population for more than five years, making timely identification and treatment critical for secondary fracture prevention.5
Treatment for fracture prevention
Safe and effective treatments are available for osteoporosis that reduce the risk of fracture and, in most instances, improve bone density. Strong evidence from randomised clinical trials supports the antifracture efficacy of drugs, including bisphosphonates, denosumab, oestrogens, tibolone, raloxifene (spine fractures only), teriparatide and romosozumab.7 Although often prescribed, calcium and vitamin D supplements produce only a small, nonprogressive increase in BMD without a reduction in fracture risk.8,9
Undertreatment of osteoporosis is common, both in primary and tertiary care. In 2004, 29% of women aged 60 years and older who presented to their GP had a history of fragility fracture after menopause, yet only 23% received antiosteoporosis medication.10 An audit of fragility fracture presentations to 16 Australian hospitals revealed only 10% of patients were investigated for osteoporosis, and only 6% were prescribed a bisphosphonate before discharge.11 Furthermore, only 60 to 73% of these patients persisted with antiresorptive therapy two years after initiation, potentially significantly reducing the expected financial and refracture benefits of antiosteoporosis medications.12-17
One successful approach to addressing this treatment gap is post-fracture care co-ordination programs. In Australia, these ORP services operate in more than 30 hospitals (from 2018 data).18 ORP services (also known as Fracture Liaison Services), are co-ordinated multidisciplinary services designed to systematically identify patients after an incident fracture, investigate for osteoporosis, inform patients about their diagnosis, initiate evidence-based treatment and improve long-term medication monitoring and adherence (Flowchart). Their outcomes include increased testing and treatment rates, improved medication adherence and reduced refracture prevalence.19
Management of osteoporosis in primary care
Primary care providers have a key role in the diagnosis and treatment of osteoporosis in patients with fragility fractures who do not present to hospital (around 60,000 per year) or who present to hospital without an ORP service. However, engagement and co-ordination between ORP services and primary care services are also required for patients who have received care in ORP services, especially for ongoing monitoring and follow-up.18 Health service fragmentation and poor communication between tertiary (or acute) services and primary care systems can lead to inadequate monitoring, poor treatment adherence and loss to follow up.20,21 GPs therefore have a crucial role in providing primary and secondary fracture prevention to those beyond the reach of and after discharge from ORP services.
Suggested strategies to enhance osteoporosis management in primary care are listed in Box 1. The systematic approach to secondary fracture prevention successfully employed by hospital-based ORP services (Flowchart) can be modified for use in primary care; it consists of four steps: identification of patients at risk of osteoporosis, appropriate investigations, initiation of treatment and follow up with appropriate monitoring.
{kind=link}
1. Identify patients at risk of osteoporosis
Many individuals will not associate their fragility fracture with osteoporosis or volunteer a history of fracture, even if recent.22 Case identification needs an active process to identify all individuals with a history of fragility fracture. Opportunistic screening could be introduced within routine clinic appointments. The Know Your Bones fracture risk assessment tool (https://knowyourbones.org.au) is a brief, free online questionnaire that graphically and numerically estimates baseline and adjusted fracture risks following treatment. Providing a link to the tool for individuals aged over 50 years before an appointment could potentially increase awareness of osteoporosis and prompt discussion of bone health. A bone health check could be incorporated into general health assessments within primary care, funded under the Medicare Benefits Schedule (MBS) Health Assessment item numbers.23 Fracture history should be routinely sought for all postmenopausal women aged over 45 years and men aged over 50 years. Hospital discharge summaries and outpatient imaging reports may identify recent fractures and should be reviewed, manually or preferably automated. Artificial intelligence models have been developed that can accurately and automatically identify patients with vertebral fractures from plain x-ray and CT scans.24,25 These systems may become widely adopted in the future.
The role of the practice nurse could be expanded to include bone health screening assessments, such as measurement of height and weight, medical history taking and fracture risk assessment. A loss of 3 cm or more in height over three years has a specificity of 96.9% and a positive predictive value of 63.1% for vertebral fracture.26
Any bone can break so it is important to question the mechanism of injury to identify fragility fractures. Consider if the fracture would have occurred if the same event (usually a fall) had happened when they were younger or healthier. Any fracture sustained from the force of a fall from standing height or less should be considered a fragility fracture. Postmenopausal women and men aged 50 years and older with a history of fragility fracture should be considered to have a presumptive diagnosis of osteoporosis.27
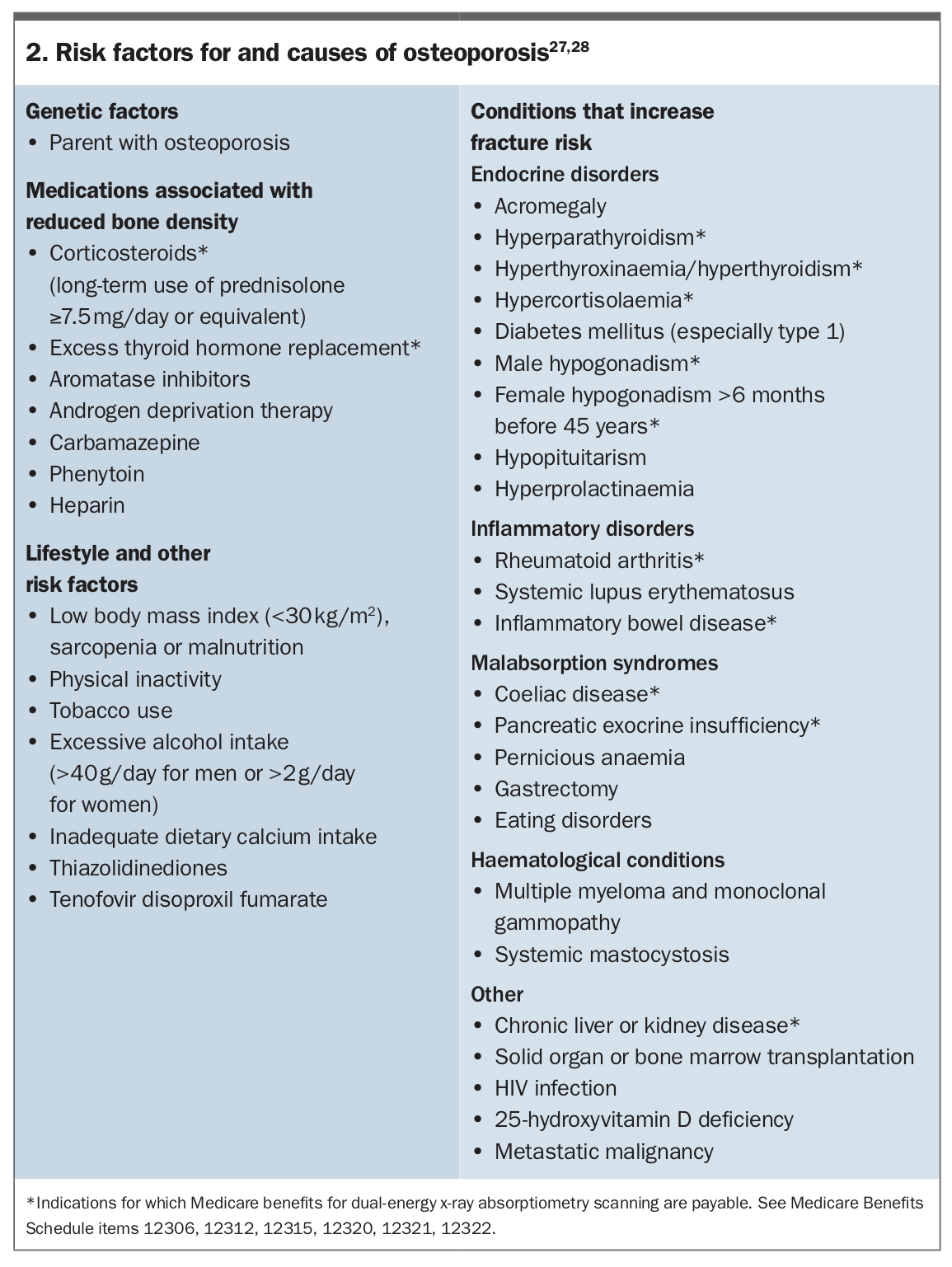
Clinical history and examination should focus on identifying major risk factors and causes of osteoporosis (Box 2) to inform further investigations. Regular medications should be reviewed to identify and minimise the use of drugs associated with reduced bone density and, where possible, deprescribe those associated with an increased risk of falls (e.g. sedative, anticholinergic, antipsychotic, antihypertensive and opioid medications).29 For older people with a history of falls and polypharmacy, a pharmacist-led medicines review may be helpful and may reduce medication-related falls.30 A detailed falls risk assessment should be performed in patients who sustained a fracture after falling, those with two or more falls in the last year or those with walking or balance difficulties.31
{kind=link}
2. Investigate patients at risk of osteoporosis
Laboratory investigations are performed to identify common treatable causes of poor bone health (e.g. hyperthyroidism) and conditions that require remediation (e.g. hypovitaminosis D, hypocalcaemia) and to inform treatment choices (e.g. a patient’s baseline renal function) (Flowchart).
All postmenopausal women and men aged 50 years and older with a fragility fracture should be referred for BMD measurement. Among those with non-hip and non-spine fractures, BMD measurement is important to support the diagnosis of osteoporosis before treatment is commenced. For those with a fragility fracture of the hip or spine, a diagnosis of osteoporosis can be assumed (regardless of BMD) and treatment should be started without delay.31 In these cases, baseline BMD testing enables subsequent monitoring of response to treatment and future assessment of candidacy for osteoanabolic therapy. Further investigation to assess for possible pathological fractures is warranted in patients with fragility fractures and normal or near normal BMD scores.
Additional investigations to assess for secondary causes of osteoporosis are warranted in individuals with suggestive clinical features or a BMD Z-score less than −2.0 SD. In cases of suspected secondary osteoporosis, referral to a specialist is recommended for investigation before treatment initiation.31
Vertebral fractures are the most common type of fragility fracture, affecting around 20% of men and women over 50 years of age.32 They are often asymptomatic and undiagnosed, or incidentally identified on imaging ordered for other reasons. Consider a thoracolumbar spine x-ray for anyone with unexplained back pain, kyphosis, or loss of height greater than 3 cm to assess for occult fracture. Graded by severity (I to III), in the absence of a significant history of trauma, the higher-grade occult vertebral fractures can generally be treated as osteoporosis. Nonfragility vertebral fractures may occur in young individuals, for example, men in manual occupations such as farming, but may not be detected until many years later. Careful history taking may uncover the initial traumatic episode.
3. Inform patients and initiate treatment
Following diagnosis, patient education includes three key messages.33 First, fracture is indicative of osteoporosis and the risk of refracture is high. To support this, an individual’s absolute fracture risk can be calculated using the Fracture Risk Assessment Tool (FRAX) (available online at https://www.sheffield.ac.uk/FRAX/tool.aspx?country=31) or Garvan Institute of Medical Research Fracture Risk Calculator (available online at https://www.garvan.org.au/promotions/bone-fracture-risk/calculator/). Second, fractures are associated with declines in mobility and independence, as well as a greater risk of premature death. Third, fracture risk can be reduced through treatment and regular follow up. These messages should be reinforced over time and consistent across healthcare providers.34
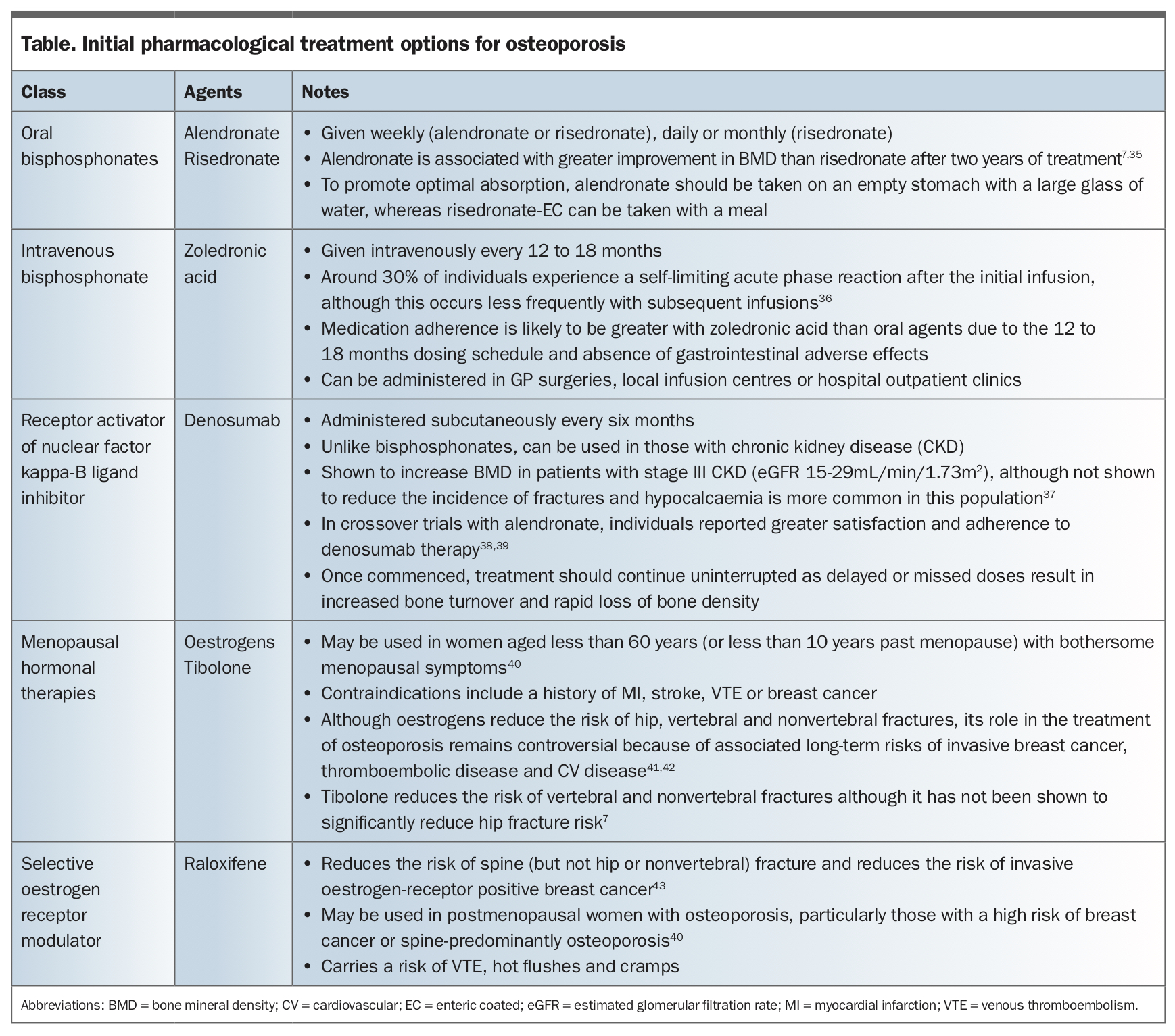
Individualised treatment-planning should incorporate pharmacological, nonpharmacological and falls risk-reducing elements. Initial pharmacological options and important prescribing points are shown in the Table. Nonpharmacological strategies to promote bone health are flagged in the Flowchart. Lifestyle risk assessment and care planning, and advice about diet, exercise and lifestyle can be provided with help from practice nurses if available. Consider referring all individuals with osteoporosis to a bone health-specific exercise program (such as high intensity resistance and impact training) or a physiotherapist, and those with a history of falls to an occupational therapist for a home assessment.44,45 Patient information can be found on the Healthy Bones Australia website (https://healthybonesaustralia.org.au) and the International Osteoporosis Foundation website (https://www.osteoporosis.foundation).
{kind=link}
4. Monitor patients
Osteoporosis treatments reduce fracture risk but are not curative and osteoporosis requires lifelong management. Long-term follow up of individuals with osteoporosis aims to optimise pharmacological and non-pharmacological management and address any complications or concerns.46 Long-term medication adherence and persistence poses challenges in every chronic disease but is essential to achieve the benefits shown in clinical trials.47 The role of practice nurses can include monitoring and interventions to support medication adherence, such as motivational interviewing, counselling and education.
Although the type and frequency of follow up required will vary between individuals, general recommendations are provided below.
- Review patients three to six months after treatment initiation or change to reinforce key messages and assess medication tolerability, adherence and persistence. Increasingly, this is occurring via telehealth.
- Arrange an annual clinical and biochemical review to reinforce key messages, identify any concerns, assess medication adherence and persistence, measure height, monitor biochemistry (renal function and 25-hydroxyvitamin D level) and encourage annual dental review.
- Repeat DXA (preferably using the same instrument) no sooner than 12 months after initiation or change in treatment to assess BMD response. If there has been no significant decline in BMD, the frequency of further scans can be widened based on risk factors and adherence. In some circumstances, it may be informative to repeat a DXA scan more frequently, e.g. after a fracture in a patient already on treatment, or annually in patients on prolonged high-dose corticosteroid therapy.
- Refer for a specialist opinion if refracture occurs after 12 months of continuous treatment, if significant loss of BMD in the lumbar spine or total hip occurs over a two-year period, if known or suspected secondary osteoporosis, if the fracture severity is disproportionate to BMD findings, or if advice is needed regarding the appropriateness or timing of a monitored break from treatment (previously termed ‘drug holiday’). Importantly, individuals with a history of fracture who experience a symptomatic new fracture after 12 months of therapy and have a BMD T-score of less than or equal to −3 SD may be eligible for osteoanabolic therapy (e.g. romosozumab) and should be referred for specialist assessment.
Serial BMD monitoring may help medication adherence among people with osteoporosis. One large observational study showed a reduction in fracture risk and greater medication use among women who had BMD monitoring within five years of treatment initiation compared with unmonitored women.48 Biochemical monitoring of bone turnover markers can be helpful in assessing adherence to therapy but does not improve it, and it is not recommended for routine care.39,40
Enhancing long-term follow up
Intervention to increase adherence will achieve substantial benefit. Ongoing monitoring and adherence support are core components of long-term care for patients at risk of fracture.
Medication monitoring may be effective when delivered virtually. Randomised trials have shown regular telephone follow up at various intervals improves short-term adherence and persistence with medication and lifestyle advice.51-54 The most successful interventions are multifaceted and individualised. This includes, for example, combining adherence monitoring with counselling.55 Compared with standard care, attendance at a nurse-led review to discuss wellbeing, medication issues and adverse effects showed a 57% improvement in adherence at 12 months.49
To combine patient counselling and education with monitoring, the clinician should seek to identify the nature of any medication issues (poor adherence, persistence or lack of initiation). They should measure the problem, identify the factors responsible and work with individuals to reach agreed solutions.55 These interventions can be performed by suitably trained GPs, nurses, pharmacists or other healthcare professionals. Practice nurses, in particular, are underused in this area and could provide medication monitoring and counselling for individuals with osteoporosis managed in primary care.
For those prescribed denosumab, the importance of regular review and monitoring is particularly important. Bone turnover rapidly rises and is followed by a decline in bone density after treatment discontinuation.56-58 In patients receiving six-monthly denosumab injections, automated recall and reminder systems should be used to avoid treatment delays. Such recall services are part of many standard practice management software systems.
All health sectors have increasingly adopted telehealth models of care in response to the coronavirus pandemic, including for the management of osteoporosis. The recent introduction of temporary MBS item codes for telehealth consultations has, for the first time, made widespread use of these services financially feasible. Early data indicate that ORP services can perform their core functions effectively and with positive consumer satisfaction through these models.59,60 The broader cost effectiveness of this model to the healthcare system and the effects on long-term medication adherence, persistence and refracture remain to be defined.
Primary fracture prevention in primary care
Primary fracture prevention aims to reduce the incidence of initial fractures by identifying individuals at risk of osteoporosis-related fractures, addressing modifiable risk factors and commencing evidence-based treatments before the first fracture. These patients can be identified through detailed clinical assessment and DXA measurement of BMD. Australian primary care guidelines recommend clinical fracture risk assessment for all postmenopausal women and men over 50 years with one or more risk factors for osteoporosis.31,61 This should include a history and physical examination to elicit risk factors for osteoporosis (Box 2), with DXA scan offered to those at increased risk. MBS items numbers cover DXA scan in all people aged over 70 years and younger people with selected risk factors for osteoporosis (Box 2). Non-MBS (private) DXA scans can be offered to individuals who are at increased risk of osteoporosis but do not meet subsidy criteria. The effectiveness and cost effectiveness of universal screening in an Australian setting is yet to be determined. One UK trial showed a systematic community-based DXA screening intervention for women aged over 70 years with an increased risk of fracture was feasible and reduced the incidence of hip fractures, however, a similar study from Denmark did not show a reduction in fracture incidence.62,63
Conclusion
Substantial evidence to practice gaps across routine management of osteoporosis offer enormous opportunities for clinicians to make a difference to patient outcomes. Evidence-based treatments have established the achievable benefits of pharmaceutical and nonpharmaceutical interventions, yet the full realisation of these potential benefits depends on the effective delivery, uptake and adoption of these treatments. Primary care plays an essential role in managing osteoporosis for fracture prevention and better quality of life for those affected. Proactive use of existing resources within and outside the practice can enable GPs to enhance the effectiveness of bone health treatments and refracture prevention services, whether delivered solely in primary care or as partners in a collaborative model spanning primary to tertiary care. GPs are well placed to not just ‘make the first fracture the last fracture’, but to prevent the occurrence of all fragility fractures. ET
COMPETING INTERESTS: None.