Challenges in type 1 diabetes. Integrating emotional support into diabetes care

Diabetes type 1
Coping with chronic illness
People with type 1 diabetes often experience emotional distress and are more likely to have elevated depressive symptoms compared with those without diabetes. Healthcare professionals are ideally placed to provide support for people with diabetes, including when and how to assess and address common emotional problems. Acknowledging and normalising feelings of distress and continual assessment of people with diabetes are the cornerstones of emotional support.
- Type 1 diabetes is a demanding chronic condition associated with emotional challenges.
- Many people with type 1 diabetes may require psychological care, although this may not be overtly expressed.
- Health professionals have the capacity to identify emotional problems and provide support to people with type 1 diabetes as part of their regular consultation.
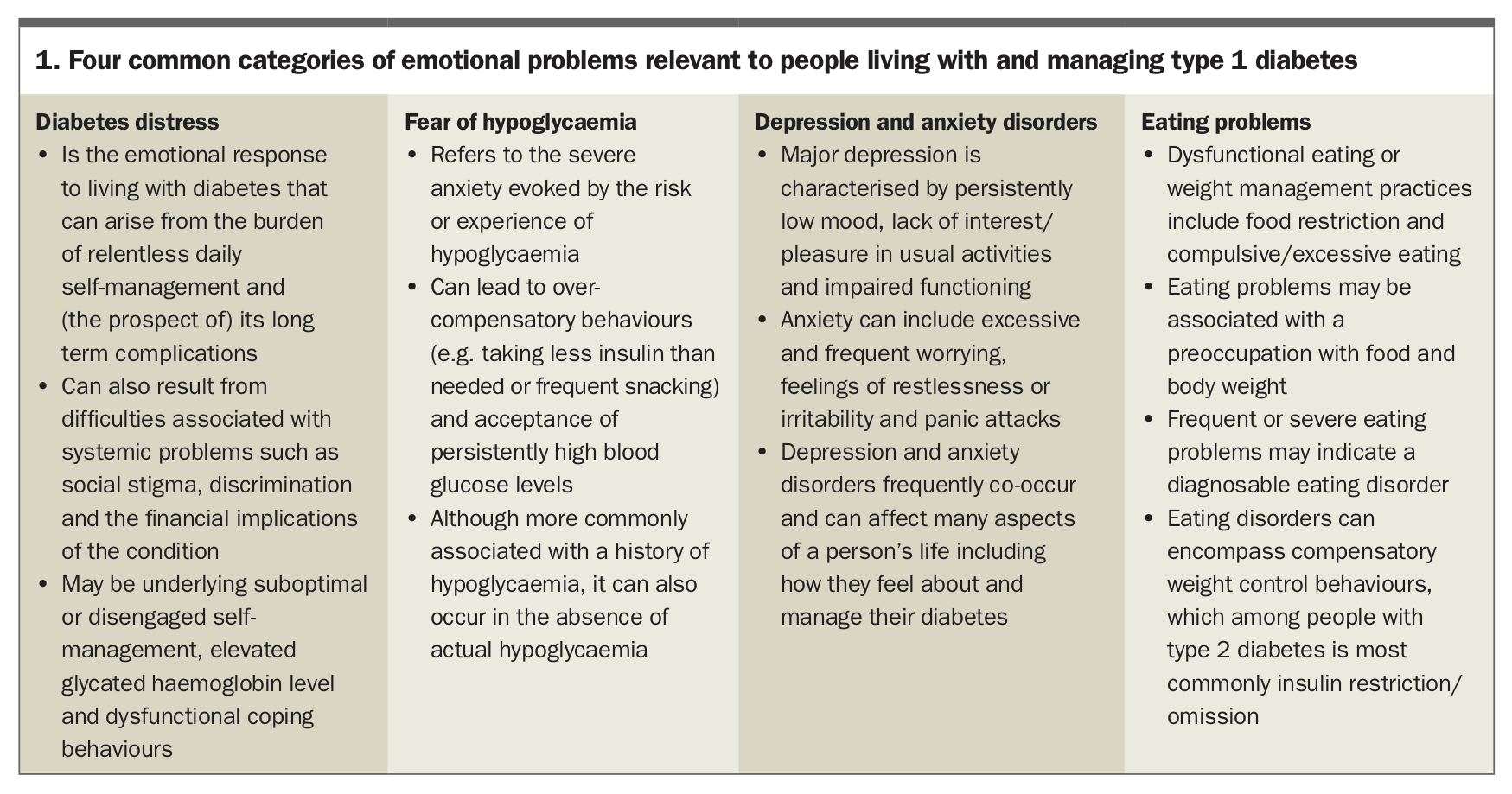
- Common emotional problems include diabetes distress, fear of hypoglycaemia, depression, anxiety and disordered eating.
- Identification involves being aware of common emotional problems, regularly asking people how they feel about living with and managing their diabetes, and conducting regular assessments (e.g. by using questionnaires such as the Problem Areas In Diabetes scale).
- Support involves providing information about the emotional problem (advising), developing an achievable action plan (assisting), providing a referral to another health professional if needed (assigning) and following up on progress (arranging).
What is the problem?
Emotional problems are common among people with type 1 diabetes. The prevalence of diabetes-related emotional distress (known as diabetes distress) is about 24 to 42% and the likelihood of elevated depressive symptoms is two to three times higher compared with people without diabetes.1-3 Although more research is needed to fully understand the causal links between diabetes and emotional problems, we know that living with type 1 diabetes entails a number of behavioural and psychosocial challenges.4 Self-management takes up a considerable amount of time, effort and motivation. On a daily basis, myriad calculations and decisions must be made and complex activities undertaken (glucose monitoring, insulin intake, physical activity and diet). No straightforward formula for managing diabetes exists and continual adjustments are often needed.
Self-management also comes with no guarantees of ‘textbook’ outcomes. Fluctuations in glucose levels in type 1 diabetes are common, sometimes unpredictable and may occur despite a person’s best efforts to maintain their glucose levels in target range. Understandably, the experience of glucose fluctuations can lead to frustration and concerns about future health. For some, it can accompany a feeling of powerlessness and disengagement from self-care.5 Moreover, diabetes-related stigma is widespread. Stigma, which is characterised by negative social judgement, exclusion, blame or devaluation, can precipitate or exacerbate isolation and negative self-judgement.6
Despite these challenges, most people with type 1 diabetes manage their emotional health well most of the time. But at times, distress may peak and impact on the person’s motivation, wellbeing and quality of life. There is growing evidence that diabetes distress is a predictor of reduced engagement in recommended self-management activities including reduced physical activity, unhealthy eating, suboptimal medication taking and less frequent glucose monitoring.4,7 Emotional problems are also associated with impaired quality of life, higher rates of complications, reduced functionality and overall mortality.8 Therefore, it is important to be alert to possible diabetes-related emotional difficulties.
How can health professionals support people with type 1 diabetes experiencing emotional problems?
Health professionals in general practice and diabetes specialist centres are ideally positioned to monitor and respond to emerging and existing emotional problems in people with type 1 diabetes. People with diabetes want to talk with their health professionals about how diabetes affects their mood and want health professionals to acknowledge the socioemotional aspects of diabetes management.9-11 Timely psychological care can lead to improved physical and emotional health.12 In particular, when health professionals show empathy and take an interest in psychological concerns, people report greater satisfaction with care and better health outcomes.13,14
Worldwide, diabetes guidelines recommend person-centred, holistic care, including regular psychological care. The Australian National Diabetes Strategy suggests regular mental health assessment (at diagnosis and as part of the annual cycle of care) and monitoring as important components of diabetes management.15 Research shows that health professionals are generally aware of the emotional burden of type 1 diabetes but they often restrict their care to medical management despite the abundant evidence that emotional problems are barriers to diabetes management.16,17
Some health professionals report that time limitations prohibit them from attending to emotional concerns during consultations. However, discussing emotional health can save time by engendering trust. It can also provide the health professional valuable information that could be relevant to ensuring effective clinical care is provided. Indeed, we know it is possible to integrate psychological care into diabetes care because many health professionals already do so within the available time of a regular consultation.18
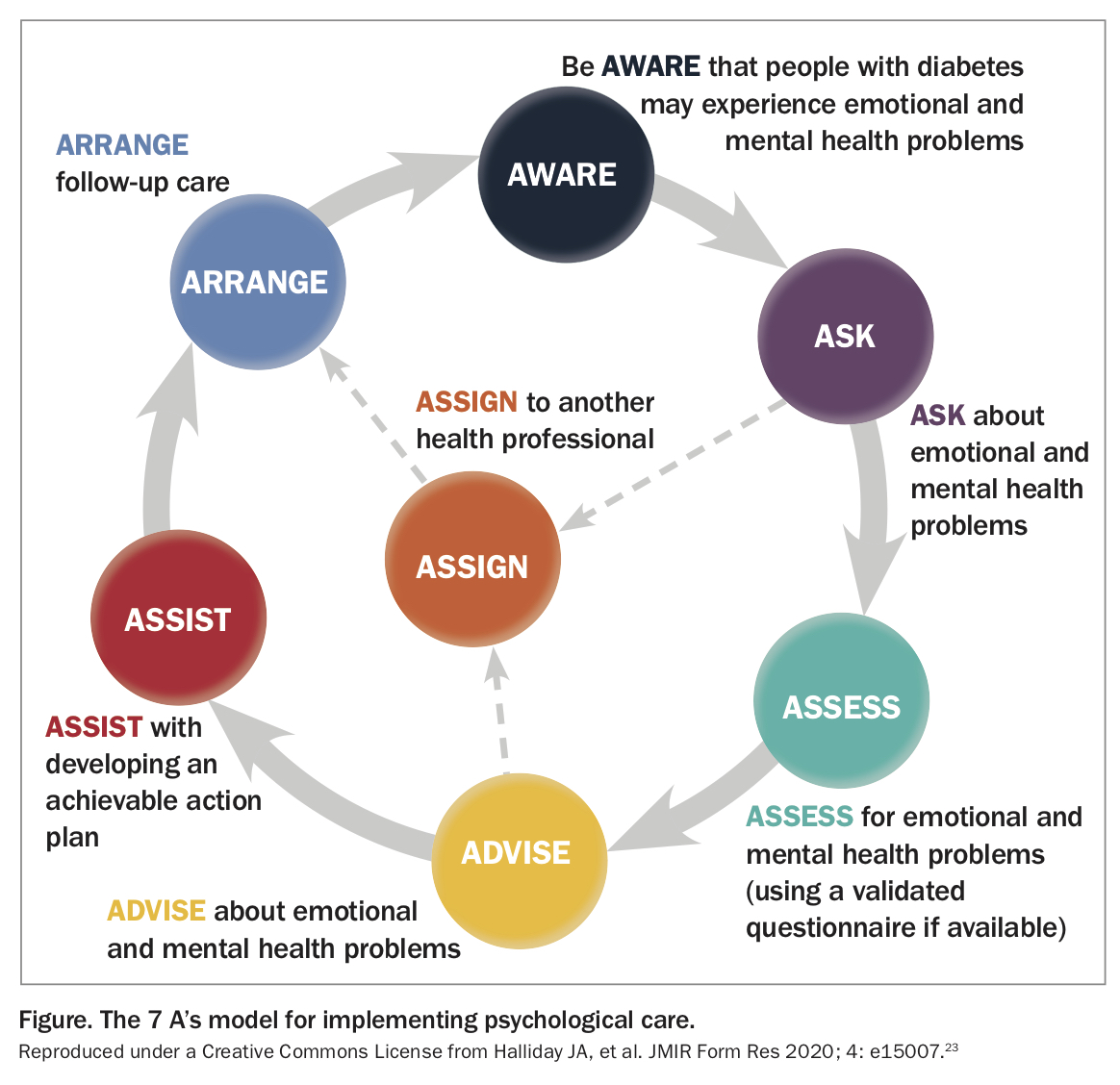
Health professionals have also reported a lack of training and skills to confidently attend to the emotional needs of people with diabetes. A small number of relevant clinical practice guides exist.19-22 Overall, they focus on two aims: (1) to assess for emotional problems, and (2) to provide psychological care. The National Diabetes Service Scheme’s (NDSS) Diabetes and Emotional Health: a practical guide for health professionals supporting adults with type 1 or type 2 diabetes provides a framework developed to elaborate on these aims (called the 7 A’s model, Figure).20 This practical guide is a free evidence-based and clinically informed resource for multidisciplinary diabetes health professionals.23
{kind=link}
How can health professionals identify emotional problems?
According to the 7 A’s model, there are three steps to identifying emotional problems in people with diabetes. The first step is to have awareness. Health professionals have an opportunity to enhance their diabetes consultations by being alert to possible emotional problems that a person with diabetes may be experiencing and that could be complicating their capacity for self-management or impairing their quality of life. Emotional problems can be diabetes-specific or generic. Four common emotional problems are summarised in Box 1. Distinguishing between these is critical as it can affect when, how and by whom psychological care is subsequently provided. For example, although diabetes distress and fear of hypoglycaemia can often be managed within regular diabetes consultations, when supporting a person with a mental health illness, a referral to a mental health professional may be warranted.
{kind=link}
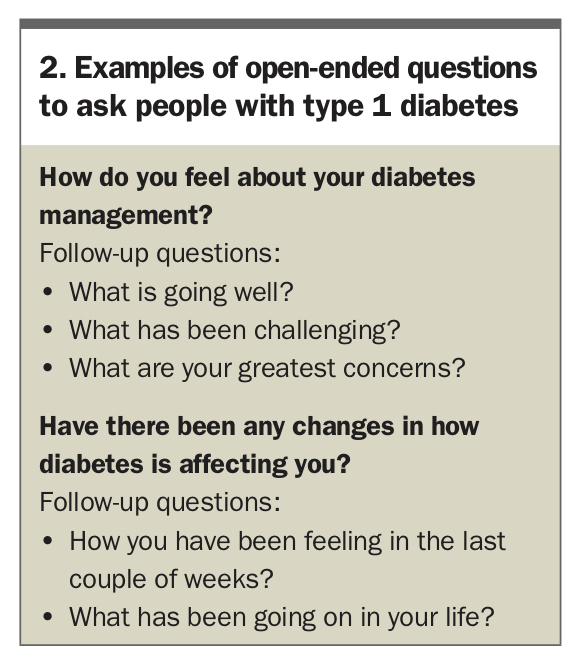
The second step in identification is to ask. Since emotional responses to living with diabetes can fluctuate over time, it is advisable to ask people about their emotional wellbeing at every consultation. An open-ended question (see Box 2 for examples) about the impact of diabetes on the person’s daily life can be a way of easing into a discussion about emotional health. Then, acknowledging and reflecting on feelings can affirm the consultation as a place for psychological care in conjunction with diabetes care.
{kind=link}
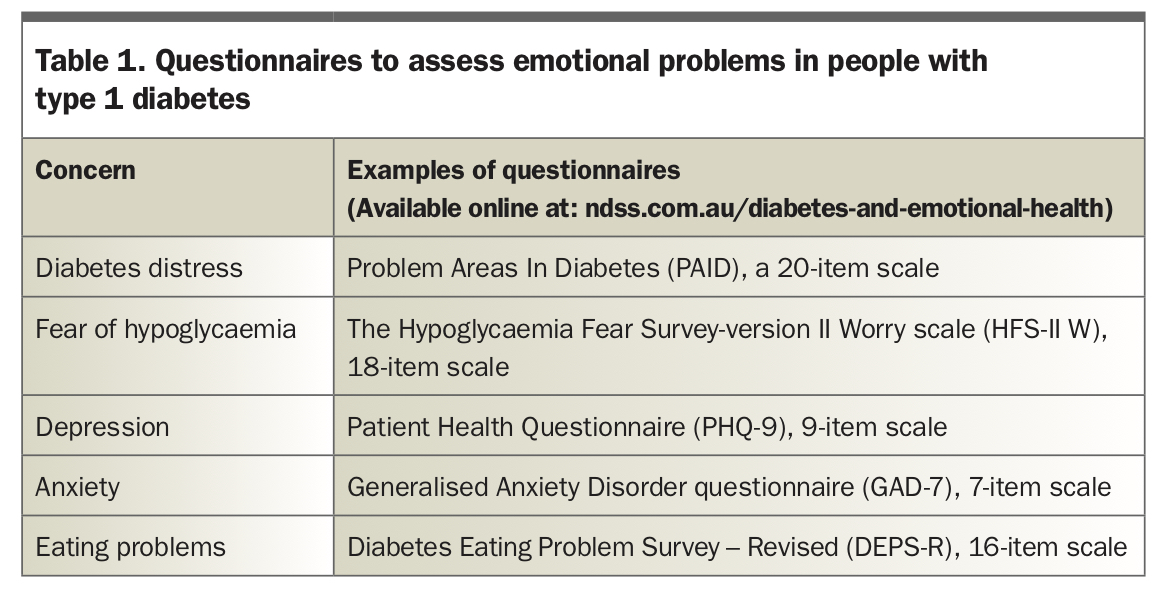
The third step in identification is to assess. In addition to asking people open-ended questions, regular systematic assessments can help ensure that problems are identified and monitored. Questionnaires can offer people with diabetes effective and pragmatic means of reporting their concerns, particularly those concerns that are difficult to voice Discussing questionnaire outcomes during the consultation is associated with greater patient satisfaction with consultations, reduced diabetes distress and improvements in glycated haemoglobin levels.16,24,25
Numerous well-validated questionnaires are freely available for assessing emotional health in people with type I diabetes (Table 1). Questionnaires about diabetes distress, in particular, can be useful as conversation starters and for converging the focus of a consultation to any challenges the person may be experiencing related to living with and managing diabetes.
{kind=link}
How can health professionals provide psychological care?
The first step to providing psychological care is to advise the person about any emotional problem or concern that has been identified. Any distress should be acknowledged and normalised. This can help the person feel heard, reduce their sense of isolation and aid trust and collaboration. Additionally, it can be empowering for the person to have a clear understanding of their emotional problem, including its associated symptoms. Sharing handouts (available through the National Diabetes Services Scheme, NDSS: ndss.com.au/mental-health) can be an effective and time-saving strategy for building on this discussion. As shown in a multinational trial, when the emotional problem is diabetes distress, an effective intervention can be as simple as conducting a psychological assessment and discussing the outcomes.16
As a next step, health professionals need to consider whether they can provide further support themselves or if another (mental) health professional needs to be involved. This will depend on the health professional’s qualifications, knowledge, skills and confidence; the severity of the emotional problem; and the needs and preferences of the person with diabetes. It is worthwhile bearing in mind that people with diabetes often report wanting emotional support from their regular diabetes health professional, illustrating the importance of integrative care no matter which course of action is decided.9,10
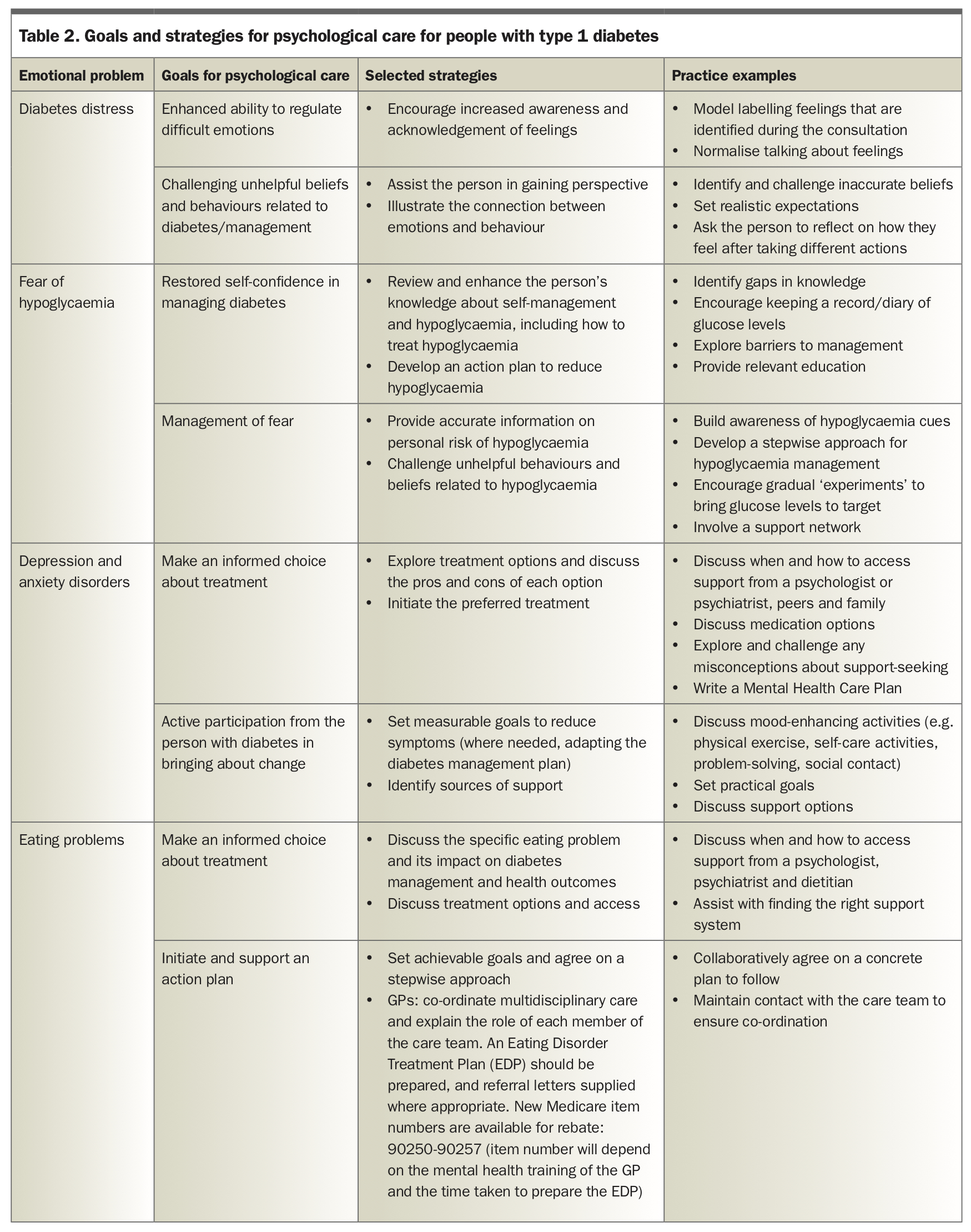
For health professionals, a number of strategies are available to incorporate psychological care into diabetes consultations (Table 2). For example, talking with the person about how they feel and what they believe about diabetes management can make a meaningful difference. This conversation allows opportunities to normalise feelings and to provide accurate information that challenges unhelpful beliefs. It can also lead to a practical discussion about problem solving.
{kind=link}
For severe and complex emotional problems (including diagnosable mental health illnesses), a referral to a mental health professional will be necessary (usually a psychiatrist or psychologist). Further information about when and how to make a referral is available in the NDSS factsheet Assisting people with diabetes to access professional psychological support: a practical guide for health professionals and the NDSS Diabetes and Emotional Health practical guide.20 If the person is not at immediate risk of harm to self, a conversation about accessing psychological support should take place. This starts by ascertaining the person’s preferences, their readiness to seek support and any barriers to accessing support. Opportunity should be taken to address any questions, concerns or misconceptions regarding when, why and how mental health support is accessed. Resources are available through the NDSS website to aid this conversation (ndss.com.au/mental-health).
Importantly, if the person is at immediate risk of harm to self, a referral to a crisis service or specialist inpatient service will be required. Risk of harm may be signalled by disclosures of suicidal ideation, recurrent episodes of diabetes ketoacidosis, cardiac arrhythmias, hypothermia, hypotension, electrolyte abnormalities, or if the person has stopped taking insulin.
The health professional’s role in psychological care does not end after referring the person with diabetes to another health professional or service. It is important to ensure that the referral has been received and accepted and, if there is a waiting list, then interim support (for example, through the health professional) is available if needed. Continued monitoring of emotional health and maintaining ongoing communication with the external health professional will help to ensure that co-ordinated and effective care is provided and, if needed, any adjustments are made.
Conclusion
Although this article offers several strategies for identifying and addressing emotional problems in diabetes care, the takeaway message is simple. What it comes down to is adopting a person-centred approach to communication and support. This means acknowledging and prioritising the person’s lived experience of diabetes as being central to the challenge of managing diabetes. Further reading and resources for health professionals can be found in Box 3. ET
{kind=link}
COMPETING INTERESTS: Dr Gray reports grants from Diabetes Australia (National Diabetes Services Scheme) to support her role at The Australian Centre for Behavioural Research in Diabetes. Dr Hendrieckx: None.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.