Diabetes and mental illness: optimising care

Diabetes type 2
Diabetes and serious mental illness (SMI) account for a considerable proportion of premature mortality. It is important that GPs are aware of the association between diabetes and SMI, particularly in young people, and manage patients with either or both conditions appropriately, by regular screening for potential comorbidities and involving a team of healthcare professionals to optimise patient outcomes.
- There is a clear association between serious mental illness (SMI) and type 2 diabetes in younger populations. It is therefore important to assess younger patients with SMI for hyperglycaemia and be alert to the symptoms of depressive and anxiety disorders in those with diabetes, even if other disorders (such as psychotic disorders) are present.
- Patients with SMI and hyperglycaemia are considered high risk for premature mortality, and should be regularly screened for comorbidities and managed appropriately.
- Establishing a shared care-co-ordination arrangement with a local health district mental health services, non-Governmental organisation or an identified carer, and simplifying or minimising prescriptions can help support patients adhere to treatment regimens.
- Patients with SMI are at high risk of diabetes and cardiometabolic disorders and frequent screening is encouraged for early detection and intervention.
- Obstructive sleep apnoea is a common comorbidity in people with SMI and should be screened for regularly as it may worsen risks for both diabetes and mental health stability.
- The orexigenic nature of some psychotropic drugs can contribute to weight gain. Drug regimens should be reviewed and orexigenic drugs replaced where feasible, especially in cases of polypharmacy.
Diabetes and serious mental illness (SMI) account for a considerable proportion of present and projected chronic illness burden and premature mortality. There is growing evidence for an association between SMI and type 2 diabetes in younger populations, with an increased risk of comorbidities including cardiovascular disease (CVD), sleep disorders and premature death. This article considers some applicable learnings from a multidisciplinary integrated health perspective that may assist in achieving better outcomes.
Diabetes and serious mental illness
Serious mental illness (SMI), defined here as enduring and diagnosable mental illness such as schizophrenia, bipolar disorder, other relapsing psychotic conditions and severe unipolar depression, occurs in about 4 to 5% of the Australian population. Diabetes occurs in about 8% of the population and prediabetes in up to 17% of the population (although this is somewhat dependent on the survey cited).1 Based on the central Sydney population, for people with SMI, the overall risk of diabetes is three times that of the general population (24% vs 8%, respectively).2 Rates of prediabetes in people with SMI (as determined by impaired fasting glucose) are also higher than in the general population.
In people with SMI, the relative risk compared with age- and gender-matched population data suggests that younger people may be 10 times more likely to develop hyperglycaemia, with the ratio only approaching unity from age 60 years. Conversely, those with young onset type 2 diabetes (aged under 40 years) are more likely to develop mental illness and experience more hospitalisations.3 The strong association between diabetes and high prevalence disorders such as depression and anxiety remains clear, with evidence for the attribution of bidirectional causality steadily accumulating.4,5
A related concept is that of ‘diabetes distress’, which has been proposed as a moderator between depression and glycaemic control.6 The two conditions covary and may share some aetiological determinants but are not interchangeable.7 Up to 40% of people with type 1 diabetes may experience diabetes distress (Twigg, S. Pers comm). As depressive/ distress symptoms increase, the ability to self-manage diet and prescribed treatments decreases and functional impairments increase.8 The association between diabetes and SMI may also be intergenerational, which may be due to shared genetic risks, environmental factors, or both. Up to 55% of patients with SMI report a family history of diabetes and, at least for nonaffective psychoses, there is an increased family history risk of diabetes.9
TIP: In young people with SMI, even those in their 20s, screen regularly for hyperglycaemia.
TIP: In people with diabetes, observe carefully for the early development of symptoms of depressive and anxiety disorders.
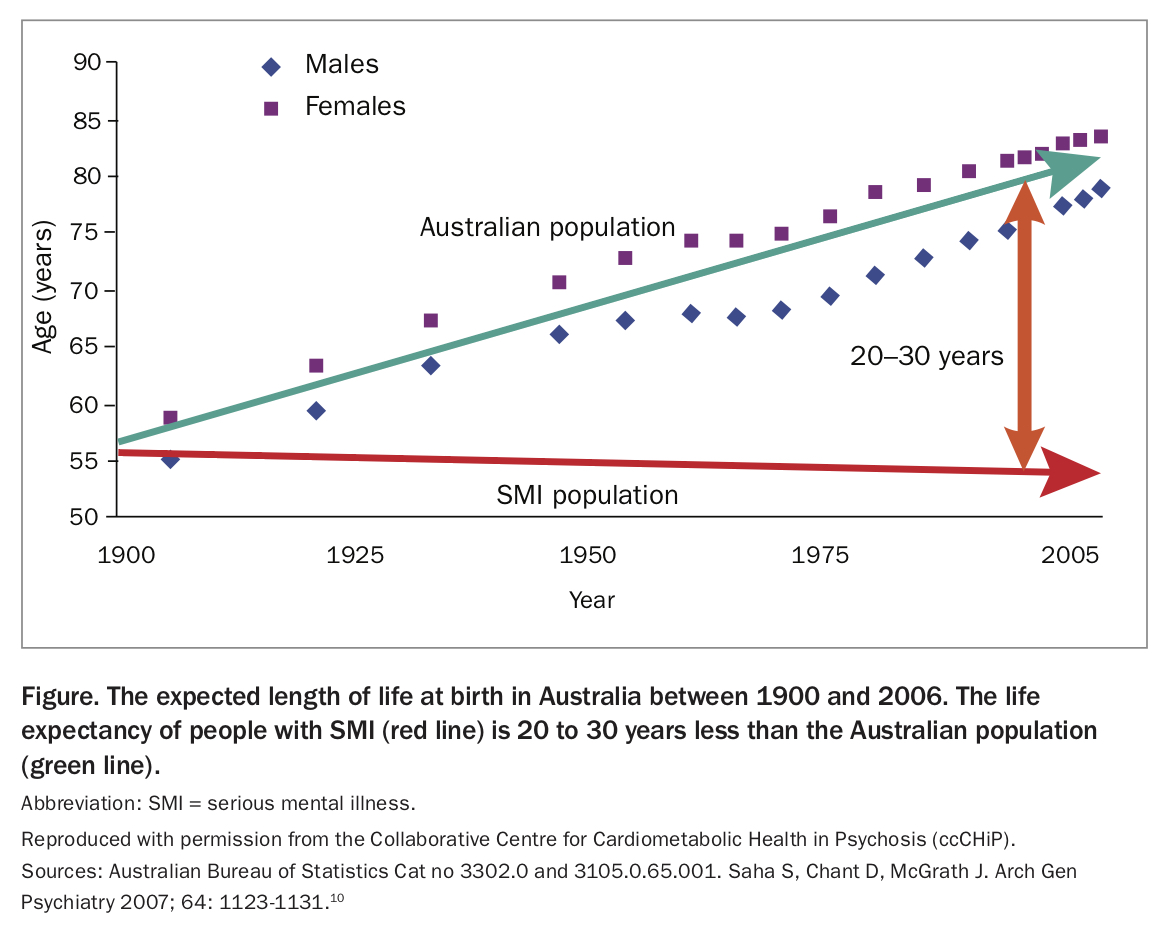
Premature mortality
It is widely accepted that patients with SMI lose between 20 and 30 years of life (Figure), mainly because of cardiometabolic disease.10 The most common underlying causes of death for people with diabetes are heart disease, cancer and stroke. Premature mortality (dying younger than 75 years of age) due to type 2 diabetes is likely underestimated in those with SMI.11 Furthermore, it has been found that in people with comorbid depression, premature mortality rates are increased beyond that apportioned to CVD.12 Over the past decades it has become clear that patients with SMI rarely achieve parity in receiving general medical care.13
{kind=link}
TIP: A priori, treat all patients with SMI and hyperglycaemia as high risk for premature mortality, and screen and manage assiduously.
Attendance and follow up
The poor cardiometabolic outcomes for people with SMI are often attributed to their unreliable attendance. Although this can be true for all patients from time to time, we have found that, once engaged, patients with SMI are very willing to work collaboratively on improving their physical health.
The issue of low attendance mainly revolves around the process of getting to the appointment rather than not wanting to participate. Deficit symptoms (primary to the illness) and secondary phenomena such as neurological, musculoskeletal and cognitive side effects conspire to make it hard for the patient to remember the appointment and plan it out in their daily schedule. Sending text reminders to smart phones enhances attendance, but one of the most compelling way to enhance attendance is to establish a shared care-coordination arrangement with the local health district mental health service, non-Governmental organisation or identified carer. At the outset of any such relationship, establishing an agreement regarding transport arrangements will produce mutual benefits. As noted above, once at the appointment, the patient is often interested in understanding their physical health status and which remedies are necessary.
TIP: Set up an agreement regarding transport and attendance protocols with the patient, carer or support worker from the outset.
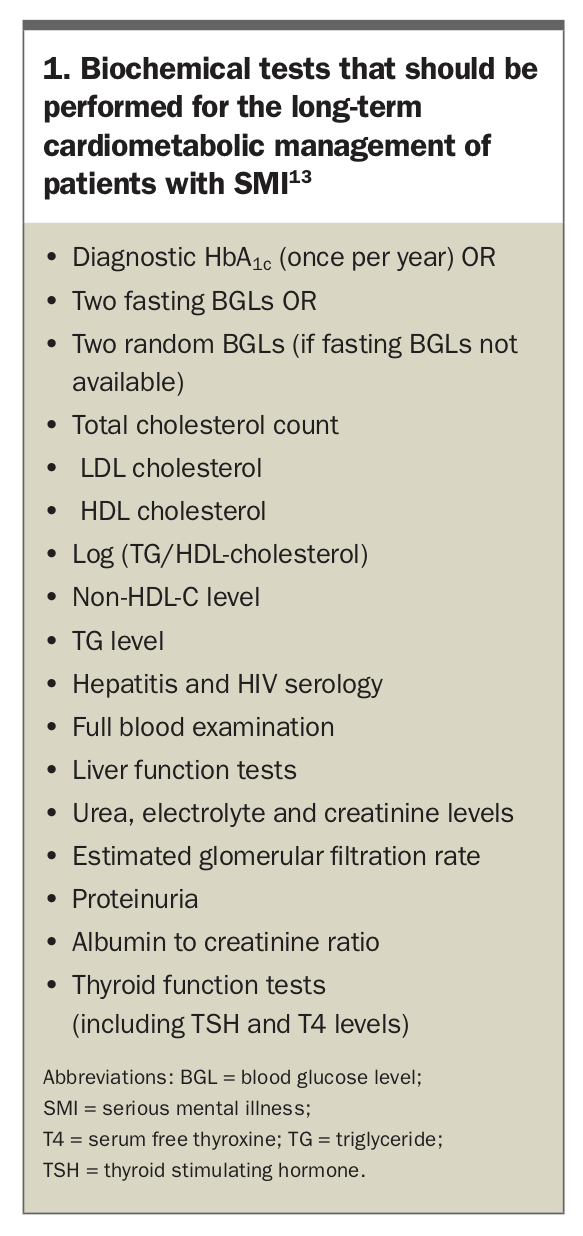
Which tests, and when?
When managing the long-term cardiometabolic care of people with SMI, the recent Royal Australian and New Zealand College of Psychiatrists (RANZCP) consensus statement outlines the range of tests that should be regularly performed (Box 1).14 We suggest six-monthly reviews until a therapeutic relationship is established between the patient and their clinician (e.g. medical psychiatrist in multidisciplinary teams, GP in community practice), and target health behaviours are formulated and practical to incorporate into the patient’s routine. Once agreed health behaviour patterns are stable, complete physical health comorbidity reviews should be undertaken 12-monthly, with flexible arrangements to accommodate changes in the patient’s circumstance that might affect risk.
{kind=link}
Given the early age of onset of hyperglycaemia, an annual diagnostic review of HbA1c is encouraged. As this is a somewhat recent development, many GPs are reluctant to use this test. Annual diagnostic reviews of HbA1c are approved and reasonable, considering the relatively higher incidence of new cases of hyperglycaemia in the younger patients with SMI. However, all relevant screening tests should be undertaken, especially a full lipid examination, as dyslipidaemia is an early and robust indicator of later risk of CVD in type 2 diabetes. In the general population, 50% of patients have either microvascular or macrovascular complications at the time of first diagnosis of diabetes.15 Given the longer lag times before a diagnosis of diabetes in people with SMI, these complications may be more frequent. Early detection and intervention are crucial.
Micro- and macrovascular complications: annual cycle of care
The notion of the ‘annual cycle of care’ is built on the sound principle of detecting diabetes-related micro- and macrovascular complications as early as possible. Although more patients with SMI are attending their vision checks because of the availability of optometrists at shopping centres, the examination of the lower limbs and renal function are less commonly performed. Patients with SMI may require extra explanation and support in understanding the reasons for providing a urine sample, and why they should have their lower limbs and feet checked regularly.
TIP: Patients with SMI are in a high-risk cardiometabolic group. Order pathology screening tests frequently to pick up early cases, and to undertake early (pre)diabetes intervention.
TIP: Work with patients with SMI to overcome their reluctance to complete the annual cycle of care.
Sleep disordered breathing
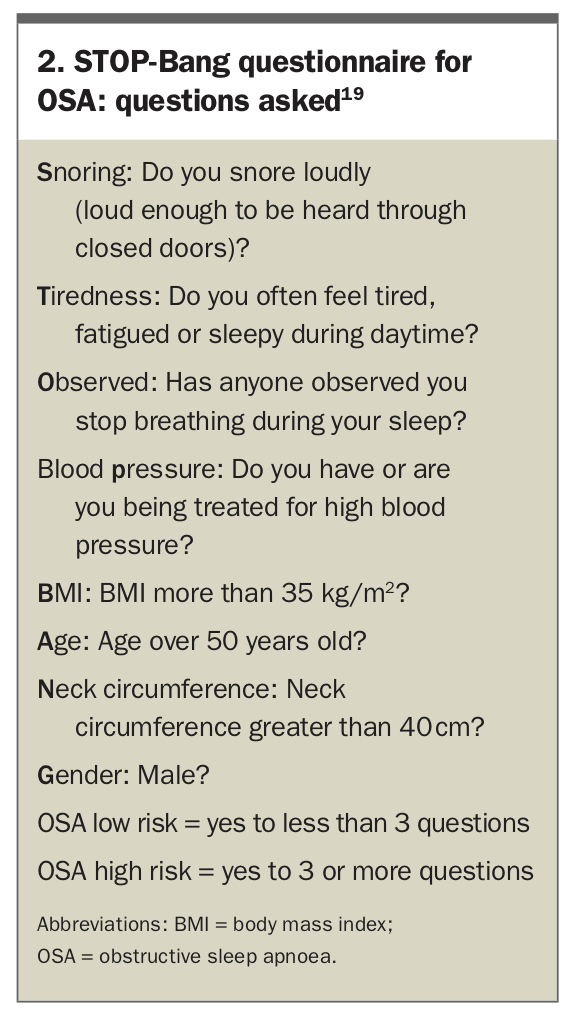
Obstructive sleep apnoea (OSA) is a frequent comorbidity in people with SMI. In an overweight cohort of people with schizophrenia, the prevalence of sleep apnoea was over 60% and undiagnosed OSA rates in obese patients with diabetes were as high as 87%.16 OSA severity has been linked to increased chances of developing type 2 diabetes de novo, and for patients with pre-existing diabetes, OSA is likely to worsen diabetes control.17,18
Because of the high prevalence of OSA in patients with SMI, we recommend screening for possible cases using a simple tool such as the STOP-Bang questionnaire (available at: www.stopbang.ca/osa/screening. php) (Box 2).19 If available, threshold cases can be further assessed using a simple home pulse oximetry device. Analysis of this data can then allow an assessment of whether a polysomnography sleep study or direct provision of continuous positive airway pressure therapy should be considered. Such a decision will usually require referral of the patient to a sleep specialist or specialist clinical service. Of note, severe OSA can mimic and actually worsen the deficit symptoms of schizophrenia, worsen cognitive function and increase the risk of sudden death, independent of the effects of OSA on diabetes and subsequent CVD.
{kind=link}
TIP: Detecting and dealing with OSA is a key component of diabetes management in patients with SMI.
Adherence to treatment
A common health myth is that people with mental illness will not be able to adequately maintain fidelity to agreed treatment plans for somatic health treatments, including oral diabetes medication. A recent systematic review of six studies examined adherence to diabetes medication in people with schizophrenia. Two of the studies found that patients with schizophrenia had higher rates of adherence to their diabetes medication than those without schizophrenia. However, many patients with schizophrenia were not adhering to their diabetes medications, as the overall adherence rate ranged from 51 to 85%.20 Although these figures are comparable to a general diabetes cohort,21 the psychiatric studies used a predominantly middle-aged male cohort, and more work is required to understand issues in younger patients. Although beyond the scope of this article, understanding a patient’s adherence issues through the lens of modern adaptations of the Health Belief Model is of considerable practical utility.22
A robust predictor of compromised treatment fidelity is the number of tablets required per day and the complexity of the regimen. This is a particular problem for patients with SMI due to polypsychotropic prescribing, and compounded by having multiple prescriptions to manage the highly prevalent medical comorbidities such as diabetes, dyslipidaemia and hypertension.
TIP: Review the number of agents prescribed and the complexity of the regimen. Simplify or minimise where feasible. Consider obtaining psychopharmacology advice.
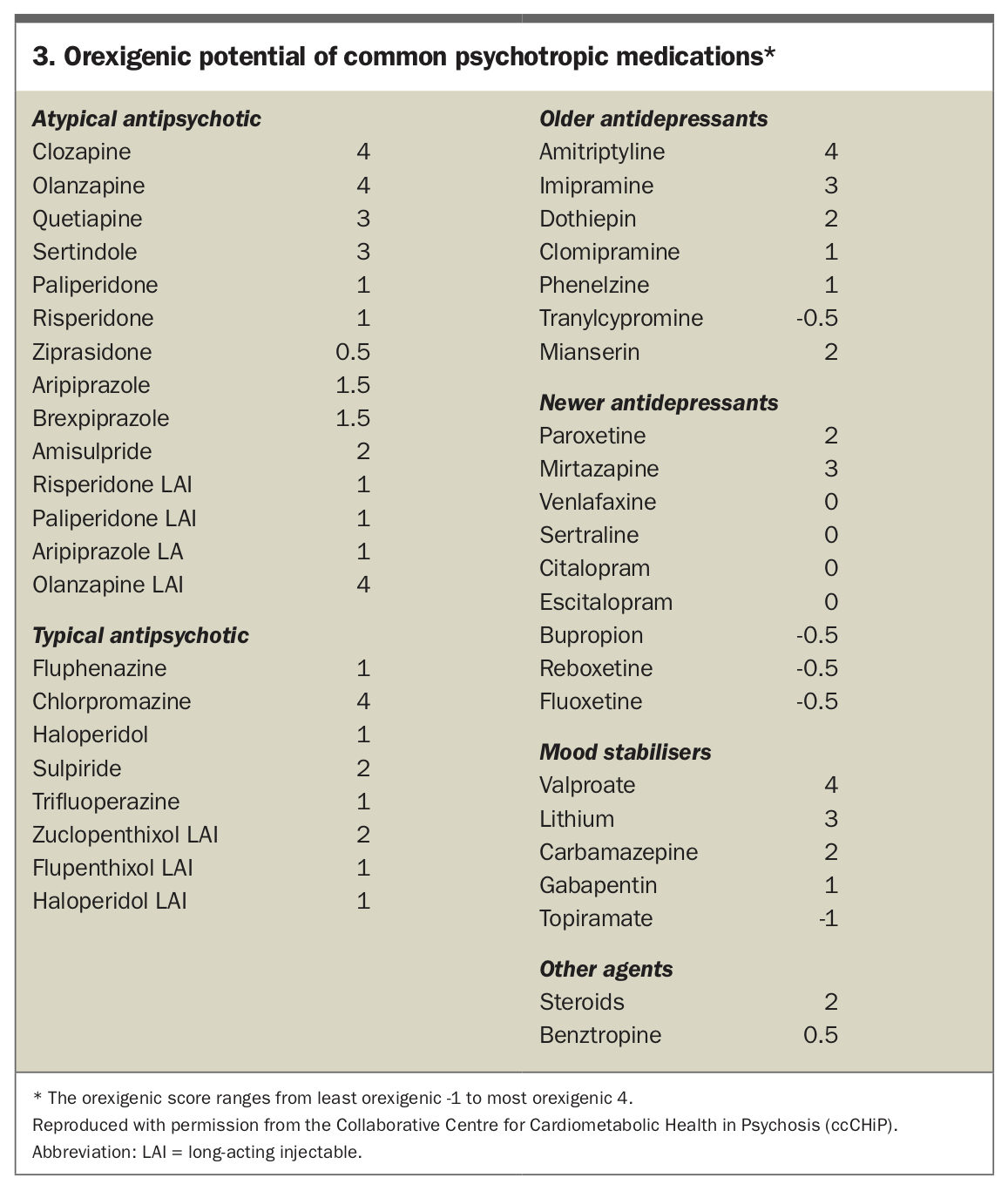
Psychotropic polypharmacy
Often newer antipsychotics are (erroneously) singled out as the cause of diabetes and other cardiometabolic problems in patients with SMI. Although relatively higher rates of diabetes were seen in people with SMI before the advent of psychotropics in the 1950s, there is little doubt that some commonly used agents increase its incidence. In cases where diabetes is associated with the use of second-generation antipsychotics, it has been proposed that the major impact is secondary to weight gain.23 There is evidence that clozapine, but not quetiapine, olanzapine or risperidone, may have a direct effect on insulin dynamics, independent of weight gain.24 Psychotropics other than antipsychotics may be particularly orexigenic (Box 3), and the unfortunate tendency to psychotropic polypharmacy with such agents drives appetite and subsequent diabesity in a genetically vulnerable group.25
{kind=link}
Polypharmacy often derives from more than one prescriber actively providing prescriptions – a common scenario in patients with SMI who are managed by community mental health teams independent of their GP. Public patients often remain on discharge medications after hospitalisation without subsequent reassessment and medication rationalisation suitable for the maintenance phase of their illness. Medications should therefore be carefully reviewed and those that are orexigenic with little evidence base to support their use (e.g. valproate in schizophrenia), should be removed or switched to less orexigenic alternatives, if clinically feasible. Drug–drug interactions are also a source of metabolic problems in some situations, made more likely through polypharmacy.
TIP: Undertake a review of the necessity of all individual prescriptions, especially when dealing with orexigenic polypsychotropic prescribing.
A co-ordinated approach to patient care
Where possible, shared decision-making in the management of SMI is preferable and should include input from a team and/or network of linked healthcare professionals, as well as the patient, in a collaborative approach to treatment. For example, having a clear line of communication with the dispensing community pharmacist can be an important component of the care process. The pharmacist may be able to identify potential problems with maintaining the shared decision-making plan, either through calculating medication possession ratios or via direct discussion.26 The pharmacist may also be able to facilitate the use of Webster packs or dosette boxes (the former is generally more successful for people with SMI) to support better medication-taking rates. The pharmacist can also undertake some reconciliation of prescriptions where multiple prescribers are involved.
For the nonpsychiatrist, where a comorbid mental health condition is suspected, referral of the patient for appropriate assessment should be routinely undertaken. For diabetes teams, psychological assessment should be easily accessible, especially for patients with type I diabetes.27 Psychiatric and psychological comorbidities are often present in patients with diabetes and should be routinely considered.28
Finally, the use of motivational interviewing is a highly recommended method of engaging the patient to enhance attendance, shared-decision making and persistence. It is also a useful tool for dealing with stress, a very real contributor to metabolic dysregulation, especially in patients with hyperglycaemia.29-31
TIP: Engage in formal shared care arrangements where possible.
Conclusion
It is important that GPs are aware of the association between SMI and diabetes, and manage patients with either condition appropriately, particularly younger patients. This includes regular screening for hyperglycaemia, diabetes and related comorbidities in patients with SMI, as well as being aware of depressive and anxiety symptoms in patients with type 2 diabetes. Supporting patients to understand the importance of regular tests and screening, managing patients through a network of linked healthcare professionals and regularly reviewing treatment regimens, particularly if psychotropic polypharmacy is involved, will help GPs to better manage patients and help in early detection of comorbidities and treatment. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.