Bone health: the effects of chronic disease

Osteoporosis
Bone diseases
People with chronic disease often have impaired bone health and their increased risk of fragility fracture is often under-appreciated. Recognition, screening and appropriate management of bone health should form part of the routine management of patients with chronic disease.
- One in two people in Australia have a chronic disease and one in five have multiple chronic diseases.
- Patients with chronic disease often have impaired bone health and are at increased risk of fragility fracture.
- Chronic conditions such as coeliac disease, inflammatory bowel disease, diabetes mellitus, chronic kidney disease and chronic liver disease are associated with increased risk of fragility fracture.
- Recognising the importance of bone health in people with chronic disease and screening for secondary causes of bone loss should form part of routine management.
- Optimal care is best undertaken in a multidisciplinary setting.
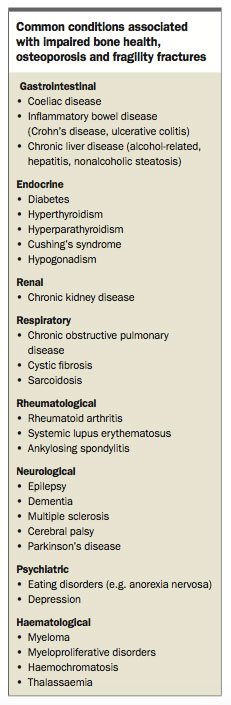
It is estimated that half of all people in Australia have a chronic disease, with one in five people affected by multiple chronic diseases. Chronic diseases are the leading cause of disability and death in Australia and account for a significant economic burden.1 Many of the common chronic diseases are associated with osteoporosis and increased risk of fracture (Box).
{kind=link}
Osteoporosis is characterised by low bone mass and impaired bone quality and affects more than one million people in Australia.2 It is associated with significant morbidity and mortality.3 It is typically asymptomatic until there is a fracture, although most vertebral fractures remain asymptomatic. The effect of chronic disease on bone health is often unrecognised in the management of these complex patients. However, attention to bone health in patients with chronic disease should form a fundamental component of their management.
This article discusses the major mechanisms contributing to bone fragility in people with chronic disease. A practical and systematic approach to the investigation and management of osteoporosis in people with chronic disease in the general practice setting is also considered.
Pathogenesis
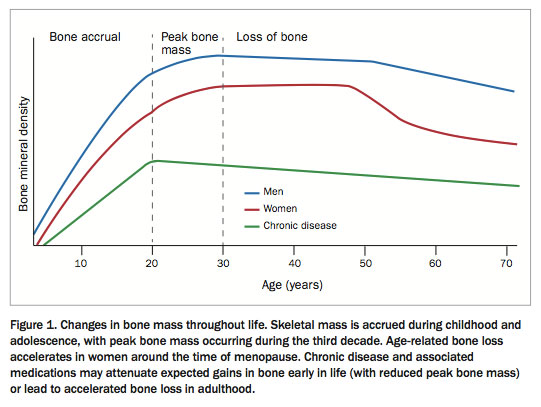
The pathogenesis of osteoporosis in people with chronic disease is multifactorial. Optimal peak bone mass, which is typically reached during the third decade of life, is an important determinant for future fracture risk (Figure 1). Although the accrual of bone and achievement of peak bone mass is largely genetically predetermined, vitamin D and calcium status, physical activity and adequate nutrition also contribute.4,5 Patients with conditions that hinder the achievement of peak bone mass have an increased lifelong risk of osteoporosis and fragility fracture.6
{kind=link}
Sex hormones influence peak bone mass and are crucial to the maintenance of bone health during adulthood. In women, gonadal dysfunction commonly presents with disturbances in menstrual cycles, whereas symptoms are often vague and nonspecific in men and the diagnosis may be delayed.7 Although acute systemic illness can often cause temporary biochemical disruptions in sex hormones, hypogonadism may accompany or be a consequence of chronic diseases.
Adverse effects associated with the use of certain medications such as glucocorticoids can lead to accelerated bone loss. The effect of chronic disease on muscle strength, function and balance may further contribute to an elevated risk of falls and fracture.8
Common chronic diseases associated with bone fragility
Coeliac disease
Coeliac disease, an autoimmune condition triggered by dietary gluten that causes mucosal inflammation within the small intestines, is associated with gastrointestinal symptoms and also skin and neurological manifestations.9 However, symptoms are often nonspecific and the disorder is commonly underdiagnosed.10 Previously thought to be a rare disorder, epidemiological studies indicate its prevalence is 1 to 2% in western communities.11
Coeliac disease results in chronic malabsorption, and the long-standing malabsorption of vitamin D and calcium can lead to osteomalacia, low bone mass and associated significant increase in fracture risk.12 Implementation of a strict gluten-free diet reverses intestinal inflammation, and improve absorption and bone mineral density (BMD).13,14
Inflammatory bowel disease
Patients with inflammatory bowel disease, Crohn’s disease or ulcerative colitis are at an increased risk of metabolic bone disorders. The key contributing mechanisms to bone loss include malabsorption due to intestinal inflammation, small bowel resections and the increased cytokine milieu resulting in high circulating levels of tumor necrosis factor-alpha and interleukin-6.15 These cytokines instigate a cascade within the bone that favours bone resorption and ultimately bone loss.
The adequate control of inflammation, particularly with use of immunological modulators (such as tumor necrosis factor-alpha inhibitors), has beneficial effects on BMD.16 Although use of glucocorticoids may be essential to control inflammation, their long-term use has detrimental effects on BMD and is a risk factor for fractures.15,17
Chronic liver disease
Chronic liver disease secondary to any cause results in an increased risk of fractures.18 The most common causes of chronic liver disease are excessive alcohol intake, chronic viral hepatitis and nonalcoholic steatosis.19 The common mechanism underlying the increased fracture risk in these patients is the persistent low-grade inflammation and increased cytokine milieu. However, vitamin D deficiency, reduced insulin-like growth factor-1 levels, vitamin K deficiency and the direct effects of alcohol also contribute to poor bone health.20
Anorexia nervosa
Anorexia nervosa and other related eating disorders are important risk factors for adverse bone health in younger individuals.21 Poor nutrition during adolescence and young adulthood prevents optimal bone accrual and leads to a failure to achieve peak bone mass.22 Furthermore, gross dietary restriction commonly results in deficiencies of micronutrient such as vitamin D and calcium, as well as of macronutrients (protein, fat and carbohydrates). Endocrine abnormalities, most notably hypogonadotrophic hypogonadism, are important mechanisms for the low bone mass and altered bone microarchitecture observed in these patients.23
The resumption and maintenance of normal body weight usually leads to recovery of hypogonadism and improvements to BMD,24 and it is important that this occurs before the age of peak bone mass. Unfortunately, patients may only experience partial recovery and relapses in adulthood can occur.24
Hyperthyroidism
Hyperthyroidism (most commonly the result of Graves’ disease or a toxic nodular goitre) disrupts normal bone remodelling, leading to reduced BMD and increased fractures.25 Thyroid hormone stimulates bone resorption and leads to bone loss through several mechanisms, including inducing a negative calcium balance due to hypercalciuria and reduced intestinal calcium absorption.26 Treatment of hyperthyroidism is associated with gains in BMD but not always a return to baseline BMD levels.27,28
Diabetes mellitus
Although the micro- and macrovascular complications of diabetes mellitus are well established, impaired skeletal health and increased fractures are also common in people with type 1 or type 2 diabetes.29 The risk factors for impaired bone strength and quality in people with type 1 diabetes include high concentrations of circulating proinflammatory cytokines and lower levels of insulin and insulin-like growth factor-1 levels, which normally stimulate bone formation.30 Patients with type 1 diabetes typically have reduced BMD and the relative risk of hip fracture is almost seven times greater than the general population.29
Patients with type 2 diabetes also have increased fracture risk, although the risk appears to be lower than in those with type 1 diabetes.30 Accumulation of advanced glycosylated end products and vitamin D deficiency predispose to bone fragility.31,32 Patients with type 2 diabetes often fracture at higher BMD than people without diabetes, with T-scores that are often normal.33 This increase in bone fragility is thought to result from microarchitectural impairments in bone quality as opposed to low bone density alone.31 The chronic complications of diabetes such as retinopathy, neuropathy and hypoglycaemia can also predispose to falls and fracture.34,35
Chronic kidney disease
Chronic kidney disease is an increasing public health issue with currently one in ten people in Australia affected.36 Worsening renal function leads to changes in calcium, phosphorus, parathyroid hormone and vitamin D metabolism, which have adverse effects on bone homeostasis. These complex mechanisms are collectively known as chronic kidney disease–metabolic bone disorder (CKD–MBD) and can be grouped as high bone turnover (e.g. hyperparathyroidism) or low bone turnover disease (e.g. osteomalacia and adynamic bone disease but patients most commonly have mixed disease).37 CKD–MBD in general is associated with an increased risk of fracture.38,39 Despite the heterogeneity in bone structure associated with this condition, the Kidney Disease: Improving Global Outcomes organisation recently recommended dual-energy x-ray absorptiometry (DXA) imaging for patients at all stages of chronic kidney disease (stage 1 to 5), including those on dialysis.40
Drugs associated with bone fragility
Glucocorticoids
Most chronic medical conditions necessitate long-term use of medications that have their own specific side effects. Glucocorticoids are important for the treatment of many systemic disorders commonly seen in general practice (e.g. rheumatoid arthritis, systemic lupus erythematosus, chronic obstructive pulmonary disease, sarcoidosis, atopic dermatitis). Bone loss and microarchitectural changes occur within weeks of commencement of their use and fractures occur in 30 to 50% of patients taking them in the long term.41,42
Antiepileptic medications
Antiepileptic medications that induce the cytochrome P450 system increase the catabolism of vitamin D and cause elevations in parathyroid hormone levels. This in turn increases bone resorption and results in the mobilisation of calcium stores from bone.43,44 Patients taking antiepileptic medications have an increased risk of falls and may sustain vertebral fractures as a result of tonic–clonic seizures.
Other medications
Proton pump inhibitors reduce gastric acidity and are associated with an increased fracture risk.45 Aromatase inhibitors, used as adjuvant therapy in the management of postmenopausal women with breast cancer, inhibit the conversion of androgens to oestrogen and rapidly reduce circulating oestrogen levels.46 The oestrogen deficiency state that ensues causes accelerated bone loss with declines in BMD and increased fracture risk.47-49 Similarly, androgen deprivation therapy in men with nonmetastatic prostate cancer results in low testosterone and oestradiol levels and can lead to significant declines in BMD and increased fracture risk.50
Clinical approach
Investigations for osteoporosis in people with chronic disease require the assessment and optimisation of underlying medical conditions and evaluation of fracture risk. In premenopausal women, a menstrual history is important to evaluate potential hypogonadism. In men, symptoms of hypogonadism may be nonspecific and biochemical assessment is also important. Review of medications (including dose of glucocorticoids) and discussion regarding smoking cessation and safe alcohol intake is beneficial for general health as well as bone health. Assessment of vision, balance and gait, and medications that predispose to falls (such as benzodiazepines and antidepressants), with allied health review as necessary, may also reduce falls risk.
Absolute fracture risk calculators are available and incorporate risk factors for osteoporosis together with BMD to stratify fracture probability. Two fracture risk calculators commonly used to aid clinicians are the Garvan fracture risk calculator and the fracture risk assessment tool (FRAX).
Imaging studies and laboratory investigations are performed based on clinical assessment. BMD testing using DXA imaging at the lumbar spine and hip is the modality of choice for the diagnosis of osteoporosis. Baseline thoracolumbar x-rays should be performed as vertebral fractures are highly prevalent and often asymptomatic (Figure 2).
{kind=link}
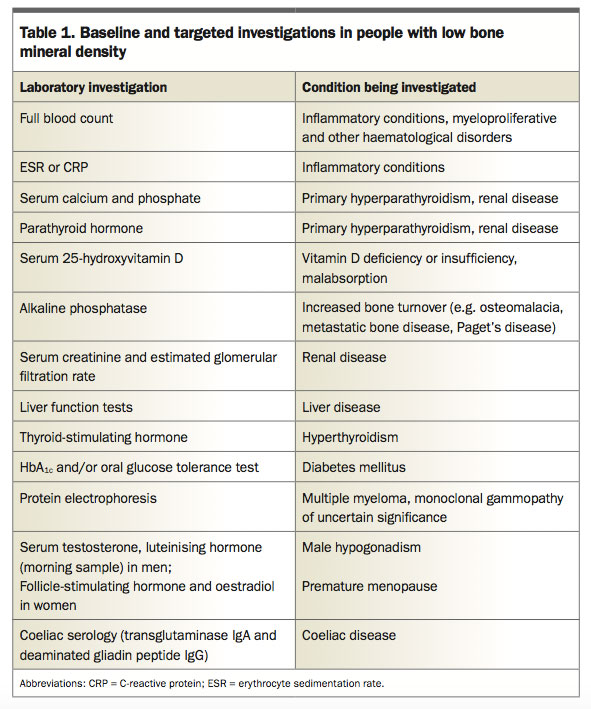
Laboratory testing is useful to exclude an additional cause of low BMD (particularly low vitamin D levels) and to ensure safety when prescribing medications for osteoporosis. Baseline laboratory evaluation includes renal and liver function tests, a full blood count, serum calcium and phosphate levels, parathyroid hormone and 25-hydroxyvitamin D levels and thyroid function. Gonadal hormones, serum protein electrophoresis, 24-hour urinary calcium excretion and antitransglutaminase antibodies may also be helpful (Table 1).
{kind=link}
Treatment
Early recognition and screening
Early recognition that patients with chronic disease may have poor bone health is essential. Screening for secondary causes of bone loss, DXA imaging, thoracolumbar x-rays and other targeted investigations will assist in identifying patients at increased risk of fractures. Repeating the DXA is generally recommended every two years, or in 12 months in people with hypogonadism, on prolonged glucocorticoid therapy or with conditions associated with excess glucocorticoid secretion.
Manage the underlying chronic disease
Effective treatment of the underlying disease processes commonly leads to improvements in bone health. For example, adhering to a gluten-free diet in people with coeliac disease and reducing the inflammatory milieu in those with inflammatory bowel disease have been shown to improve BMD. The effect of hormone replacement therapy on BMD in patients with anorexia nervosa is complex and management often requires specialist involvement. Randomised controlled trials with use of the oral contraceptive pill (containing 35 µg ethinyloestradiol) have not been shown to be effective in improving BMD; 51,52 however, transdermal oestrogen (100 µg 17-β oestradiol) combined with cyclical progesterone was associated with a mild increase in spine and hip BMD.53 Maintenance of a normal body weight is paramount in returning menstrual regularity and restoring BMD.21
Minimise additional risk factors
People with chronic disease who smoke should be strongly encouraged to quit. Physical activity, specifically weight bearing and resistance exercises, show modest improvements in BMD and may reduce falls. Ensuring adequate nutrition and maintenance of a healthy body weight is important. Patients with secondary osteoporosis should aim to have the recommended daily intake of calcium (1300 mg/day in older adults, ideally from dietary sources). Calcium supplements may be used when dietary intake is inadequate (a daily dose of 500 to 600 mg of elemental calcium has been recommended by Osteoporosis Australia).2 Serum vitamin D levels should be replete and kept above 50 nmol/L.
Specific osteoporosis treatment
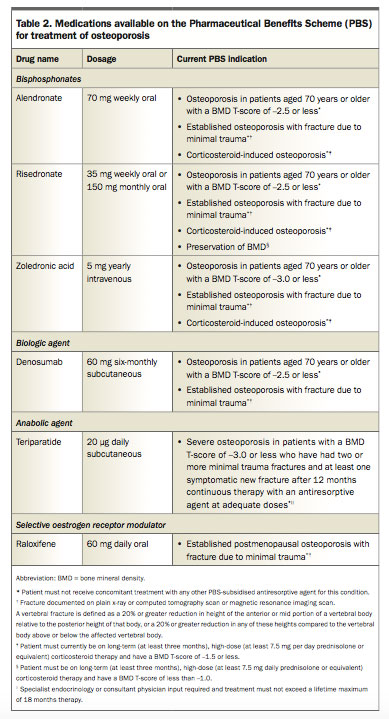
Use of medications (including oral or intravenous bisphosphonates and denosumab) in patients with chronic disease is reserved for those at high risk of fracture. Medications available on the PBS to treat osteoporosis are outlined in Table 2. Treatment should be tailored to the patient’s needs and comorbidities.
{kind=link}
Intervention with bisphosphonates is recommended for patients who require corticosteroids (more than 7.5 mg prednisolone daily or equivalent for more than three months) and have a BMD T-score of -1.5 or less, as there is a higher BMD fracture threshold in these patients. Use of oral bisphosphonates prevents bone loss; however, decreased compliance, malabsorption or gastrointestinal intolerance may favour the use of parenteral antiresorptives in these patients.
Teriparatide may be used in patients with very low BMD who continue to fracture on antiresorptive therapy, with specialist input required for initiation. Some patients may be at high risk of fracture but do not qualify for treatment under the PBS criteria, thus the need for pharmacological treatment should also be judged on a case-by-case basis.
Consider specialist referral
Limited evidence-based guidance is available for treating osteoporosis in several groups, including patients with type 1 diabetes, chronic kidney disease (creatinine clearance <30 mL/minute), neurological and haematological diseases, as well as young adults and pregnant women. Such patients require individualised management and specialist input is often recommended. Furthermore, referral of the patient to a specialist may also be appropriate if there is declining BMD or new incident fracture while taking specific osteoporosis treatments.
Conclusion
Osteoporosis and impaired bone health is an unrecognised component of many chronic diseases. Osteoporotic fractures carry a significant morbidity and mortality, and increased awareness, targeted screening and initiation of treatment are essential. ET
References
- Commonwealth of Australia: Australian Institute of Health and Welfare (AIHW). Australian burden of disease study: fatal burden of disease 2010. Canberra: AIHW; 2015. Available online at: http://www.aihw.gov.au/publication-detail/ ?id=60129550176 (accessed June 2017).
- Osteoporosis Australia Medical & Scientific Advisory Committee. Osteoporosis Australia. Available online at: http://www.osteoporosis.org.au/ (accessed June 2017).
- Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int 2006; 17: 1726-1733.
- Ebeling PR, Daly RM, Kerr DA, Kimlin MG. Building healthy bones throughout life: an evidence-informed strategy to prevent osteoporosis in Australia. Med J Aust 2013; 199(7 Suppl): S1.
- Kohrt WM, Bloomfield SA, Little KD, Nelson ME, Yingling VR. Physical activity and bone health. Med Sci Sports Exerc 2004; 36: 1985-1996.
- Seeman E. Pathogenesis of bone fragility in women and men. Lancet 2002; 359: 1841-1850.
- Manolagas SC, Kousteni S, Jilka RL. Sex steroids and bone. Recent Prog Horm Res 2002; 57: 385-409.
- Weinstein RS. Glucocorticoid-induced bone disease. N Engl J Med 2011; 365: 62-70.
- Fasano A, Catassi C. Celiac disease. N Engl J Med 2012; 367: 2419-2426.
- Mustalahti K, Catassi C, Reunanen A, et al. The prevalence of celiac disease in Europe: results of a centralized, international mass screening project. Ann Med 2010; 42: 587-595.
- Dubé C, Rostom A, Sy R, et al. The prevalence of celiac disease in average-risk and at-risk Western European populations: a systematic review. Gastroenterology 2005; 128 (4 Suppl 1).
- Zanchetta MB, Longobardi V, Bai JC. Bone and celiac disease. Curr Osteoporos Rep 2016; 14: 43-48.
- Heikkila K, Pearce J, Maki M, Kaukinen K. Celiac disease and bone fractures: a systematic review and meta-analysis. J Clin Endocrinol Metab 2015; 100: 25-34.
- Corazza GR, Di Sario A, Cecchetti L, et al. Bone mass and metabolism in patients with celiac disease. Gastroenterology 1995; 109: 122-128.
- Targownik LE, Bernstein CN, Leslie WD. Risk factors and management of osteoporosis in inflammatory bowel disease. Curr Opin Gastroenterol 2014; 30: 168-174.
- Krajcovicova A, Hlavaty T, Killinger Z, et al. Combination therapy with an immunomodulator and anti-TNFα agent improves bone mineral density in IBD patients. J Crohns Colitis 2014; 8: 1693-1701.
- van Hogezand RA, Hamdy NA. Skeletal morbidity in inflammatory bowel disease. Scand J Gastroenterol Suppl 2006; 59-64.
- Diamond T, Stiel D, Lunzer M, Wilkinson M, Roche J, Posen S. Osteoporosis and skeletal fractures in chronic liver disease. Gut 1990; 31: 82-87.
- Younossi ZM, Stepanova M, Afendy M, et al. Changes in the prevalence of the most common causes of chronic liver diseases in the United States from 1988 to 2008. Clin Gastroenterol Hepatol 2011; 9: 524-530. e1.
- Collier J. Bone disorders in chronic liver disease. Hepatology 2007; 46: 1271-1278.
- Schorr M, Miller KK. The endocrine manifestations of anorexia nervosa: mechanisms and management. Nat Rev Endocrinol 2017; 13: 174-186.
- Seeman E, Szmukler GI, Formica C, Tsalamandris C, Mestrovic R. Osteoporosis in anorexia nervosa: the influence of peak bone density, bone loss, oral contraceptive use, and exercise. J Bone Miner Res 1992; 7: 1467-1474.
- Misra M, Klibanski A. Endocrine consequences of anorexia nervosa. Lancet Diabetes Endocrinol 2014; 2: 581-592.
- Fichter MM, Quadflieg N, Hedlund S. Twelve-year course and outcome predictors of anorexia nervosa. Int J Eat Disord 2006; 39: 87-100.
- Vestergaard P, Mosekilde L. Hyperthyroidism, bone mineral, and fracture risk – a meta-analysis. Thyroid 2003; 13: 585-593.
- Mosekilde L, Eriksen EF, Charles P. Effects of thyroid hormones on bone and mineral metabolism. Endocrinol Metab Clin North Am 1990; 19: 35-63.
- Grant DJ, McMurdo ME, Mole PA, Paterson CR. Is previous hyperthyroidism still a risk factor for osteoporosis in post-menopausal women? Clin Endocrinol (Oxf) 1995; 43: 339-345.
- Rosen CJ, Adler RA. Longitudinal changes in lumbar bone density among thyrotoxic patients after attainment of euthyroidism. J Clin Endocrinol Metab 1992; 75: 1531-1534.
- Vestergaard P. Discrepancies in bone mineral density and fracture risk in patients with type 1 and type 2 diabetes--a meta-analysis. Osteoporos Int 2007; 18: 427-444.
- Vestergaard P. Diabetes and bone fracture: risk factors for old and young. Diabetologia 2014; 57: 2007-2008.
- Burghardt AJ, Issever AS, Schwartz AV, et al. High-resolution peripheral quantitative computed tomographic imaging of cortical and trabecular bone microarchitecture in patients with type 2 diabetes mellitus. J Clin Endocrinol Metab 2010; 95: 5045-5055.
- Patsch JM, Burghardt AJ, Yap SP, et al. Increased cortical porosity in type 2 diabetic postmenopausal women with fragility fractures. J Bone Miner Res 2013; 28: 313-324.
- Ma L, Oei L, Jiang L, et al. Association between bone mineral density and type 2 diabetes mellitus: a meta-analysis of observational studies. Eur J Epidemiol 2012; 27: 319-332.
- Ivers RQ, Cumming RG, Mitchell P, Peduto AJ, Blue Mountains Eye Study. Diabetes and risk of fracture: The Blue Mountains Eye Study. Diabetes Care 2001; 24: 1198-1203.
- Strotmeyer ES, Cauley JA, Schwartz AV, et al. Nontraumatic fracture risk with diabetes mellitus and impaired fasting glucose in older white and black adults: The health, aging, and body composition study. Arch Intern Med 2005; 165: 1612-1617.
- Australian Bureau of Statistics (ABS). Australian Health Survey: biomedical results for chronic diseases, 2011-12. Canberra: ABS; 2013. Available online at: http://www.abs.gov.au/ausstats/[email protected] Lookup/4364.0.55.005 main+features12011-12 (accessed June 2017).
- Moe SM, Drüeke TB, Block GA, et al. Group Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int Suppl 2009: S1-130.
- Ball AM, Gillen DL, Sherrard D, et al. Risk of hip fracture among dialysis and renal transplant recipients. JAMA 2002; 288: 3014-3018.
- Moe SM, Nickolas TL. Fractures in patients with CKD: time for action. Clin J Am Soc Nephrol 2016; 11: 1929-1931.
- West SL, Lok CE, Langsetmo L, et al. Bone mineral density predicts fractures in chronic kidney disease. J Bone Miner Res 2015; 30: 913-919.
- Canalis E, Mazziotti G, Giustina A, Bilezikian JP. Glucocorticoid-induced osteoporosis: pathophysiology and therapy. Osteoporos Int 2007; 18: 1319-1328.
- Van Staa TP, Leufkens HG, Abenhaim L, Zhang B, Cooper C. Use of oral corticosteroids and risk of fractures. J Bone Miner Res 2000; 15: 993-1000.
- Vestergaard P. Epilepsy, osteoporosis and fracture risk - a meta-analysis. Acta Neurol Scand 2005; 112: 277-286.
- Valsamis HA, Arora SK, Labban B, McFarlane SI. Antiepileptic drugs and bone metabolism. Nutr Metab 2006; 3: 36.
- Yu EW, Bauer SR, Bain PA, Bauer DC. Proton pump inhibitors and risk of fractures: a meta-analysis of 11 international studies. Am J Med 2011; 124: 519-526.
- Geisler J, Lonning PE. Endocrine effects of aromatase inhibitors and inactivators in vivo: review of data and method limitations. J Steroid Biochem Mol Biol 2005; 95: 75-81.
- Coleman RE, Banks LM, Girgis SI, et al. Skeletal effects of exemestane on bone-mineral density, bone biomarkers, and fracture incidence in postmenopausal women with early breast cancer participating in the Intergroup Exemestane Study (IES): a randomised controlled study. Lancet Oncol 2007; 8: 119-127.
- Howell A, Cuzick J, Baum M, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet 2005; 365: 60-62.
- Amir E, Seruga B, Niraula S, Carlsson L, Ocana A. Toxicity of adjuvant endocrine therapy in postmenopausal breast cancer patients: a systematic review and meta-analysis. J Natl Cancer Inst 2011; 103: 1299-1309.
- Cheung AS, Zajac JD, Grossmann M. Muscle and bone effects of androgen deprivation therapy: current and emerging therapies. Endocr Relat Cancer 2014; 21: R371-R394.
- Grinspoon S, Thomas L, Miller K, Herzog D, Klibanski A. Effects of recombinant human IGF-I and oral contraceptive administration on bone density in anorexia nervosa. J Clin Endocrinol Metab 2002; 87: 2883-2891.
- Strokosch GR, Friedman AJ, Wu SC, Kamin M. Effects of an oral contraceptive (norgestimate/ethinyl estradiol) on bone mineral density in adolescent females with anorexia nervosa: a double-blind, placebo-controlled study. J Adolesc Health 2006; 39: 819-827.
- Misra M, Katzman D, Miller KK, et al. Physiologic estrogen replacement increases bone density in adolescent girls with anorexia nervosa. J Bone Miner Res 2011; 26: 2430-2438.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.