Growth hormone replacement therapy in adults: when does it have a role?

Growth disorders
Endocrine diseases
Growth hormone deficiency (GHD) in adults is characterised by abnormal body composition, skeletal effects, impaired physical function, unfavourable metabolic profile and reduced quality of life. The diagnosis of GHD requires biochemical confirmation with growth hormone stimulation testing in the context of an appropriate clinical history. Growth hormone replacement therapy benefits patients with confirmed adult GHD.
- Growth hormone deficiency (GHD) in adults is characterised by abnormal body composition, impaired physical function, metabolic and cardiovascular risks, adverse skeletal effects and reduced quality of life.
- The diagnosis of GHD is confirmed by appropriate clinical history and rigorous biochemical criteria.
- Biochemical diagnosis is essential and requires the demonstration of impaired growth hormone secretion in response to provocative stimuli. Only patients who are at risk of GHD should be tested.
- Growth hormone replacement therapy in adults with GHD improves the signs and symptoms of GHD and quality of life.
- From 1 December 2018, growth hormone replacement therapy has been available on the PBS for severe GHD in adults.
Adult growth hormone deficiency (GHD) is a clinical syndrome characterised by abnormal body composition, an unfavourable metabolic and cardiovascular profile, decreased physical fitness and diminished quality of life.1 The diagnosis of GHD is based on biochemical criteria demonstrating a diminished growth hormone response to provocative stimuli in the context of a pituitary or hypothalamic disorder.2
Replacement therapy with recombinant human growth hormone, also known as somatropin, has been available since the 1980s.3 Extensive experience since then has provided overwhelming evidence that growth hormone replacement therapy improves or reverses many of the signs, symptoms and consequences of GHD in adults. Growth hormone replacement therapy has long been listed on the PBS for children with GHD and other causes of significant short stature, but recently the PBS listing was extended to include adults with severe GHD.
This article provides an overview of growth hormone regulation and physiology and discusses GHD in adults, including aetiology, diagnosis and prescribing of growth hormone replacement therapy.
Growth hormone regulation
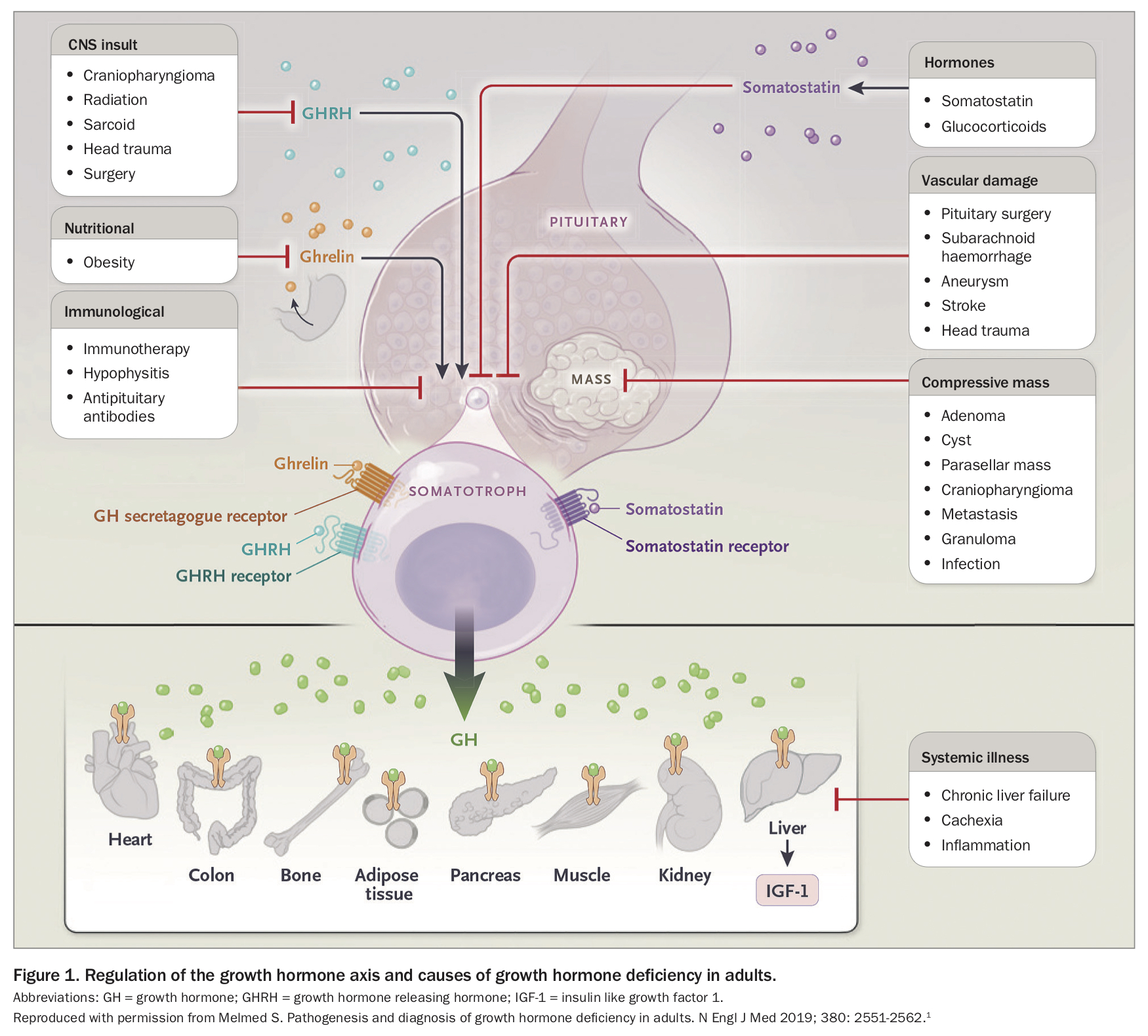
Growth hormone is a 191-amino acid polypeptide secreted by the somatotroph cells of the anterior pituitary gland. Secretion of growth hormone is primarily regulated by hypothalamic-derived growth hormone-releasing hormone (GHRH) and somatostatin, as well as complex gut, liver and gonadal signals (Figure 1).1 GHRH and somatostatin, both produced by the hypothalamus, reach the anterior pituitary via the hypothalamic-hypophyseal portal system. GHRH stimulates growth hormone secretion via signalling through somatotroph cell surface G protein-coupled receptors, and somatostatin inhibits growth hormone secretion by impairing the response to GHRH.1,4 Various neuropeptides, neurotransmitters and amino acids modulate GHRH action and growth hormone release.1 Ghrelin, derived from the gastrointestinal tract, and its synthetic mimetics also stimulate growth hormone secretion and synergise the action of GHRH.1 Growth hormone release is inhibited by glucose loading, fatty acids and visceral adiposity, and increased by amino acids such as arginine and leucine, sleep, stress, exercise and insulin-induced hypoglycaemia.1,4 Growth hormone release is also suppressed by insulin-like growth factor 1 (IGF-1), the peripheral target hormone for growth hormone, via negative feedback mechanisms. Glucocorticoids, oestrogen, testosterone and thyroid hormones are also involved in regulation of growth hormone production.4,5
{kind=link}
Growth hormone secretion is affected by age, nutritional status, chronic illnesses and sex. Production of growth hormone peaks during mid-adolescence and declines after cessation of growth, then remains stable through to mid-adulthood before progressively declining with ageing.1,4 Growth hormone is secreted in a pulsatile pattern, with most pulses occurring at night. Nadir growth hormone levels occur during the day, and daytime growth hormone levels are often undetectable.1,6 The half-life of circulating growth hormone is short, being about 14 minutes.1
Growth hormone physiology
Growth hormone receptors are present in multiple tissues, including liver, cartilage, muscle, adipose tissue, bone, brain, heart and kidney.1,7 The action of growth hormone is mediated both directly through activation of the growth hormone receptor, and indirectly by inducing production of IGF-1.7 IGF-1 is a 70-amino acid protein produced in several tissues, and mediates most of the growth-promoting actions of growth hormone.7 Locally-derived IGF-1 exerts tissue-specific autocrine and paracrine growth-promoting actions, and circulating IGF-1, predominantly produced in the liver, mediates endocrine effects.4 Growth hormone is the primary regulator of IGF-1,7 but other factors are also involved, including oestrogen, which reduces hepatic sensitivity to growth hormone and decreases synthesis of IGF-1.6
Growth hormone is an important metabolic hormone. Its main actions are optimisation of body composition and physical function and regulation of energy and substrate metabolism.8 Both growth hormone and IGF-1 have anabolic effects on skeletal muscle and bone, increasing muscle mass and bone formation, reducing fat mass and increasing total body water.1,7 Growth hormone increases lipolysis and protein synthesis and decreases hepatic and muscle insulin sensitivity and glucose uptake. Growth hormone also increases the peripheral conversion of thyroxine to triiodothyronine, and cortisol to the inactive metabolite, cortisone.4
Causes of acquired adult growth hormone deficiency
GHD in adults usually results from acquired hypothalamic–pituitary disease. Pituitary tumours or other sellar masses cause about two-thirds of adult GHD9 owing to compression and compromise of somatotroph function or treatment with radiation or surgery.1 Less common causes include traumatic brain injury, infiltrative or granulomatous hypothalamic–pituitary disease, infections, haemorrhage and cranial irradiation.1,9
The likelihood and severity of GHD increases with increasing number of other pituitary hormone deficiencies.10,11 The probability of GHD in patients with three or four pituitary hormone deficiencies ranges from 96 to 100% compared with 41% for patients with one pituitary hormone deficiency.12
Clinical features of growth hormone deficiency in adults
GHD in adults is associated with a clinical syndrome characterised by abnormal body composition, impaired physical function, unfavourable metabolic effects, increased cardiovascular risk, reduced life expectancy and diminished quality of life (Figure 2).13-15 Fat mass is increased with greater central fat distribution and reduced lean body mass, muscle strength and physical fitness.16 The lipid profile is impaired, with increased total cholesterol, LDL cholesterol and triglyceride levels, as well as decreased HDL cholesterol levels in women.14 Insulin sensitivity is also reduced.17
{kind=link}
Patients with GHD have elevated inflammatory markers, impaired fibrinolysis, endothelial dysfunction, impaired cardiac functional reserve, reduced left ventricular mass and systolic function and increased cardiovascular mortality.15,18-22 Skeletal effects, including low bone turnover, decreased bone mineral density and increased vertebral fractures, are also observed.23 Patients with GHD report significantly impaired quality of life, with reduced energy and motivation, increased emotional lability, disturbed sex life and feelings of isolation.24,25
How to test for growth hormone deficiency
The diagnosis of GHD in adults is established by an appropriate clinical history and stringent biochemical criteria. The overall accuracy of available tests depends on the pretest probability, and only patients at risk of adult GHD, such as those with a history of acquired pituitary disease, surgery, radiation therapy, head trauma or documented deficiencies in other pituitary hormones should generally be tested for GHD.2 Since a misleading diagnosis of GHD may be made in some patients with normal pituitary function, testing for GHD should not be performed in patients with nonspecific symptoms such as weakness, frailty or obesity, or in a clinical context where GHD is considered unlikely.1 The diagnosis of idiopathic GHD is particularly difficult, and strict criteria are necessary, including the use of two growth hormone stimulation tests to confirm the diagnosis.2 Testing for GHD should not be performed until other hormones are adequately replaced.2
Growth hormone and IGF-1 levels
Random measurements of serum growth hormone levels are insufficient for a diagnosis of GHD because growth hormone secretion is pulsatile.1 An IGF-1 measurement is also not suitable as a single test for diagnosing or screening for GHD in adults.
IGF-1 levels are influenced by multiple factors in addition to growth hormone, including age, gender and serum insulin levels, and there is significant overlap in plasma IGF-1 levels between individuals with and without GHD.26 In fact, 42% of patients with GHD have normal IGF-1 levels for age and sex.10 However, an IGF-1 level below the age-adjusted reference range, in the absence of conditions such as poorly controlled diabetes, liver disease and use of oral oestrogen therapy, and in the presence of other pituitary hormone deficiencies, strongly supports significant GHD and may help identify patients who would benefit from growth hormone replacement therapy.2 An accurate measurement of growth hormone secretion is only obtained by measuring the secretory reserve in response to provocative stimuli.
Insulin tolerance test
The insulin tolerance test (ITT) is the gold-standard test for the diagnosis of GHD.2 This test assesses the function of the complete hypothalamic-somatotroph axis and is of use in both pituitary and hypothalamic disease. Although safe when performed by experienced clinicians, the ITT can be labour intensive and unpleasant for patients, and is contraindicated in the elderly and patients with cardiac disease or seizure disorders.2,27 The test has a sensitivity and specificity of 96% and 92%, respectively, using a peak growth hormone cut-off level of 5.1 mcg/L.27 The PBS criterion for the treatment of severe GHD in adults, which aligns with the TGA registration, is a peak growth hormone level of less than 2.5 mcg/L.
Arginine test
Arginine is a weaker stimulant of growth hormone secretion, and therefore lower growth hormone cut-offs are required. A peak growth hormone level of less than 0.4 mcg/L after arginine stimulation is the PBS criterion for growth hormone replacement therapy. It has a sensitivity of 87% and specificity of 91% for the diagnosis of GHD.27 Side effects are uncommon and include paresthesia, dry mouth, nausea, vomiting and headache.27,28
Glucagon stimulation test
The glucagon stimulation test is a practical and frequently used alternative to the ITT.The sensitivity and specificity have been reported as 97% and 88%, respectively, using a peak growth hormone cut-off of 3.0 mcg/L.29 The release of growth hormone following glucagon administration is delayed, and growth hormone measurement over four hours is recommended.30 Nausea, vomiting and headache may occur.1 The mechanism by which glucagon stimulates growth hormone secretion is not yet fully elucidated.30 Blood glucose monitoring should be performed during and after the test, as there is a risk of delayed hypoglycaemia.1 The standard glucagon dose is 1 mg administered via intramuscular injection. Obesity may blunt the growth hormone response, and a higher dose of 1.5 mg glucagon is recommended in patients with a body weight of more than 90 kg.1 Recent research has suggested that there should be reduced weight-based diagnostic cut-offs to prevent a high frequency of false-positive glucagon tests in obese patients.28 However, in Australia, the current PBS criteria are based on the single peak growth hormone cut-off value of 3.0 mcg/L.
Growth hormone secretagogues
More recently, macimorelin, an oral growth hormone secretagogue, has been proposed for the diagnosis of GHD. Macimorelin has a diagnostic accuracy similar to that of the ITT for diagnosis of GHD, with a sensitivity and specificity of 92% and 96%, respectively, using a peak growth hormone cut-off value of 5.1 mcg/L. It is not yet routinely available in Australia and disadvantages include QT prolongation and the potential for misdiagnosis of hypothalamic disease.31
Benefits of growth hormone replacement therapy in adults
Growth hormone replacement therapy in adults with GHD has been extensively shown to improve signs and symptoms of GHD (Table). Body composition is improved, with decreased adipose volume, increased muscle volume and lean body mass, and increased muscle strength and exercise capacity.32,33 Growth hormone improves lung capacity by increasing respiratory muscle strength and lung volume, as well as red cell mass, which determines the oxygen carrying capacity of the blood.34-38 Cardiovascular benefits include improvement in the lipid profile, normalisation of impaired fibrinolysis, a reduction in diastolic blood pressure, inflammatory markers and carotid intima media thickness and an increase in left ventricular mass and systolic function.17,18,39-42 Glomerular filtration rate and renal plasma flow are also improved with use of growth hormone replacement therapy.43 The effect on glucose homeostasis is somewhat unclear, with both increased and unchanged fasting blood glucose levels, and decreased HbA1c level observed.17 Growth hormone replacement therapy increases total body and lumbar spine bone mineral density.23 Quality of life and wellbeing are markedly improved.4,33,44
{kind=link}
Clinical benefits of growth hormone replacement therapy may not become apparent until after at least six months.2 Hypopituitarism is associated with increased mortality, but current studies do not allow a definitive statement on whether growth hormone replacement therapy has any effect on this.1 The effect of other pituitary hormone deficiencies, particularly secondary adrenal insufficiency, is a significant confounding factor when interpreting observational studies, and long-term, placebo-controlled trials powered for mortality have not been undertaken.
Prescribing growth hormone replacement therapy
As of 1 December 2018, the PBS listing for growth hormone replacement therapy was extended to include adults with severe adult GHD, based largely on the New Zealand criteria.45 Initially, to qualify for the PBS listing, impaired quality of life had to be demonstrated, as assessed by the Quality of Life-Assessment of Growth Hormone Deficiency in Adults outcome measure, but this criterion was subsequently removed from the PBS criteria on advice from the Pharmaceutical Benefits Advisory Committee.
The following criteria must be met to qualify for PBS-subsidised adult growth hormone replacement therapy.
- Undergoing treatment by an endocrinologist.
- Documented hypothalamic or pituitary disease for adult-onset GHD, or a congenital, genetic or structural cause of childhood-onset GHD.
- Meet growth hormone stimulation testing criteria by using ITT, arginine infusion test or glucagon stimulation testing.
- A baseline IGF-1 level within the previous 12 weeks of application (not required to be abnormal, but documented as a baseline measure).
Growth hormone replacement therapy currently requires the administration of daily subcutaneous injections, although longer-acting formulations with improved dosing profiles are in various stages of development.46
Adverse effects
Growth hormone replacement therapy is generally well tolerated. Dose-dependent adverse effects due to water retention occur in 5 to 18% of patients, and include arthralgia, myalgia, oedema, paraesthesia and carpal tunnel syndrome.3 Sleep apnoea, hypertension, insomnia and hyperglycaemia may also occur.47,48 Women, elderly patients and those with a higher body weight are more susceptible.3 Adverse effects can be minimised by commencing growth hormone replacement at low doses followed by careful titration.2,3 If adverse effects occur, improvement is often achieved with dose reduction.3,47 Growth hormone replacement therapy has a favourable safety profile, and there is no evidence for increased death, malignancy or recurrence of intracranial tumours.3,47,49
Growth hormone dosing
In contrast to weight-based dosing of growth hormone in children, dosing in adults draws on physiological data showing that women secrete more growth hormone than men and growth hormone production declines with age. A starting dose of 0.2 to 0.3 mg daily in adults is generally tolerated without adverse effects. The dose should be titrated every one to two months by 0.1 to 0.2 mg daily, according to clinical response, side effects and IGF-1 level. Adults over 60 years of age may benefit from a slightly lower starting dose of 0.1 to 0.2 mg daily and slower titration to reduce the risk of adverse effects, whereas young adults aged less than 30 years may benefit from slightly higher starting doses of 0.4 to 0.5 mg daily.2
As higher levels of oestrogen within the liver inhibit secretion of IGF-1, women taking oral, but not transdermal, oestrogen have increased growth hormone requirements.50 Therefore, women with concurrent growth hormone and oestrogen deficiency in the setting of hypopituitarism should have their oestrogen administered preferentially via the transdermal route.
Monitoring
The target IGF-1 level for adults receiving growth hormone replacement therapy is generally within the upper half of the age-related reference age.2 Due to the effects of growth hormone on thyroid hormone and cortisol metabolism, growth hormone replacement therapy may unmask underlying hypothyroidism or hypoadrenalism. Monitoring of thyroid and adrenal function is recommended and doses of replacement thyroxine and hydrocortisone may need adjustment.3 In patients with diabetes mellitus, glycaemia profile should be monitored and dose adjustments in antidiabetic medications made if required.2 Careful growth hormone dose titration is recommended for patients at increased risk of sleep apnoea or cardiopulmonary disorders.47 Growth hormone replacement therapy is contraindicated in the presence of active malignancy.2
Conclusion
Growth hormone acts to mediate growth and metabolic functions. GHD is characterised by abnormal body composition, impaired physical function, metabolic and cardiovascular risks, adverse skeletal effects, increased mortality and reduced quality of life. Adults with GHD require careful assessment and investigation to confirm the diagnosis. Growth hormone replacement therapy is indicated for severe GHD and improves many of the symptoms and consequences of GHD, is generally well tolerated and has a favourable safety profile. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.