Statin intolerance in people with diabetes: a clinical approach

Lipid disorders
Diabetes type 2
Diagnosing statin intolerance is challenging because of a lack of specific diagnostic tests and high background rates of muscle and liver abnormalities. Ideally the patient’s abnormalities should be reassessed after statin withdrawal and rechallenge, and alternative diagnoses should be explored. Well-proven management options for statin intolerance are changing to an alternative statin, low-dose statin therapy and trialling other LDL-cholesterol lowering drugs.
- HMG-CoA reductase inhibitors (statins) are of proven benefit for the primary and secondary prevention of coronary artery disease in people with diabetes.
- Improper management of presumed statin intolerance can lead to missing an alternative diagnosis and people not gaining statin-related cardiovascular risk reduction benefit.
- The diagnosis of statin intolerance is hampered by the lack of specific tests and high background rates of muscle symptoms and abnormal liver function tests.
- Ideally the diagnosis should be confirmed after statin withdrawal and rechallenge with the same or another statin following resolution of abnormalities and consideration of alternative diagnoses.
- Many people who have experienced statin intolerance are able to tolerate an alternative statin, low-dose statin therapy or other LDL-cholesterol lowering drugs.
HMG-CoA reductase inhibitor (statin) drugs are commonly prescribed medications that lower coronary artery disease (CAD) event rates over five years by 21% per 1.0 mmol/L reduction in LDL-cholesterol levels (LDL-C) in people with diabetes, which is similar to the effect achieved in people without diabetes. A 9% reduction in all-cause mortality per 1.0mmol/L reduction in LDL-C levels (over five years) has also been observed in people with diabetes, similar to the 13% reduction in those without diabetes.1,2 The benefits of statins are therefore similar in people with or without diabetes, and among people with diabetes statin benefits are similar irrespective of whether there is a prior history of vascular disease or other baseline characteristics (e.g. diabetes type, gender, age, body mass index and pretreatment lipid levels).2 Statin therapy also lowers triglyceride levels by about 13% and increases HDL-cholesterol levels by about 5%.1 Statins may also have pleiotropic anti-inflammatory, antioxidant, antiplatelet/antithrombotic and vasodilatory actions, which may contribute to their vasoprotective effects.3
Australian guidelines recommend moderate or high-dose statin therapy for people with diabetes who have CAD, or who are at moderate to high risk of CAD, based on an existing diagnosis of CAD, renal damage or an estimated cardiovascular disease risk of more than 10% using risk calculators (see www.cvdcheck.org.au).4
It is estimated that 2 to 20% of people taking statins experience statin-related side effects,5 with rates of up to 50% in patients referred to specialist lipid clinics.6
Challenges to diagnosing a statin intolerance include the lack of specific diagnostic tests and high background rates of muscle and liver abnormalities, particularly as nonalcoholic fatty liver disease (NAFLD) and alcohol- or drug-induced liver dysfunction are common in people with diabetes. Underinvestigated or undertreated statin intolerance can leave people at heightened risk of CAD, with consequences for patients, families, the community and healthcare system, and can also result in a missed alternative diagnosis.
This article briefly reviews statin intolerance, including its definition, risk factors, differential diagnoses and potential treatment approaches. Several national and international bodies have recently published comprehensive guidelines.7-9
Definition
Statin intolerance is defined as an intolerance to statin therapy related to attributed symptoms and/or biochemical abnormalities that develop after statin commencement, resolve after statin withdrawal and recur with exposure to the same or another statin. Each phase may take days to weeks. Drug withdrawal and rechallenging is seldom performed in clinical practice and subsequently many people who may potentially benefit from statin treatment go without due to misattribution of symptoms or abnormal blood test results to statin intake.
Presentation
Statin intolerance usually occurs within weeks of statin commencement or a dosage increase, or may be triggered by the development of an intercurrent condition, such as hypothyroidism, worsening renal function or the use of drugs that increase blood statin concentrations (e.g. erythromycin).
The most common presentation is muscle related (in about 80% of cases), including muscle pain, which may occur with or without elevated circulating creatine kinase levels. Placebo-controlled randomised controlled trials demonstrate that some muscle symptoms attributed to statins may not be truly statin related. For example, in the three-year primary prevention Heart Outcomes Prevention Evaluation (HOPE)-3 trial, muscle pain/weakness was reported in 5.8% of patients treated with rosuvastatin, and also in 4.7% of participants in the placebo group.10 The extremely rare, but most severe form of myopathy, rhabdomyolysis, occurs at a rate of 0.70/100,000 patient-years.9 If a patient develops this kidney and life-threatening side effect, drug cessation and no further statin challenge are recommended. A rise in creatine kinase levels may also be asymptomatic, and elevated levels, even more than fivefold the upper limit of normal levels, can occur with recent exercise or with hypothyroidism.11
Asymptomatic abnormal liver function tests (LFTs) are the second most common form of statin intolerance, with elevated aminotransferase levels (more than three times the upper limit of normal) occurring in 3% or fewer of patients treated with statins. Most resolve spontaneously within weeks, even without drug discontinuation,12 with there being no strong evidence of liver damage from long-term statin use. As abnormal LFTs and creatine kinase levels are common, it is wise to check levels before statin commencement.
Other statin attributed symptoms such as erectile dysfunction, insomnia and effects on cognition are often promoted by the media and are less well-validated.13 There is no strong evidence that statins contribute to cognitive decline. Indeed, placebo-controlled trials of statins that include validated tests of cognitive function have not revealed any concern to date.14
Statin therapy may increase the risk of developing type 2 diabetes by 9%,15 although usually only in people with risk factors for diabetes. It is not known whether statin cessation can reverse such new-onset diabetes. New-onset diabetes is not usually regarded as a feature of statin intolerance.
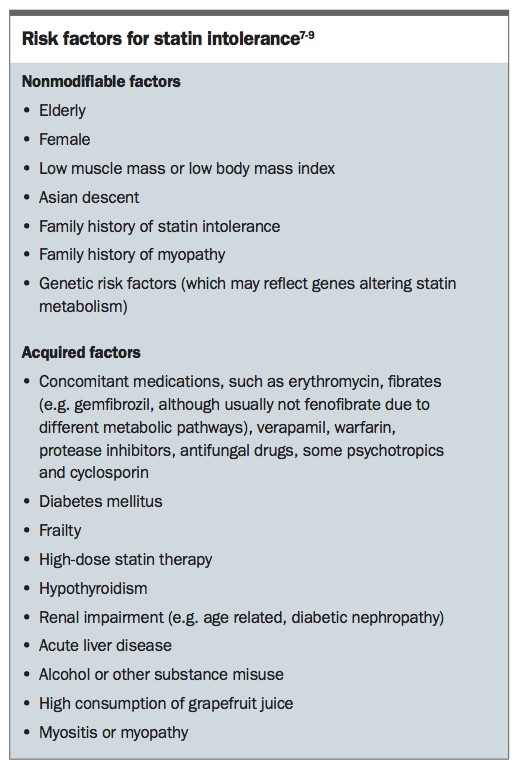
Risk factors
Risk factors for statin intolerance are summarised in the Box.7-9 As noted, diabetes and other conditions common in diabetes, such as renal impairment and liver disease, are risk factors.
{kind=link}
Differential diagnoses
Differential diagnoses for statin intolerance include other causes of muscle pain such as neuromuscular disorders (e.g. myopathies, fibromyalgia or neuropathy), connective tissue disorders, thyroid disease, vitamin D deficiency, depression, injury, viral illnesses and, for lower limb pain, peripheral vascular disease.
Abnormal LFTs may be due to hepatitis (infectious, alcoholic or drug-induced), NAFLD, autoimmune diseases or storage disorders (e.g. haemochromatosis or Wilson’s disease).7-9
Assessment
Assessment of patients with statin intolerance should include careful history taking and physical examination and review of medications, including over-the-counter treatments. Discussion with a pharmacist may help regarding medications or drug interactions that may induce the symptoms or cause abnormal blood tests. Investigations may include full blood count, erythrocyte sedimentation rate, measurement of muscle enzymes (creatine kinase and urinary myoglobin), LFTs, thyroid function tests, vitamin D levels and, as appropriate, iron studies, hepatitis serology, autoantibodies and perhaps even an electromyogram or muscle biopsy.7-9
Management
The diagnosis of statin intolerance should be confirmed after exclusion of other causes of the symptoms and/or signs, and after rechallenge of the statin following its withdrawal and the cessation of the initial symptoms and/or signs. If the patient develops rhabdomyolysis, the statin should be ceased and not rechallenged. Some patients are reluctant to be rechallenged, even at lower doses with the same statin, and an alternative statin may be more acceptable to them. Clinical and biochemical review at approximately four-weekly intervals is reasonable.7-9
After drug cessation and resolution of the abnormal symptoms or signs, therapeutic options for patients with a statin intolerance are to:
- rechallenge with the original statin at a reduced dose and slowly uptitrate the dosage as tolerated over a four-week period
- change to an alternative statin and slowly uptitrate the dosage as tolerated
- change to a low-dose statin with alternate day dosing and slowly uptitrate the drug frequency and/or dose as tolerated
- use another LDL-C lowering drug.
Changing to a statin that is hydrophilic (such as pravastatin or rosuvastatin) or one that has a different metabolic pathway (such as not via the hepatic cytochrome P450 system) may be helpful. An example of using a low-dose statin with alternate day dosing is rosuvastatin 5mg daily on three days a week, separated by at least one day, with a gradual increase of dose (over two to four weeks) to 10mg on three days a week or 5mg daily. If this is tolerated, the dosage can be further increased (for example, to 10 mg on three days a week with 5mg on other days).7-9 Even a once-weekly statin regimen can significantly lower LDL-C levels,16 but clinical trial evidence showing reduction of hard clinical end points with this approach is awaited.
Alternative LDL-C lowering medications, such as ezetimibe, bile acid binding resins or the effective but currently costly (predominantly private script) two-weekly subcutaneous injection of evolocumab (a proprotein convertase subtilisin/kexin type 9 [PCSK9] inhibitor), may be used instead of or with low-dose statins.7-9,17 Although nicotinic acid can improve the lipid profile, the drug is not recommended as it usually very poorly tolerated due to flushing and gut upset and can induce or worsen hyperglycaemia and gout. Furthermore, trials have not shown cardiovascular disease benefit of nicotinic acid.
Patients should be encouraged to continue a healthy diet, including a safe level of alcohol and perhaps use of plant sterol-containing foods (e.g. margarines), which can lower LDL-C levels by 10 to 15%.18
Patients are often aware of or have tried over-the-counter LDL-lowering alternatives, including red yeast rice, which is a weak natural source of lovastatin.19 There is anecdotal and some clinical trial evidence that some over-the-counter supplements, such as vitamin D, coenzyme Q10 or magnesium (in particular, magnesium orotate), alone or in combination, may be helpful but overall the evidence is weak and robust clinical trials are required.7-9,20-22
Summary
Statin drugs are of proven benefit to people with diabetes and those with or at high risk of cardiovascular disease. Symptoms or abnormal blood tests that may represent true statin intolerance are common in clinical practice. Careful history taking and examination and prudent investigations while the patient is taking a statin and after statin withdrawal, as well as statin rechallenge, will help diagnose statin intolerance. The most common and well-proven management options are the use of an alternative statin, low-dose statin therapy and use of other LDL-C lowering drugs. ET
Acknowledgement
Professor Jenkins is supported by a NHMRC Practitioner Fellowship and Sydney Medical Foundation Fellowship.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.