Endocrinopathies of lithium: common and treatable

Endocrine diseases
Lithium is effective in the treatment of patients with mood disorders; however, it has a narrow therapeutic index and is associated with a number of significant toxicities including endocrinopathies. Routine monitoring for complications is indicated to enable timely lithium cessation or initiation of treatment.
- Thyroid and parathyroid dysfunction and nephrogenic diabetes insipidus (DI) are common in patients treated with lithium.
- For patients undergoing lithium therapy, thyroid function and calcium levels should be monitored at baseline, then every three to six months after starting treatment, and then every six to 12 months long term.
- Levothyroxine should be initiated in patients with overt hypothyroidism or enlarged goitre, or in asymptomatic patients with thyroid stimulating hormone (TSH) levels greater than 10.0 mU/L. It may also be initiated in symptomatic patients with a TSH level of 3.5 to 10 mU/L.
- Management of a patient with persistent hyperparathyroidism may include careful observation with vitamin D3 supplementation, surgical intervention or medical therapy with cinacalcet hydrochloride in patients with contraindications to surgery.
- In patients with suspected nephrogenic DI, the diagnosis should be confirmed with a water deprivation test.
- Cessation of lithium therapy should be considered for patients with early or overt nephrogenic DI and they should be monitored for hypernatraemia.
- Amiloride hydrochloride is first-line treatment for patients with confirmed nephrogenic DI but starting amiloride requires close monitoring of the serum lithium level and adjustment of lithium dosage.
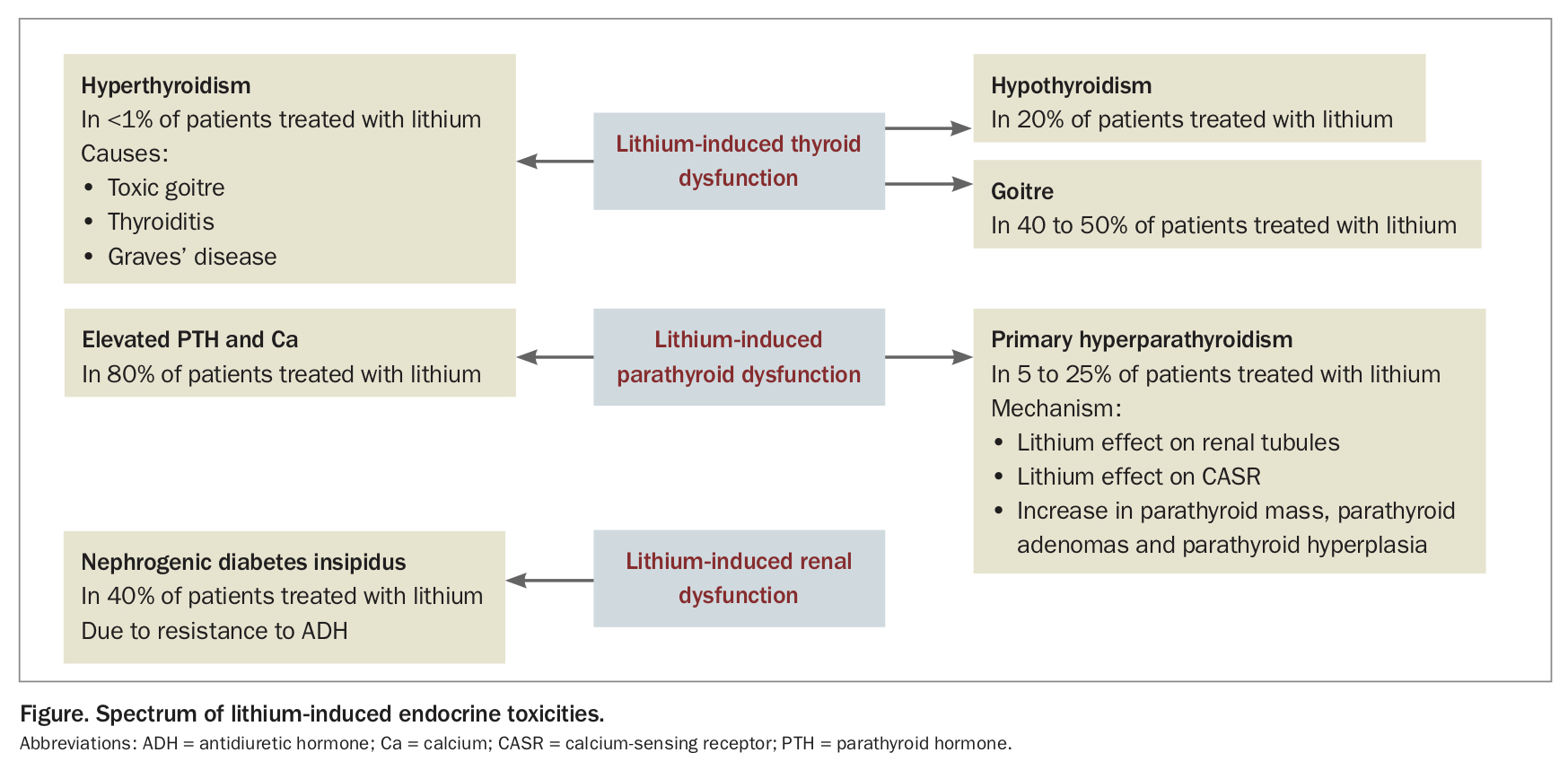
Lithium is widely used in the management of patients with mood disorders and is effective in preventing relapse, protecting against both depression and mania, and reducing the risk of suicide.1,2 Although efficacious, lithium use is also associated with significant toxicity. Endocrine and renal toxicities are common, particularly thyroid and parathyroid dysfunction, as well as nephrogenic diabetes insipidus (DI). Lithium appears to contribute to weight gain but not to metabolic syndrome; however, risk factors for metabolic syndrome should be considered in all patients taking lithium due to its association with mood disorders. All patients prescribed lithium should be routinely referred to an endocrinologist, for the development of a shared management plan, and urgently referred if an endocrinopathy is suspected (Box). We discuss below some common adverse effects including endocrinopathies associated with lithium therapy (Figure).
{kind=link}
{kind=link}
Lithium-induced thyroid disorders
Lithium has many effects on thyroid physiology. It inhibits the synthesis and release of thyroid hormone, which causes hypothyroidism, elevated thyroid stimulating hormone (TSH) levels and compensatory thyroid enlargement, and promotes thyroid autoimmunity, which also causes hypothyroidism, thyroiditis and, less commonly, Graves’ disease. Lithium-induced thyroid abnormalities are common. For patients undergoing lithium therapy, thyroid function should be monitored at baseline, then every three to six months after starting treatment, and then every six to 12 months long term.
Goitre
Lithium-induced goitre occurs in up to 40 to 50% of patients treated with lithium.3,4 The goitre is usually diffuse, enlarged to about twice the size of the normal thyroid and may develop within weeks or up to years after starting lithium therapy.3,5,6 Management for patients who develop a lithium-induced goitre should be the same as for any other goitre. If nodules are detected clinically, they should be investigated further with ultrasonography and/or fine needle aspiration, where indicated, to exclude malignancy. Thyroxine treatment may reduce goitre volume and can therefore be considered in patients with significant goitre and compressive symptoms.3,4,6 Surgery should be considered if thyroxine is ineffective or there are significant compressive symptoms.3
Hypothyroidism
Lithium-induced hypothyroidism occurs in up to 20% of patients treated with lithium. Hypothyroidism is primarily due to inhibition of thyroid hormone synthesis and release, and may occur in patients without thyroid enlargement as well as in those who develop goitre.3,4 In addition, there is evidence that lithium therapy can be associated with the development of thyroid autoantibodies, or an increase in their titre if present before lithium administration.7 Risk factors for the development of lithium-induced hypothyroidism include female sex, increasing age (more than 50 years), family history of thyroid disease and positive thyroid autoantibodies.5,8,9 Increased frequency of monitoring may be considered in patients with risk factors present.
Presentation of lithium-induced hypothyroidism is the same as that of hypothyroidism in the general population. In patients with mood disorders, neuropsychiatric symptoms of hypothyroidism and subclinical hypothyroidism are of particular relevance and include symptoms of lethargy, mental slowing, decreased concentration and memory, and depression. The presence of these symptoms should be considered when making treatment decisions. Patients with subclinical hypothyroidism with a TSH level less than 10 mU/L may not require treatment if they are asymptomatic but should be closely monitored. Patients with a TSH level less than 10 mU/L who are symptomatic, those with a TSH level greater than 10 mU/L, or with goitre or overt hypothyroidism should be treated with levothyroxine. Thyroid function usually normalises on cessation of lithium therapy and levothyroxine may be discontinued.10 If lithium is to be ceased, levothyroxine treatment must be reconsidered and thyroid function monitored to avoid iatrogenic hyperthyroidism which may exacerbate psychiatric symptoms. We suggest monitoring of thyroid function every four to six weeks after cessation of lithium with levothyroxine dose adjustment as required until thyroid function stabilises. If levothyroxine can be discontinued, thyroid function can then be monitored every six to 12 months. If there is an ongoing levothyroxine requirement, thyroid function should be monitored every three to six months.
Hyperthyroidism
Lithium-induced thyrotoxicosis has a much higher incidence than thyrotoxicosis in the general population (2.7 cases per 1000 vs 0.8 to 1.2 cases per 100,000) and may be due to toxic goitre, thyroiditis or Graves’ disease.3,11 Lithium-induced thyrotoxicosis is most often due to transient and painless thyroiditis. One proposed mechanism is a direct toxic effect of lithium on the thyroid.3,4 Lithium has also been shown to induce the production of thyroid autoantibodies suggesting the pathogenesis may in some cases be autoimmune.7,12 Although Graves’ disease is described in patients treated with lithium, there is no evidence that lithium induces the production of TSH receptor antibodies and these cases may be coincidental.
The management of lithium-induced thyrotoxicosis is similar to that of thyrotoxicosis in the general population. Thyroiditis management may be supportive or require corticosteroid therapy. A toxic goitre may be managed with radioiodine therapy or surgery. The options for management of Graves’ disease include antithyroid medical therapy (with carbimazole or propylthiouracil), radioiodine or surgery.
Lithium-induced parathyroid disorders
Hyperparathyroidism associated with lithium therapy was first described in 1973.13 Since then, a number of cases of hyperparathyroidism associated with lithium therapy have been reported. Lithium causes an increase in parathyroid hormone (PTH) and calcium levels in 80% of patients within weeks of starting treatment.14 The rise in PTH and calcium levels is usually mild, at about 10%, and generally remain within the normal range.14,15 Although estimates vary widely, approximately 5 to 25% of patients taking lithium develop hypercalcaemia and hypocalciuria with elevated or inappropriately normal PTH levels, consistent with primary hyperparathyroidism.14,16-20 Like primary hyperparathyroidism, lithium-induced hyperparathyroidism is more prevalent in females, with the female-to-male ratio estimated at 4:1.19
Lithium-induced hyperparathyroidism may be asymptomatic or associated with a number of clinical features, including exacerbation of psychiatric symptoms or manifestations, nephrolithiasis, hypercalcaemic crisis, worsening hypertension, fatigue, constipation, abdominal pain, bone pain, bone demineralisation and osteoporosis.18,20
The mechanism of lithium-induced hyperparathyroidism is multifactorial. Lithium reduces renal calcium clearance, which seems to be a direct effect of lithium on the renal tubules since it occurs early after treatment initiation and before PTH levels rise.21 In addition, lithium reduces the sensitivity of the parathyroid cell to extracellular calcium, causing a shift in the inhibitory setpoint for PTH to a higher calcium concentration.19,20,22 These actions are proposed to be a direct effect of lithium on the calcium-sensing receptor (CASR) located in the parathyroid gland and renal tubules. Long-term lithium therapy causes an increase in parathyroid mass, parathyroid adenomas and parathyroid hyperplasia.18,20,23 The frequency of parathyroid hyperplasia versus adenoma is variable; however, patients with lithium-induced hyperparathyroidism have a higher prevalence of parathyroid hyperplasia and multiple adenomas than those with primary hyperparathyroidism, which has implications for surgery.19,23
Lithium-induced changes in calcium and PTH homeostasis are usually reversible if lithium is discontinued; however, in some cases, long-term lithium use can cause irreversible hypercalcaemia.20 There are several approaches to management of patients for whom discontinuation of lithium is contraindicated due to psychiatric illness, or for those who have persistent hyperparathyroidism despite cessation of lithium. In patients with mild asymptomatic hypercalcaemia (corrected calcium less than 2.85 mmol/L) a conservative approach with surveillance may be appropriate.24,25 Vitamin D3 supplementation should be considered as this has been shown to reduce PTH, improve bone mineral density and reduce bone turnover.26 We recommend aiming for a serum vitamin D level of 75 nmol/L.27 If intervention is required, first-line treatment for management of hyperparathyroidism is surgery. Given the prevalence of multiglandular disease, the surgical approach is controversial, with some advocating for isolated adenoma resection with intraoperative PTH measurement and others for bilateral neck dissection and multigland excision.28-30 Variable cure rates after surgical treatment are reported, ranging from 58 to 100% for patients with lithium-induced hyperparathyroidism compared with more consistent cure rates of 90 to 95% for those with primary hyperparathyroidism. Calcimimetics such as cinacalcet increase the sensitivity of the CASR to serum calcium, reducing the secretion of PTH and serum calcium. Cinacalcet is effective in normalising serum calcium and reducing PTH in hyperparathyroidism and there are case reports of it being successfully used to treat lithium-induced hyperparathyroidism, although it must be noted that cinacalcet is not PBS listed for the treatment of primary hyperparathyroidism.19,31-33
Given the prevalence of lithium-induced hyperparathyroidism, monitoring of calcium and PTH levels in patients undergoing lithium therapy is recommended at baseline, then at six months after starting therapy, then at 12 months, and then annually if stable.34 If lithium-induced hyperparathyroidism is detected and is suitable for conservative management, bone mineral density assessment is recommended every one to two years.24
Lithium-induced nephrogenic diabetes insipidus
Although not strictly an endocrine complication of lithium, nephrogenic DI induced by lithium is a common endocrine consultation. Nephrogenic DI occurs in up to 40% of patients treated with lithium. Under normal circumstances antidiuretic hormone (ADH) regulates water permeability of the principal cells in the collecting tubule and promotes water reabsorption via aquaporin-2 water channels. Lithium causes resistance to ADH resulting in polyuria and polydipsia. Over time, this may become irreversible.35-37 In addition to polyuria and polydipsia, nephrogenic DI may cause hypernatraemia which, in severe cases, can cause reduced consciousness, seizures, coma and even death.38 Sodium should be monitored in patients suspected of having nephrogenic DI.
For patients who develop polyuria and polydipsia with lithium therapy, a water deprivation test may be considered to confirm nephrogenic DI and exclude central DI or psychogenic polydipsia as the cause of symptoms. If nephrogenic DI is confirmed, consideration should be given to ceasing lithium therapy, which may resolve the symptoms of DI. If lithium is continued, amiloride may be used as first-line treatment for nephrogenic DI. Amiloride inhibits the epithelial sodium channels in the collecting tubules and prevents the entry of sodium and lithium, thereby preventing ongoing lithium toxicity.35 In clinical trials amiloride resulted in increased urinary concentrating ability and a reduction in urine output.37,39 Lithium has a narrow therapeutic index and small changes in concentration can result in toxicity or subtherapeutic levels. Amiloride may alter lithium concentration and lithium levels must therefore be monitored carefully if amiloride and lithium are continued concurrently, and the lithium dose adjusted accordingly.40 Other treatment options include thiazide diuretics in conjunction with a low-salt diet and NSAIDs. Supraphysiological doses of desmopressin may be effective in patients with partial ADH resistance.38
Metabolic syndrome
There is conflicting evidence for weight gain and development of metabolic syndrome as a result of lithium use. Although lithium does seem to be associated with mild weight gain, there is no conclusive evidence for the development of metabolic syndrome.41-44 However, the prevalence of obesity and metabolic syndrome is higher in patients with mood disorders than in the general population and risk factors should always be considered in patients treated with lithium.45-47
Conclusion
Lithium is the mainstay of treatment for bipolar disorder; however, it is associated with a number of adverse effects including endocrinopathies. Monitoring for thyroid and parathyroid dysfunction is recommended in all patients treated with lithium and treatment may be indicated if abnormalities are detected depending on the severity. Polyuria and polydipsia are common and, if nephrogenic DI is confirmed, specific treatments can be initiated. Risk factors for metabolic syndrome should be considered in all patients treated with lithium because of the strong association between mood disorders, obesity and metabolic syndrome. ET