Managing complex cases of diabetes

Diabetes complications
Diabetes medicines
Recognising and investigating patients with ‘peculiar’ cases of diabetes is crucial for effective management. Five clinical vignettes explore complex scenarios in diabetes care, including latent autoimmune diabetes of adulthood, young-onset type 2 diabetes, post-transplant diabetes mellitus, euglycaemic diabetic ketoacidosis and pancreatic cancer risk with glucagon-like peptide-1 therapy.
- The clinical presentation of diabetes is diverse and certain clinical features can help identify patients who require more detailed assessment.
- Reaching a specific diabetes diagnosis and understanding the underlying pathophysiology is important for optimal management.
- Most people with diabetes are managed in primary care, although those with complex cases of diabetes often benefit from the involvement of a multidisciplinary team, including an endocrinologist.
- As therapeutics in diabetes are rapidly advancing, clinicians need to be vigilant for potential adverse effects and provide appropriate education to patients.
Keeping up to date with the classification and treatment of diabetes mellitus has become increasingly challenging. Several diagnostic entities fall under the umbrella of diabetes, and the past decade has seen the emergence of novel therapies and devices. Here, we explore some of the enigmas of diabetes management in a case-based discussion.
Case 1. Latent autoimmune diabetes of adulthood
Michael, aged 45 years, has returned to your surgery after being discharged from the local emergency department. He is a long-term patient who was diagnosed with type 2 diabetes five years ago. He has been taking metformin 1 g twice daily and his HbA1c three months ago was 6.4%. He has a body mass index (BMI) of 28.5 kg/m2 and a waist circumference of 88 cm. Apart from mild hypertension, he has no significant past medical history. He has no family history of diabetes. His sister has systemic lupus erythematosus.
Michael presented to hospital after an episode of syncope and was found to have a random blood glucose level of 20 mmol/L and an HbA1c of 10%. He was started on modified-release gliclazide 12 mg in the morning and insulin glargine 20 units at night. Serological tests found he is positive for glutamic acid decarboxylase (GAD) 65 antibodies.
What is latent autoimmune diabetes of adulthood?
Latent autoimmune diabetes of adulthood (LADA) is an autoimmune form of diabetes that occurs typically but not exclusively in people older than 30 years. Phenotypically and genetically there are commonalities with both type 1 and type 2 diabetes, which have given rise to the term ‘type 1.5 diabetes’.1 The American Diabetes Association considers LADA as part of the spectrum of type 1 diabetes rather than a distinct entity.2 LADA evolves with a more insidious onset of insulin deficiency than type 1 diabetes. As a result, the clinical prodrome of hyperglycaemic symptoms may be prolonged, and initiation of insulin therapy can often be delayed for several months or years without ensuing diabetic ketoacidosis.
Although the prevalence of diagnosed LADA in the Australian population is low (less than 1%), almost 5% of those with clinically defined type 2 diabetes may in fact have LADA.3 We therefore advocate targeted screening for the condition.
When and how should we screen for LADA?
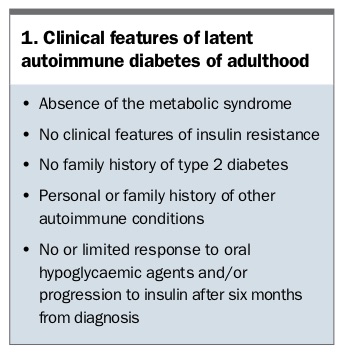
Clinical features that raise suspicion for LADA are listed in Box 1. Autoimmune antibody screening is akin to that used in patients with suspected type 1 diabetes. GAD65 antibodies are the most common antibodies detected, but testing for the tyrosine phosphatase-related islet antigen-2 (IA-2) and zinc transporter 8 autoantibodies (Zn-T8) can identify additional cases.4 Patients with a high GAD titre are more likely to progress to requiring insulin.1
{kind=link}
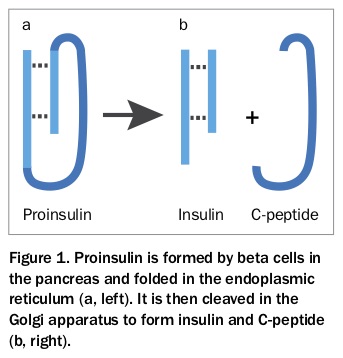
C-peptide is a cleavage product of insulin production and is therefore a useful marker of endogenous insulin secretion (Figure 1). Before insulin administration and in the presence of hyperglycaemia, a low-to-normal fasting C-peptide level supports relative insulin deficiency. In contrast, an elevated C-peptide level indicates intact insulin secretion.
{kind=link}
Additionally, it is worth considering the possibility of concurrent autoimmune conditions. Was there more to Michael’s syncopal episode than dehydration? He may have arrhythmia secondary to Graves hyperthyroidism or postural hypotension secondary to Addison’s disease. Hashimoto’s thyroiditis and coeliac disease also cluster with autoimmune diabetes.
Is specialist referral required?
Patients with diabetes can be managed appropriately in primary care. Referral to an endocrinologist may be indicated to confirm the diagnosis or to escalate treatment. Patients benefit from receiving diabetes education in a multidisciplinary environment, particularly when insulin therapy is initiated.
Case 2. Young-onset type 2 diabetes
Rebecca is a 15-year-old Indigenous girl who arrives at your outreach clinic with her concerned mother. Rebecca was recently diagnosed with diabetes, and both her parents and older brother have type 2 diabetes.
Rebecca has struggled with weight gain since puberty and has a BMI of 32 kg/m2. Her menstrual cycles have become irregular, and her last menstrual period was two months ago. She has no clinical signs of insulin resistance.
Rebecca has been taking extended-release metformin 1 g at night for three months. Her HbA1c today is 8.0%. She is clearly distressed by the diagnosis and particularly the risk of long-term complications that she has seen affect her family members.
Why distinguish ‘young-onset’ type 2 diabetes?
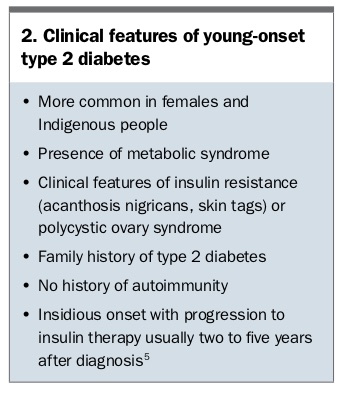
The rising prevalence of type 2 diabetes in adolescents and young adults is of international concern. In Australia, 400 new cases of type 2 diabetes are diagnosed annually in people aged between 10 and 24 years, and the incidence is at least fourfold higher among Aboriginal and Torres Strait Islander people.5 Contributing factors include intrauterine exposure to hyperglycaemia and overnutrition, diet, inadequate physical activity, obesity, low socioeconomic status, family history of type 2 diabetes and the metabolic syndrome, ethnicity and comorbid conditions, particularly polycystic ovary syndrome and nonalcoholic fatty liver disease.6 The clinical features of young-onset type 2 diabetes are listed in Box 2.
{kind=link}
It is important to recognise the psychosocial impact of a diabetes diagnosis in this age group, particularly the burden it places on an individual’s relationships and career. Furthermore, young-onset type 2 diabetes has been associated with greater risk of renal and nerve complications and higher standardised mortality, in part because of the duration of hyperglycaemia.7 Mortality for people diagnosed at age 15 to 29 years peaks at the age of 40 years.7 Therefore, managing cardiovascular risk factors is crucial in the young patient.
What are the priorities in this patient’s care?
Building rapport is of utmost importance, as maintaining the patient’s long-term engagement with health services is likely to improve outcomes. Consultations should therefore be delivered in a supportive, nonjudgemental and collaborative manner. An open discussion around mental health is encouraged, and the offer of psychologist referral as part of standard care is often welcomed.
A holistic approach to care includes a discussion of dietary and lifestyle interventions. The possibility of a reduced medication burden or even diabetes remission can motivate patients to achieve weight loss. However, setting unrealistic expectations, such as promises of long-term ‘cure’, is counterproductive. If the patient consents, engaging a partner or family member in their management plan can be useful. Contraception and pregnancy planning should also be discussed early.
Is specialist referral required?
Access to multidisciplinary care is preferable for patients with young-onset type 2 diabetes to ensure cohesive advice is provided by a team experienced in diabetes management. The team should include a diabetes educator and dietitian, and ideally an exercise physiologist and psychologist. Multidisciplinary care may be best delivered by a specialist service where available. Nevertheless, maximising engagement and adherence is a priority, and some patients may find primary care more approachable.
Case 3. Post-transplant diabetes mellitus
Mark, a 60-year-old man living in rural Australia, attends your clinic. His primary medical issue is idiopathic pulmonary fibrosis, which progressed over the past five years despite medical therapy to cause severe functional limitation and a requirement for home oxygen. He has undergone bilateral lung transplantation.
Despite normoglycaemia being demonstrated during the work-up for the transplantation, Mark has developed post-transplant diabetes mellitus (PTDM). He required an insulin infusion in the intensive care unit immediately after the transplantation while receiving parenteral feeding and high-dose intravenous corticosteroids. His immunosuppressant regimen now includes tacrolimus and prednisone 10 mg in the morning, and he takes modified-release gliclazide 60 mg in the morning for diabetes.
What are the predictors for post-transplant diabetes mellitus?
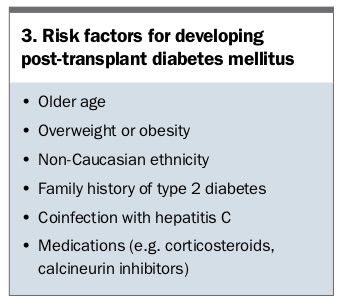
The incidence of PTDM is high after solid organ transplantation; PTDM affects up to half of all patients, although the proportion depends largely on the immunosuppressive regimen used.8 In our experience, about two-thirds of lung transplant recipients without cystic fibrosis develop PTDM, whereas the condition is almost universal in patients with cystic fibrosis.9 Risk factors for PTDM are shown in Box 3.
{kind=link}
Early recognition and initiation of treatment of PTDM is important given that diabetes increases the risk of infection, graft failure and mortality after transplantation.10 In a study of 367 lung transplant recipients, PTDM reduced mean survival by more than five years compared with those without diabetes.11 Our centre at St Vincent’s Hospital Sydney has protocolised screening for diabetes as part of the pre-transplant work-up and again six to 12 weeks after transplantation using standard diagnostic criteria, including a two-hour oral glucose tolerance test if overt hyperglycaemia is not detected. The diagnostic criteria used and classification are different for patients with cystic fibrosis.9
How does management differ between PTDM and other types of diabetes?
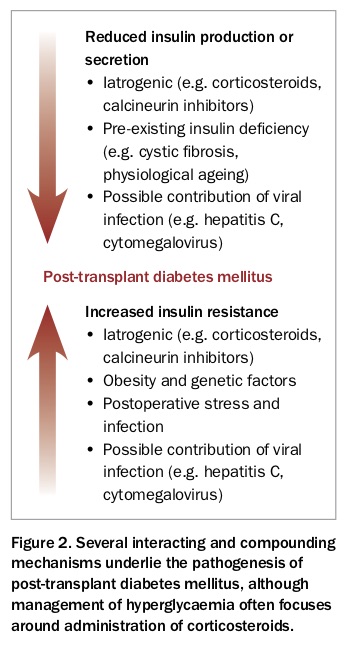
Treatment of PTDM is tailored to the individual, taking into consideration the use of concomitant medications (particularly corticosteroids), need for titratability, pattern of hyperglycaemia, reduced insulin secretion and sensitivity and avoidance of side effects (Figure 2). Immediately after the transplantation, an insulin infusion is usually initiated, with a transition to isophane insulin or gliclazide thereafter.
{kind=link}
Evidence supporting the use of novel hypoglycaemic therapies is scarce in this area. At our centre, introducing empagliflozin several years after heart transplantation led to significant reductions in blood pressure and BMI, as well as an expected reduction in HbA1c of 0.6%.12
A suggested approach to managing PTDM in contrast to general management of type 2 diabetes is presented in the New-Onset Diabetes After Transplantation 2003 International Consensus Guidelines .13
Is specialist referral required?
Transplant recipients require closely integrated care between GPs in the community and highly specialised transplant units. Inclusion of an endocrinologist in this team serves to address metabolic and bone health in the high-risk patient, with proposed advantages including greater efficiency of care, improved quality of life, lower hospital admission rates and improved survival.
Case 4. Sodium-glucose cotransporter-2 inhibitors and diabetic ketoacidosis
You are the doctor on duty for the local emergency department when you receive a call about Judy, a 55-year-old woman who arrived by ambulance with hypotension and vomiting. Measurement of venous blood gases shows metabolic acidosis with a pH of 7.15 and a blood glucose level of 10.5 mmol/L.
Judy has had type 2 diabetes for 20 years and is being treated with metformin, dapagliflozin and insulin glargine. She has been preparing for a colonoscopy tomorrow and therefore has not taken insulin for two days to avoid hypoglycaemia. Because of nausea she did not tolerate a clear fluid diet today.
You suspect euglycaemic diabetic ketoacidosis associated with the sodium-glucose cotransporter-2 (SGLT-2) inhibitor. A high blood ketone level (5 mmol/L) is confirmed by bedside point-of-care testing. After assessing the need for potassium replacement, you commence an insulin-dextrose infusion.
How common is this adverse effect of SGLT-2 inhibitors?
Euglycaemic diabetic ketoacidosis is defined by the triad of:
- increased anion gap metabolic acidosis
- ketosis
- relative euglycaemia (glucose level less than 11.1 mmol/L).
The presence of relative euglycaemia may mask and delay the diagnosis of underlying ketoacidosis. Hence, the TGA released a formal alert in August 2015.14
As of April 2017, the TGA had received 82 notifications of SLGT-2 inhibitor-associated diabetic ketoacidosis, 20% of which were considered life threatening.15 The condition is reported both in patients with type 1 diabetes and in those with type 2 diabetes. Use of SGLT-2 inhibitors in type 1 diabetes is off-label. Diabetic ketoacidosis should prompt screening for autoimmune diabetes (type 1 diabetes or LADA) in a patient previously diagnosed with type 2 diabetes. Nevertheless, we have seen several cases of euglycaemic diabetic ketoacidosis in patients with longstanding type 2 diabetes, who likely had insulin deficiency due to secondary islet cell failure.16
What is the pathogenesis and can it be prevented?
SGLT-2 inhibitors lead to increased glucagon and reduced insulin secretion from the pancreas, which in turn enhances release of free fatty acids and production of ketones. In states of endogenous insulin deficiency, such as autoimmune diabetes or long-term type 2 diabetes, cessation or reduction of exogenous insulin administration compounds this effect. Caloric losses through glycosuria are heightened by fasting, and as ketoacidosis progresses, nausea leads to a further reduction in caloric intake (Figure 3).17
{kind=link}
To prevent this cascade, we recommend withholding SGLT-2 inhibitors for at least three days either side of an anaesthetic procedure and during periods of fasting or low carbohydrate intake. This approach is supported by the Australian Diabetes Society.18 Insulin should be continued, although dose adjustment may be needed for patients with insulin deficiency. Patients should be educated about this potential adverse effect and equipped with a ketone-meter where appropriate.
Is specialist referral required?
Diabetic ketoacidosis requiring insulin-dextrose infusion is best managed in a high-dependency setting, and therefore referral is essential.19 Specialist consultation is advised before recommencing an SGLT-2 inhibitor following an episode of euglycaemic diabetic ketoacidosis.
Case 5. Glucagon-like peptide-1 and pancreatic cancer
Peter, aged 35 years, returns to see you after an appointment with his endocrinologist. He developed type 2 diabetes three years ago and has been treated with lifestyle intervention and metformin. Comorbidities include obesity and excessive alcohol consumption. His father and brother also have type 2 diabetes. His maternal grandfather died from pancreatic cancer.
A recent HbA1c measurement was 7.7%. Peter was advised to commence exenatide, which might help his efforts to lose weight in addition to improving glycaemic control. Peter has been reading about glucagon-like peptide-1 (GLP-1) therapy on the internet and asks you about the risk of cancer associated with its use.
Does GLP-1 therapy increase cancer risk?
Early studies raised concern about a potential link between incretin therapies (GLP-1 and dipeptidyl peptidase 4 [DPP-4]) and pancreatic disease, including pancreatitis and pancreatic cancer. GLP-1 has a trophic effect on pancreatic beta cells, and it was therefore theorised that incretin therapies might stimulate premalignant lesions rather than induce new neoplasms.20 Importantly, international authorities advised continuing the use of these medications given that causality was unsubstantiated.21 In particular, increased vigilance with newer therapies may have led to a reporting bias, and diabetes and obesity independently increase the risk of pancreatic cancer.
A recent meta-analysis of 33 studies (79,971 participants) found that pancreatic cancer risk was not increased by incretin therapies (odds ratio, 0.67; 95% confidence interval, 0.44 to 1.01).22 Further, it is worth considering the significant reduction in major adverse cardiovascular events, cardiovascular mortality and all-cause mortality associated with these treatments.23 Nevertheless, pancreatitis is listed as a rare adverse effect in the product information for incretin therapies, and we avoid prescribing these agents in patients with known risk factors for pancreatitis. Of note, chronic pancreatitis is a known risk factor for pancreatic cancer.
Further, rodent studies suggested an increased incidence of medullary thyroid cancer with GLP-1 therapy.24 Importantly, parafollicular (C) cells in the human thyroid behave differently to those in the rodent when exposed to incretin therapy, because of their much lower expression of GLP-1 receptors.25 There is no evidence that incretin therapy increases thyroid cancer risk in humans.
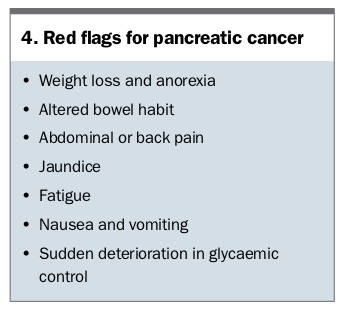
What are the ‘red flags’ for pancreatic cancer in diabetes?
The diagnosis of pancreatic cancer is often delayed because of the absence of symptoms in early disease or attribution of symptoms to another illness. For example, a new diagnosis of diabetes with marked hyperglycaemia may in itself explain weight loss and fatigue. Nevertheless, it is important to consider the diagnosis in patients presenting with red flags (Box 4), particularly in the absence of traditional risk factors for diabetes.
{kind=link}
CT with contrast using a ‘pancreatic protocol’ is the preferred modality for diagnosis as sensitivity and specificity are high.26 Smaller lesions not identifiable on CT may be detected on specialised imaging, such as endoscopic ultrasound examination. Measurement of the serum marker Ca 19-9 should not be used as an isolated screening test because of its relatively low negative predictive value. However, marked elevation of the Ca 19-9 level in association with a pancreatic mass is highly suggestive of pancreatic cancer.
Is specialist referral required?
Referral to a gastroenterologist is recommended if there is a high suspicion of pancreatic cancer, even if results of initial investigations are normal. The complexity of such cases usually warrants the involvement of an endocrinologist.
Conclusion
The vast majority of patients with diabetes are initially assessed and receive ongoing follow up in primary care. Recognising peculiar cases and investigating differential diagnoses accordingly is crucial, as appropriate and effective management depends on the underlying aetiology. Referral of complex cases to an endocrinologist, often as part of a multidisciplinary team, can assist in confirming the diagnosis and facilitating further treatment. ET
References
J Transplant 2018; 2018: 1025893.