Exercise in prediabetes and type 2 diabetes: moving beyond advice

Diabetes type 2
Exercise and physical fitness
Exercise can reduce the level of health risk in people with prediabetes and type 2 diabetes. However, merely advising patients to exercise is not enough – appropriate screening and management are required to ensure the safety and efficacy of the prescribed exercise program.
- Lifestyle intervention involving regular exercise reduces the risk of adults with prediabeties progressing to type 2 diabetes.
- Regular aerobic or resistance exercise, either alone or in combination, can improve glycaemic control in type 2 diabetes. Improvements are superior for people who achieve or exceed current exercise guidelines.
- Regular exercise also improves common comorbidities in type 2 diabetes (e.g. hypertension, dyslipidaemia, abdominal fatness and mental health).
- Providing people only with advice to engage in exercise is associated with poor patient adherence and has little effect on markers of glucose control.
- Appropriate pre-exercise screening and management of comorbidities and medication interactions is required for safe and effective exercise programs for people with type 2 diabetes, including blood glucose management during and after exercise.
- Referral to an accredited exercise physiologist is recommended before starting a new exercise regimen, or significantly changing a current one. This includes consideration of comorbidities and diabetes complications such as and microvascular disease, when exercise may need to be modified or is contraindicated.
Exercise can reduce the risk of people with prediabetes progressing to type 2 diabetes, and in those with type 2 diabetes it can reduce blood glucose levels and improve markers of cardiovascular disease (CVD) risk.1 However, just advising patients to exercise does not improve glucose control. In fact, without appropriate screening and exercise management, it can reduce exercise adherence or cause harm. Referring people with type 2 diabetes to an accredited exercise physiologist (AEP) is recommended to ensure that the exercise prescribed is safe and effective.
Safety and efficacy of exercise in prediabetes and type 2 diabetes
Exercise can reduce the risk of adults with prediabetes progressing to type 2 diabetes, and for those with type 2 diabetes it has beneficial effects on glycaemic control and CVD risk factors. Landmark studies such as the US Diabetes Prevention Program and the Da Qing study have clearly established that exercise is a key component for reducing the progression of prediabetes to type 2 diabetes.2,3 The Da Qing study showed an average 47% reduction in incidence of type 2 diabetes compared with the control group at 6-year follow-up, and benefits from exercise remained at 20-year follow-up.3 Furthermore, lifestyle interventions may be at least as effective as pharmaceutical interventions for reducing progression of prediabetes to type 2 diabetes.4 Data from the US program show lifestyle interventions involving regular exercise can reduce the incidence of type 2 diabetes in people with prediabetes by 58% whereas metformin reduced the incidence by 31%.2 Exercise has other health benefits beyond managing glycaemia, and a focus on lifestyle modification rather than pharmaceutical intervention can improve other areas of health including mental wellbeing, and can mitigate drug side effects. Increased exercise is necessary to reduce progression to diabetes and the burden of disease on individuals and healthcare systems.
For people with established type 2 diabetes, exercise can improve glucose control and it has a significant positive effect on risk factors for CVD. Exercise acutely lowers blood glucose and increases insulin sensitivity for 24 to 48 hours after exercise, resulting in better glucose control independent of insulin-sensitising medication or insulin injections.5 Exercise studies that used continuous glucose monitoring have shown that after an acute bout of moderate to vigorous aerobic exercise, there is a corresponding reduction of time spent in hyperglycaemia as well as decreased postprandial hyperglycaemia (Figure). Results from a high-quality meta- analysis established that regular exercise for 12 weeks or more lead to a mean reduction in HbA1c of about 0.89% when exercise was equal to or more than 150 minutes per week.6 These levels of exercise are also associated with significant improvement in macrovascular and microvascular endpoints.7 Furthermore, exercise may potentially lower the dosage of medication needed to achieve optimal blood glucose maintenance.
{kind=link}
Exercise therapy is important for broader health management beyond glucose control in people with type 2 diabetes. Other well-documented effects of exercise include improved cardiac and vascular function, which is of particular relevance in type 2 diabetes, where one in three people with type 2 diabetes have CVD and mortality from CVD is high.8,9 Exercise also has positive effects on a number of CVD risk factors such as reducing systolic and diastolic blood pressure, reducing blood triglycerides and LDL-cholesterol, and increasing HDL-cholesterol. Notably, exercise improves cardiorespiratory fitness, which is itself an independent predictor of CVD risk and mortality.10 Intensive glucose-lowering therapy using medication has not consistently been associated with lower all-cause mortality or death from CVD; however, even small increases in cardiorespiratory fitness have been shown to reduce risk of mortality.11 Managing CVD risk factors is a key component of managing diabetes. Given such strong evidence for exercise benefits in people with type 2 diabetes, there is a significant need for these patients to engage in appropriate targeted exercise.
Another component of lifestyle interventions for people with prediabetes and type 2 diabetes is fat loss. Exercise may aid in weight loss when dietary modification is also undertaken, but little or no change in body weight may result from exercise alone. A common misconception is that exercise only confers benefits when weight loss occurs. However, exercise even without weight loss still yields clinically relevant improvements in health outcomes including decreased visceral fat.12
Exercise guidelines
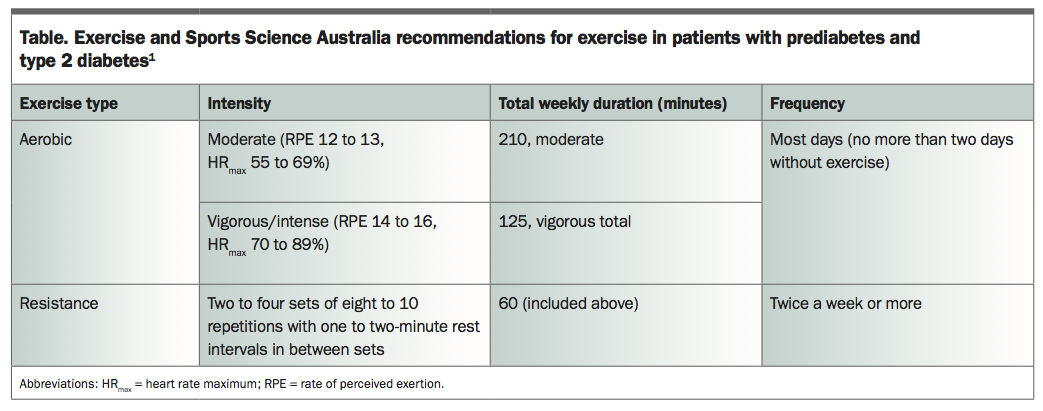
Exercise and Sports Science Australia (ESSA) has well-established exercise recommendations for people with prediabetes and type 2 diabetes. Broadly, exercise has two forms: aerobic training and resistance training. Exercise guidelines for aerobic training focus on large, rhythmic muscle activities such as walking, running and cycling, and provide advice on intensity of aerobic exercise, which is usually measured as a percentage of predicted maximum heart rate (%HRmax) or as a rating of perceived exertion (RPE). Moderate intensity is defined as exercise with an RPE of about 12 to 13 out of 20 (perceived as ‘somewhat hard’) or equivalent heart rate (55 to 69% of HRmax).12 Vigorous intensity is exercise with an RPE of 14 to 16 out of 20 (perceived as ‘hard’) or 70 to 89% of HRmax. Additionally, the talk test can be used to prescribe aerobic training. A person doing moderate intensity aerobic exercise may be able to talk whereas at high intensity exercise they may not be able to say more than a few words without taking a breath. ESSA recommends a weekly minimum of 210 minutes of moderate exercise or 125 minutes of vigorous exercise for people with prediabetes and type 2 diabetes. Some physiological benefits of exercise are transient, lasting only 24 to 48 hours, thus training needs to provide regular ‘doses’ of exercise stimulus to maintain benefits. For instance, patients should not go more than two consecutive days without undertaking some form of aerobic exercise.
Resistance training is exercise in which free weights, machines, bands or body weight are used to create moderate to high loads on muscle. Resistance exercise has been shown to be very effective for increasing insulin sensitivity and glucose control for 24 to 48 hours post-exercise. Therefore, people with prediabetes and type 2 diabetes should undertake resistance exercise targeting major muscle groups twice a week. ESSA recommends that eight to 10 different exercises (with two to four sets of eight to 10 repetitions and short rests of 1 to 2 minutes between sets) be included in the total weekly exercise program.1
Exercise training should include both aerobic and resistance exercise, as studies have shown better results on blood glucose markers with combined exercise modes compared with either one in isolation (Table).
{kind=link}
Special considerations
Although exercise is extremely potent for improving health outcomes for people with prediabetes and type 2 diabetes, merely providing patients with advice to engage in exercise does not result in adherence. For most people, such advice is insufficient to change their behaviours and improvements in health outcomes, including glucose control, are poor or nonexistent with this approach.6 Referral to appropriate allied health professionals for screening, exercise prescription and lifestyle counselling are crucial for improving exercise behaviours in sedentary and inactive patients with prediabetes and type 2 diabetes.
Not only is advising people with type 2 diabetes that they should exercise of limited efficacy, but such advice without appropriate screening and prescription may place these patients at risk of injury or exacerbate concomitant comorbidities or disease (such as hypertension, peripheral vascular disease, foot ulcers and uncontrolled glycaemia). General advice to engage in 150 minutes of exercise or more per week, without appropriate instruction, supervision and consideration of contraindications to specific exercise modalities, could prove harmful. Patients with multiple comorbid conditions usually have the most to gain from exercise, and benefit from the wide-ranging improvements in health that exercise offers. However, exercise prescription in these people needs to be specific and personalised to limit any exercise-related risk.
Another consideration for the safe prescription of exercise for this patient group is the interaction between medications and exercise, most notably insulin and sulfonylureas, which can cause hypoglycaemia. For safe exercise prescription, an understanding of exercise and drug interactions is necessary to limit the possibility of adverse events. Although exercise training is safe and effective, even in patients with concomitant disease and polypharmacy, general advice may be inappropriate and lead to harm. Allied health professionals such as AEPs have the necessary training to prescribe safe and effective exercise for these patient groups.
Asymptomatic diseases such as coronary artery disease may be present in people with type 2 diabetes and established CVD is often present in these patients. Referral to AEPs is necessary for appropriate pre-exercise screening so that the exercise program prescribed is safe and effective, and pre-exercise medical assessment by a specialist may also be indicated. Although the risk of harm from exercise is low, the potential adverse outcomes are significant. Risk management through pre-exercise screening (including history of CVD, diabetes complications, current exercise and lifestyle factors, and graded exercise testing with ECG) is required to ensure patients at risk of asymptomatic disease are managed appropriately.
Referrals under existing government health initiatives such as the chronic disease GP Management Plan and Group Allied Health Services Under Medicare should be recommended early for patients with prediabetes and type 2 diabetes who are not engaging in regular exercise.
Conclusion
Exercise has wide-reaching benefits for people with prediabetes and type 2 diabetes. Large-scale trials have confirmed that exercise is a critical component for reducing the risk of prediabetes progressing to type 2 diabetes. For all people, including those with type 2 diabetes, exercise benefits extend beyond improved glucose metabolism and include improved CVD risk profile and reduced risk of all-cause mortality. Exercise is a safe and effective therapeutic tool when screening of concomitant and asymptomatic disease is carried out. Unfortunately, just advising patients to exercise has little impact on adherence and glycaemia. AEPs have the knowledge to improve adherence and prescribe safe and effective exercise programs.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.