Bone health in type 2 diabetes. Managing fracture risk

Fractures
Diabetes type 2
Bone mineral density in people with type 2 diabetes is typically normal or even elevated; paradoxically, fracture risk is higher and post-fracture mortality in diabetes is further increased. The mechanisms and contributing factors to this are not well-defined but may include hyperglycaemia, increased risk of falls and certain diabetes medications. Antiosteoporotic medications are effective in managing fracture risk in those with type 2 diabetes and should be used to minimise the morbidity and mortality in this vulnerable group.
- People with diabetes are at increased risk of fracture despite normal or elevated bone mineral density (BMD).
- Contributing factors to increased fracture risk may include hyperglycaemia, increased risk of falls due to peripheral neuropathy or impaired vision and some diabetes medications.
- Mortality from fractures is higher for people with diabetes than those without diabetes.
- Although BMD scores may be normal or high on dual energy x-ray absorptiometry scanning, trabecular bone score (which measures bone microarchitecture) and cortical bone measurements on quantitative CT are lower.
- Use of fracture risk calculators may underestimate the true risk of fracture in people with diabetes.
- There should be a low threshold for measuring BMD in a patient with type 2 diabetes, and those with an osteopenic-range BMD (T-score between −2.5 and −1.0) may require active surveillance.
- Thiazolidinediones and possibly insulin and canagliflozin are associated with increased fractures, whereas metformin and liraglutide may be protective. The remaining current therapies appear to be neutral with respect to fracture risk.
- Despite lower bone turnover, antiresorptive agents remain effective in reducing fracture risk in those with diabetes.
Type 2 diabetes mellitus is a common condition worldwide, and is projected to further increase due to obesity and ageing. There is increasing evidence that diabetes is associated with bone fragility despite normal or above normal bone density (BMD), with higher risk of fracture, and elevated risk of mortality after a fragility fracture. Thus, bone health in this vulnerable group needs to be assessed and proactively managed. Understanding how bone health is affected in type 2 diabetes is paramount to identifying and appropriately managing high-risk patients.
Fracture risk in type 2 diabetes
Numerous meta-analyses have shown that both type 1 and type 2 diabetes are associated with increased risk of fractures.1-5 The risk appears to be greater in people with type 1 diabetes, especially at the hip (relative risk [RR], 6.3 to 6.94), with a trend towards increased risk of vertebral and nonvertebral fractures. Type 2 diabetes is associated with a modest increase in the risk of hip (RR, 1.3 to 2.1) and all fractures (RR, 1.2), particularly distal lower limb, and no difference in risk of vertebral fractures.2-5 Differences in the observed risk for vertebral fractures in type 2 diabetes are in part due to ascertainment bias of clinical (i.e. symptomatic) versus morphometric (i.e. asymptomatic vertebral deformities detected only on radiology) fractures in studies using different methodologies.6 It is also unclear whether increased vertebral fracture risk is observed only in women with type 2 diabetes or is present in both sexes – smaller sample sizes of men in some studies could underestimate this effect in men.2,4,7,8
Although the fracture risk, especially for hip fractures, appears to be increased in people with type 2 diabetes, the contributing mechanisms remain unclear due to multiple confounders. It is postulated that the cumulative exposure to hyperglycaemia (both in duration and degree) and/or vascular complications may contribute to poor bone quality. Studies have found an increased risk of fractures only in people with longer duration of type 2 diabetes, and a reduction in fractures in those with early diabetes or dysglycaemia,9-12 although this finding is inconsistent.7,8,13 Cohort and observational studies suggest that participants treated with insulin or other diabetes medication had an increased fracture risk compared with those managed with diet alone.11,14-16 However, in the absence of prospective studies, it is difficult to separate medication bias (the underlying clinical choices dictating a patient’s treatment regimen) from independent effects of the medications per se.
Finally, increased fracture risk has been associated with microvascular diabetic complications.10,15,17 It remains to be determined whether hyperglycaemia directly affects bone fragility, or if it is the sequelae from nonskeletal complications (such as impaired vision, proprioception and frequent falls due to retinopathy or peripheral neuropathy) that increase fracture risk. Studies have not shown a consistent correlation between fracture risk and glycaemic control (as measured by either fasting glucose or glycated haemoglobin [HbA1c] levels), which is associated with the development of microvascular complications.10,18-20 Further, a recent prospective cohort study found that frailty, based on comorbidities and functional testing, increased the risk of fracture in people with diabetes, suggesting that functional impairment does contribute, at least in part, to fracture risk.21
Importantly, irrespective of the mechanism, each fragility fracture is associated with increased mortality and substantially higher post-fracture mortality in those with type 2 diabetes and aged under 70 years compared with those without diabetes.22-25 Therefore, the cumulative burden from fractures in this vulnerable group is high and at-risk patients should be identified early.
Pathophysiology of bone disease in type 2 diabetes
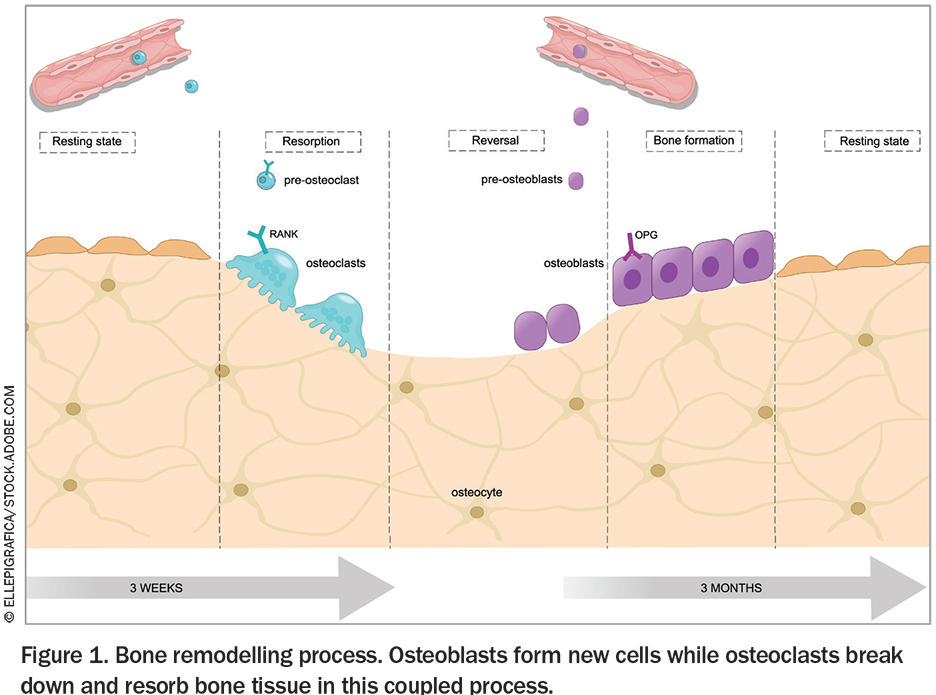
Bone undergoes continual remodelling to repair microfractures and allow for the flux of ions and minerals into the systemic circulation. Under normal circumstances, remodelling is a coupled process, between osteoblasts (bone-forming cells) and osteoclasts (bone-resorbing cells), as shown in Figure 1. Conditions where bone turnover is either high or low are associated with microarchitectural deficits and may independently predict fracture risk.26
{kind=link}
Type 2 diabetes is likely a low bone turnover state, which may therefore contribute to less bone loss and increased BMD, but worse microarchitecture and impaired bone strength, resulting in increased fracture risk; the association is complex and the underlying pathophysiology is not well established.
Bone turnover is reduced
Two meta-analyses suggest that type 2 diabetes is associated with reduced bone turnover markers (BTMs), with measured reductions in bone resorption (most consistently collagen type 1 C-terminal telopeptide and N-terminal telopeptide) and bone formation (osteocalcin and procollagen type 1 N-terminal propeptide).27,28 The degree of hyperglycaemia appears to contribute to this low bone turnover state, although there are numerous confounders in the studies.
Bone mineral density is unchanged or increased
BMD is paradoxically normal or even elevated in people with type 2 diabetes and is likely related to the increased body mass index that often co-occurs.4,5,29,30 There is variability as to whether age, sex, duration of diabetes and glycaemic control are associated with BMD.5,29 Despite normal or higher BMD, the association of type 2 diabetes with lower bone turnover is independent of adiposity, suggesting a complex interplay between type 2 diabetes, hyperglycaemia, BMD and fracture risk.31,32
Bone microarchitecture is worse
Despite higher BMD, there is evidence that type 2 diabetes is associated with poorer measures of bone strength and microarchitecture. Bone can be classified as either trabecular or cortical, according to the porosity and microstructure. Trabecular (or cancellous) bone is highly porous and has a high surface area and is therefore the site for most of the metabolic activity of bone such as exchange of ions and haematopoiesis. It is highly flexible in nature and is found at the end of long bones, vertebrae and flat bones such as the pelvis. Cortical bone is denser and contributes to load bearing and protection of underlying organs. It is found in the shaft of the long bones and forms the outer shell around trabecular bone at other sites. A dual energy x-ray absorptiometry (DXA) scan, which is the standard method for determining BMD, does not measure these components separately, but there are other imaging modalities that do.
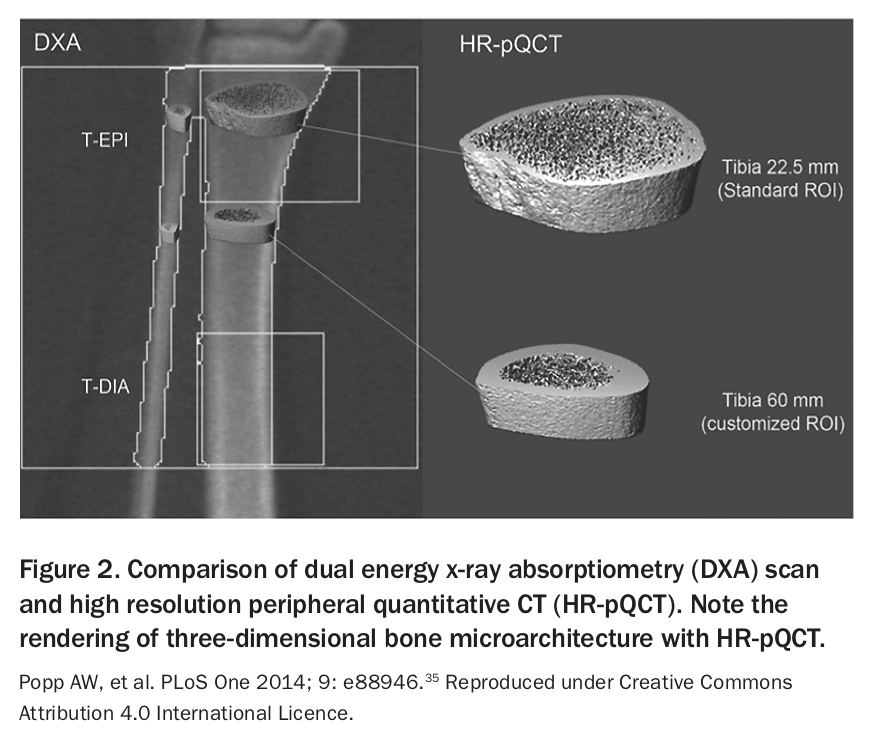
Trabecular bone score (TBS) aims to quantify the trabecular compartment of vertebrae by using pixel grey-level variations in a spine DXA image to provide information on microarchitecture and fracture risk, independent of BMD. Two cross-sectional studies found lower spine TBS but higher BMD in patients with type 2 diabetes and a negative correlation between TBS and HbA1c.33,34 Type 2 diabetes is also associated with impaired cortical parameters, particularly higher cortical porosity, with preserved trabecular indices when using high resolution peripheral quantitative CT (HR-pQCT) of the distal radius and tibia to assess three- dimensional bone microarchitecture (Figure 235).36 A small study found that fasting glucose levels (but not duration of type 2 diabetes or insulin resistance) were associated with lower cortical volumes.37 Some studies have found cortical deficits in only a subset of people with type 2 diabetes (e.g. with fracture or with microvascular disease).38,39 Together, the HR-pQCT data suggest that type 2 diabetes is associated with cortical deficits that impair bone strength, which may relate to the increased fracture risk despite higher BMD.
{kind=link}
Fracture-risk prediction in type 2 diabetes
Since BMD is elevated in type 2 diabetes, current fracture risk calculators such as the Fracture Risk Algorithm (FRAX) (https://www.sheffield.ac.uk/FRAX) or the Garvan Fracture Risk Calculator (https://www.garvan.org.au/promotions/bone-fracture-risk/calculator) can be unreliable in quantifying fracture risk in people with type 2 diabetes. These patients experience higher fracture risk for a given BMD, age or FRAX score compared with those without type 2 diabetes.40 The hip-fracture risk in an individual with type 2 diabetes was equivalent to a gender-matched counterpart without type 2 diabetes, with a T-score 0.4 to 0.6 lower.40
Adjusting fracture risk algorithms to partially explain fracture risk in type 2 diabetes may provide a more accurate prediction of a patient’s fracture risk. Methods for adjustment include reducing the T-score by 0.5, increasing the patient’s age by 10 years, including rheumatoid arthritis as a comorbidity (as a surrogate for type 2 diabetes) and adding TBS adjustments.41
Fracture risk in type 2 diabetes is poorly understood and is underestimated using current prediction algorithms; however, measuring BMD remains helpful in predicting fracture risk, especially if it is low. Type 2 diabetes is not listed as a secondary cause of fracture for Medicare reimbursement of BMD scanning and there are no definitive guidelines on clinical risk factors for fracture in type 2 diabetes. Therefore, there should be a low threshold for measuring BMD in a patient with type 2 diabetes, and those with an osteopenic-range BMD (T-score between −2.5 and −0.1) may require active surveillance.
Effect of type 2 diabetes medications on bone
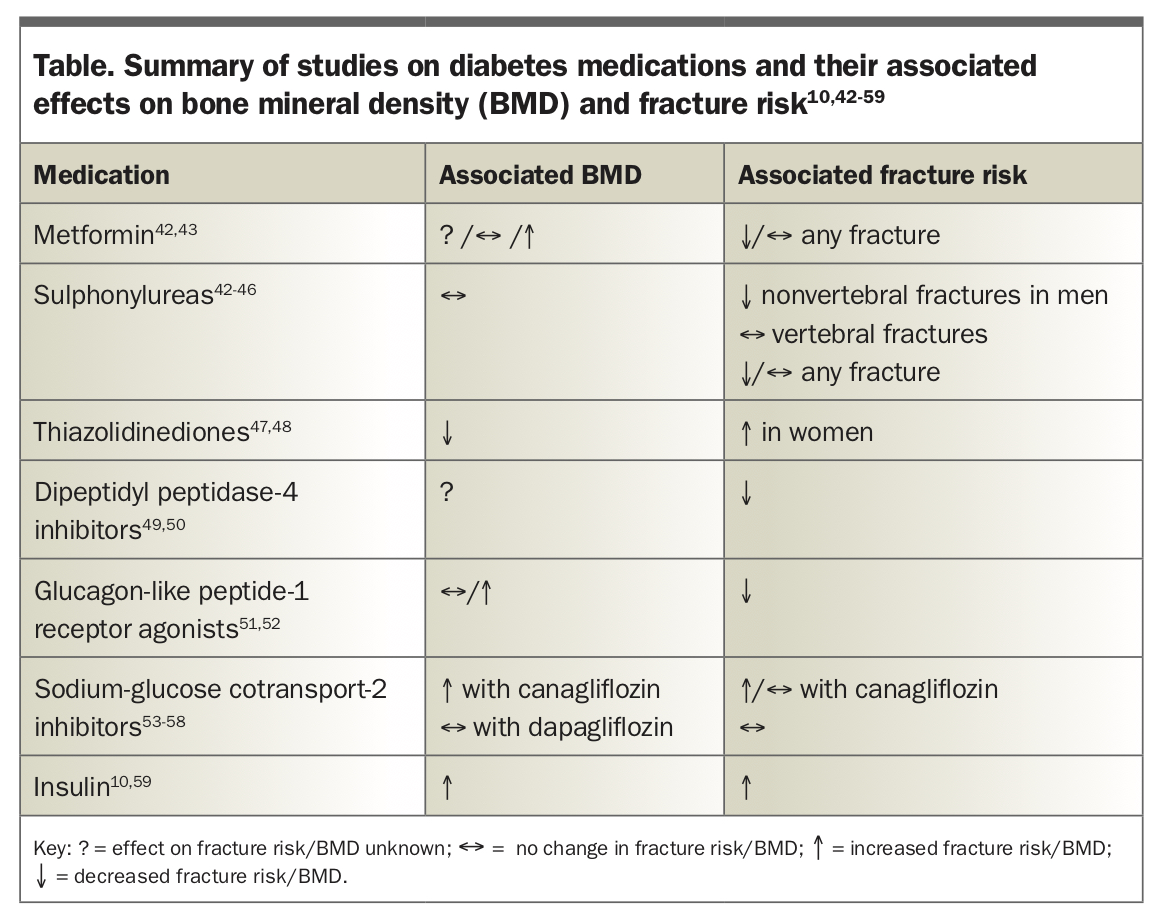
Meta-analyses of clinical trials and observational studies provide some data on the effect of diabetes medications on BMD and fracture risk in people with type 2 diabetes (Table).10,42-59 Overall, thiazolidinediones, and possibly insulin and canagliflozin (a sodium-glucose cotransporter-2 inhibitor), are associated with increased fractures, whereas metformin and liraglutide (a glucagon-like peptide-1 receptor agonist) may be protective. The remaining current therapies (sulfonylureas, dipeptidyl peptidase-4 inhibitors and other sodium-glucose cotransporter-2 inhibitors) appear to be neutral with respect to fracture risk. Therefore, thiazolidinediones should be used with caution in those with a previous fracture, low BMD or high falls risk. Risk of falls secondary to hypoglycaemia should also be carefully considered when choosing diabetes medications.
{kind=link}
Bone management in type 2 diabetes
Given that type 2 diabetes is a low bone turnover state, there are theoretical concerns about the efficacy and safety of antiresorptive agents in patients with type 2 diabetes. There have been no randomised clinical trials directly evaluating the efficacy of anti-osteoporotic medications in type 2 diabetes; however, post-hoc and subgroup analyses of major trials have shown no difference in efficacy between people with and without type 2 diabetes.
Alendronate use in women in the Fracture Intervention Trial was associated with similar increases in BMD at all sites in those with type 2 diabetes compared with those without diabetes.60 In a Danish prescription registry cohort study, there was no difference in antifracture efficacy of alendronate or etidronate for all fracture types in those with type 2 diabetes.61 A post-hoc analysis of three phase III Japanese trials of risedronate found that BTMs were slightly lower in participants with type 2 diabetes compared with those without, but there were no significant differences in BTM suppression or BMD gain in response to risedronate use between both groups.62 In a recent post-hoc analysis of Fracture REduction Evaluation of Denosumab in Osteoporosis every 6 Months (FREEDOM) and 7-year extension trials, denosumab in type 2 diabetes resulted in higher BMD and reduction in vertebral fractures compared with placebo.63 Subgroup analyses of the Multiple Outcomes of Raloxifene Evaluation (MORE) trial and Raloxifene Use for The Heart (RUTH) trial found that raloxifene was associated with a similar reduction in vertebral fractures in participants with and without type 2 diabetes.64,65 A similar reduction in hip and forearm fractures was also observed in the Danish registry study.61
Teriparatide is the only bone-anabolic agent currently listed on the PBS in Australia. In a post-hoc analysis of the observational Direct Analysis of Non-vertebral Fractures in the Community Experience (DANCE) study, teriparatide (20 mcg daily subcutaneously for up to 24 months) was associated with similar increases in spine and total hip BMD, greater increases in femoral neck BMD and similar reduction in nonvertebral fractures in people with type 2 diabetes compared with those without.66
The currently available antiosteoporosis medications in Australia appear to be efficacious and safe in people with type 2 diabetes. Additional considerations for therapy choice include renal function (especially for bisphosphonates), medication burden and/or adherence and frequent concomitant vitamin D insufficiency. Issues that remain unanswered include whether intravenous bisphosphonates (e.g. zoledronic acid) have similar efficacy in type 2 diabetes, whether antiosteoporotic treatments have similar fracture benefit and safety (especially long term) in those without osteoporotic BMD (given that type 2 diabetes is associated with higher BMD), if there are changes on bone histomorphometry (given the microarchitecture differences in type 2 diabetes) and the effects of new anabolic agents (e.g. romosozumab).
Conclusion
People with type 2 diabetes have a specific fracture-risk profile, with a higher fracture risk despite increased BMD, and high post-fracture mortality. The underlying mechanisms are not yet defined but may relate to reduced bone quality and turnover, and microarchitecture changes. Contributing factors may include severity of disease and disease-related complications or falls, sex and concurrent use of certain medications such as insulin and thiazolidinediones. Antiosteoporotic medications are effective in reducing fracture risk in people with type 2 diabetes and should be used to minimise the morbidity and mortality associated with fragility fractures in this vulnerable group. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.