A clinical approach to managing obesity in adults

Obesity is a complex chronic disease that is strongly associated with an increased risk of all-cause mortality. Therapies for managing obesity should be guided by an individual’s body mass index, comorbidities and the presence and severity of obesity-related complications.
- Obesity is a complex chronic disease associated with increased morbidity and mortality.
- Routine screening is required to assess the complications of obesity.
- Preconception counselling is crucial as many women are unaware of the potential adverse effects of obesity on both maternal and offspring outcomes.
- Even small reductions in body weight can reduce the complications of obesity.
- For many individuals, lifestyle interventions alone will not achieve the required amount of weight loss and pharmacotherapy with or without metabolic surgery should be considered.
What are the health risks from obesity?
Obesity is a complex chronic disease that is strongly associated with an increased risk of all-cause mortality.1-3 Importantly, the longer the duration of obesity, the greater its impact on mortality, which is an important consideration in young adults with obesity.4
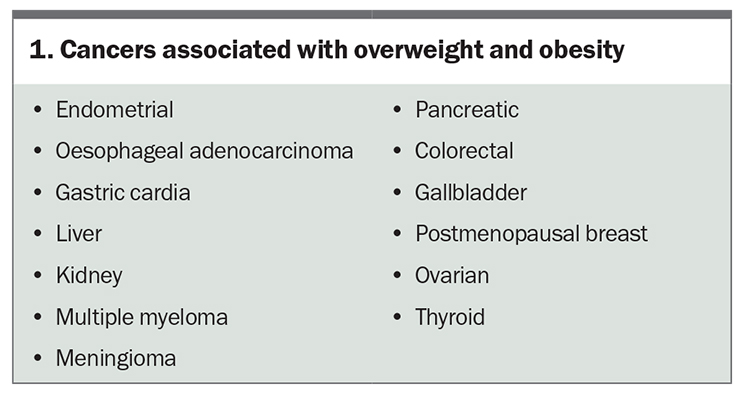
Excess weight is directly linked to various cardiovascular risk factors. As body mass index (BMI) increases, so do blood pressure and low-density lipoprotein (LDL), triglyceride and fasting blood glucose levels.5-7 This results in an increased risk of various diseases such as type 2 diabetes, cardiovascular disease (CVD), chronic kidney disease and metabolic-associated fatty liver disease.8-11 The burden of carrying excess body weight may result in mechanical complications including obstructive sleep apnoea, urinary incontinence, osteoarthritis and low back pain.8,12,13 Obesity is a state of chronic low-grade inflammation and is a major risk factor for at least 13 different types of cancer (Box 1) and dementia.14,15
{kind=link}
In women of reproductive age, obesity is associated with menstrual disturbance, impairment of oocyte development and quality, anovulation, delayed conception, as well as worsening of the clinical presentation of PCOS.16,17 Depression is almost twice as common in people with obesity than in those who have a healthy weight, although the direction of causality is not clear.18,19 Women tend to experience more mental health complications associated with obesity than men, and this gender disparity is likely due to complex societal factors underlying weight stigma.20 Weight stigma can lead to a strong dissatisfaction with one’s bodyweight and/or shape, which is a risk factor for the development of comorbid disordered eating behaviours.20 The resulting mental health impact of weight stigmatisation can drive further weight gain and the development of other chronic diseases.21
Why is weight loss important?
Weight loss is important as even small reductions in body weight reduce the complications of obesity. Weight loss of 5% of the total body weight can prevent the development of type 2 diabetes in individuals with prediabetes, leads to improvement in blood glucose management in individuals with type 2 diabetes, reduces liver fat, results in improvements in systolic blood pressure and triglyceride levels, and improves physical disability in patients with knee osteoarthritis.20-25 Greater weight loss of 10% or more can result in additional health benefits including remission of type 2 diabetes, improvements in obstructive sleep apnoea, reductions in liver inflammation and injury, and a lower risk of cardiovascular events and mortality.22-26 In women with PCOS, lifestyle interventions improve hyperandrogenism even if weight loss is minimal, although greater weight loss from metabolic surgery also results in improved menstrual regularity and can result in disease remission.17,27
In women with obesity and subfertility, lifestyle interventions have a positive effect on pregnancy and natural conception rates, whereas it is unclear whether it improves the live birth rate.28 Weight management approaches, including medically supervised low (4200 to 5000 kJ) and very low (<3300 kJ) energy diets in combination with behavioural weight loss therapy, do not induce binge eating in overweight adults without pretreatment binge eating, and can reduce binge eating in those with pretreatment binge eating behaviours.29
When and how do you screen for secondary causes of obesity?
Obesity is a chronic and complex disease contributed to by many factors including a genetic predisposition to obesity, work and social environments that promote the consumption of convenient highly-processed foods and sedentary behaviour, metabolic adaptations defending against weight loss, as well as other psychosocial and economic drivers.30 For most individuals, their risk for obesity will be conferred by numerous variants in several genetic drivers, that is, polygenic obesity. However, screening for rare monogenic subtypes of obesity should be considered if extreme obesity occurs at a young age (under 5 years) together with clinical features of genetic obesity syndromes (in particular extreme hyperphagia) and/or a family history of extreme obesity.31
A relatively sudden increase in weight may suggest an endocrine cause for obesity, and screening for causes such as hypothyroidism and Cushing’s syndrome (including iatrogenic cortisol excess from exogenous glucocorticoid use) should be considered, particularly if suggestive clinical features are present. For example, if the patient reports dry skin, cold intolerance or other features to suggest hypothyroidism, check the thyroid stimulating hormone level. If there are clinical features of Cushing’s syndrome (e.g. easy bruising, facial plethora, proximal myopathy or wide purple striae), measure the midnight salivary cortisol and 24-hour urinary free cortisol levels, or arrange a 1 mg overnight dexamethasone suppression test (the diagnostic approach will depend on the pretest probability). PCOS should be considered if there are clinical features of insulin resistance (acanthosis nigricans), hyperandrogenism (acne and hirsutism) or oligo-ovulation/anovulation (irregular menstrual cycles).
Review the use of medications associated with weight gain, such as antidepressants (e.g. mirtazapine, amitriptyline, sertraline, fluoxetine, paroxetine), antipsychotics (e.g. olanzapine, clozapine, quetiapine, risperidone), anticonvulsants (e.g. valproate, carbamazepine, gabapentin) and therapies for diabetes (e.g. insulin, sulfonylureas and thiazolidinediones), and consider switching to less obesogenic drugs if possible.32 If there is diagnostic uncertainty, consider referral of the patient to a specialist service.
How do you assess for obesity-related complications?
The following routine assessments should be performed in all adults with overweight and obesity:33
- measure weight, height and BMI
- measure waist circumference
- measure blood pressure (using an appropriately sized arm cuff)
- measure fasting glucose levels (repeated every one to three years according to local guidelines34)
- assess fasting lipid profile
- perform liver function tests and calculate nonalcoholic fatty liver disease fibrosis score (see: https://nafldscore.com/)
- screen for mechanical complications, such as osteoarthritis
- screen for obstructive sleep apnoea (e.g. STOP-BANG questionnaire)
- screen for depression and anxiety (e.g. K10 screening tool or Patient Health Questionnaire-9)
- screen for disordered eating (e.g. Eating Disorder Examination Questionnaire)
- screen for CVD (e.g. www.cvdcheck.org.au) in all adults 45 years of age and older (or 30 years and older for Aboriginal and Torres Strait Islander people) without existing CVD or not already known to be at increased risk of CVD
- encourage age-appropriate cancer screening (e.g. bowel, breast, cervix and prostate)
- screen for clinical signs of hyperandrogenism in women (e.g. hirsutism, acne, male pattern balding).
How do you identify candidates for weight loss interventions?
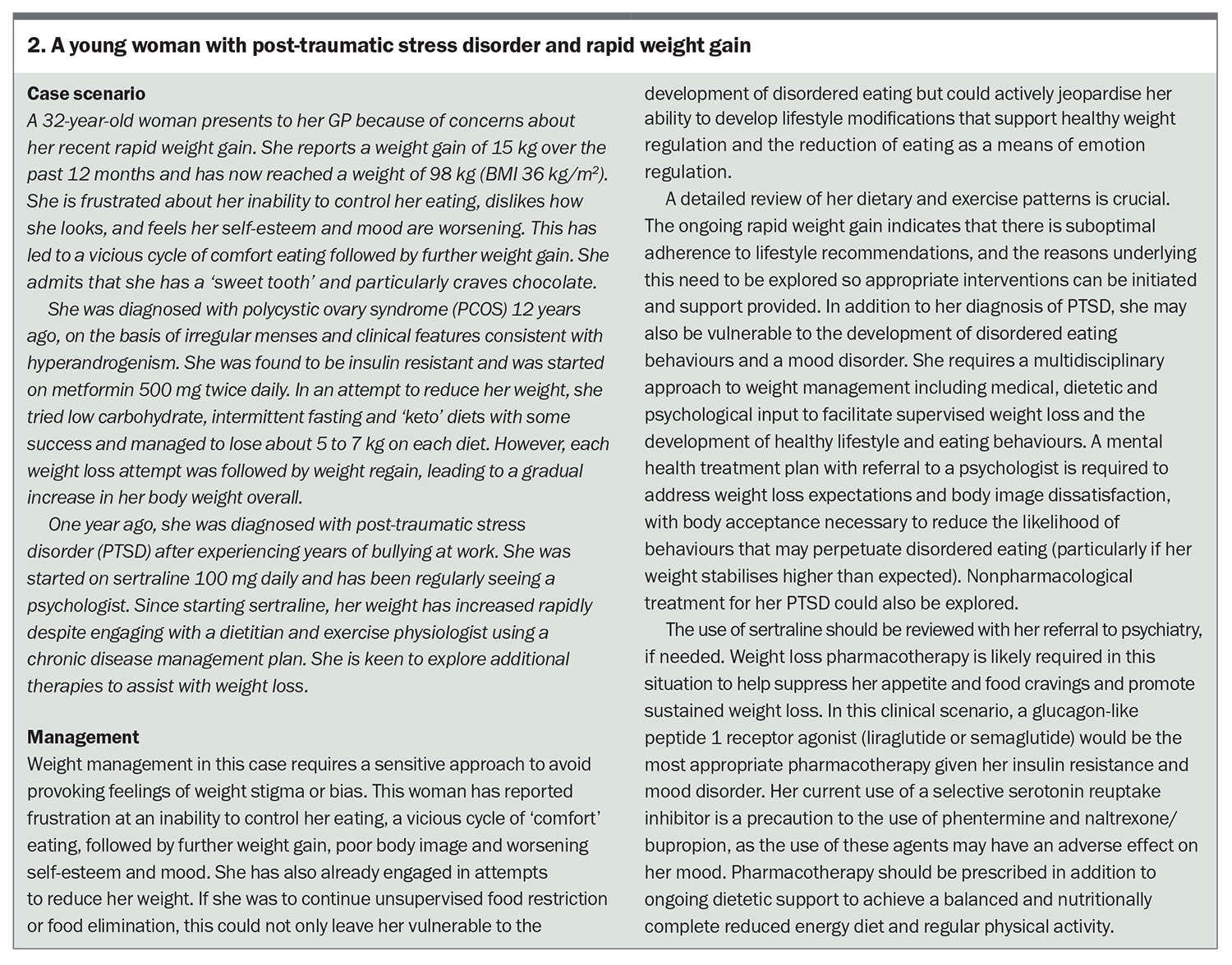
Treatments for obesity should be guided by an individual’s BMI, waist circumference and the presence and severity of obesity-related complications. It is imperative that lifestyle modifications are the basis of all treatment pathways with goals focused on reducing energy intake, optimising diet quality and increasing energy expenditure. Antiobesity pharmacotherapies are indicated for any individual with a BMI of 30 kg/m2 or more, or a BMI 27 kg/m2 or more plus the presence of at least one weight-related complication (see the Case Study in Box 2). Consider starting antiobesity pharmacotherapies if lifestyle modifications alone have been unsuccessful in achieving desired weight loss, or to maintain weight loss and prevent weight regain. Consider metabolic surgery for adults with a BMI of 40 kg/m2 or more, or a BMI of 30.0 to 39.9 kg/m2 with complications that may improve with weight loss.
{kind=link}
Special considerations in women of childbearing age
Many women planning to conceive are unaware of the potential adverse effects of obesity on both maternal and offspring outcomes. Obesity is associated with reduced fertility and oocyte quality, and also adversely impacts the quality and early development of the embryo.35,36 Obesity is associated with increased risks in the antenatal, intrapartum and postpartum periods, as well as increased anaesthetic risk.37 There is a direct relationship between the class of obesity and the likelihood of serious adverse outcomes for both mother and baby.38 A large retrospective cohort study found that, when compared with normal-weight women, the hazard ratio for stillbirth was 1.36 for overweight women, 1.71 for women with class I obesity, 2.00 for women with class II obesity, 2.48 for women with class III obesity, and 3.16 for women with a BMI of 50 kg/m2 or more.39 Perinatal exposure to maternal obesity is also associated with cardiometabolic morbidity in the offspring.40
Height and weight should be measured and BMI calculated at preconception appointments. The risks of overweight and obesity on fertility and pregnancy outcomes need to be discussed using a sensitive and person-centred approach. The Royal Australian and New Zealand College of Obstetricians and Gynaecologists’ best practice statement on management of obesity in pregnancy recommends starting folate 5 mg daily (due to the increased risk of neural tube defects) and iodine 150 mcg daily (unless contraindicated) in the preconception period for women with obesity.37
Ideally, weight and metabolic health should be optimised before conception to reduce the risk of pregnancy-related complications, and to minimise exposure of the fetus to an adverse metabolic environment. A multifaceted and holistic approach to weight management is best provided by an experienced healthcare team. At present, there is a lack of conclusive randomised trial data regarding the optimal weight loss interventions for pre-pregnancy use.37 Women should be advised to use reliable forms of contraception while working on weight loss, particularly when using antiobesity pharmacotherapy. Medications for weight loss should be avoided during the time of conception and during pregnancy for safety reasons. Women who have undergone metabolic surgery require additional nutritional supplementation and careful monitoring for micronutrient deficiencies in the preconception period. It is recommended that conception is avoided for 12 to 18 months following metabolic surgery, particularly when there is rapid weight loss or nutritional deficiencies.
Lifestyle interventions and the role of behaviour therapy
Lifestyle interventions to reduce energy intake, increase energy expenditure and improve nutritional quality are the cornerstone of weight management. A network of experienced clinicians providing support and supervision is key to the success of lifestyle interventions and can be funded using a chronic disease management plan, mental health treatment plan or eating disorder treatment and management plan, if appropriate. Behaviour therapy is key to helping people make long-term changes in the way they respond to stimuli that trigger eating. Behaviour modification programs offered by accredited practising dietitians, psychologists and other suitably experienced clinicians can result in more weight loss and less weight regain.41 If there is any concern for a binge-eating disorder, consider referral of the patient to a healthcare practitioner with expertise in eating disorders.
The Australian Dietary Guidelines and the Australian Guide to Healthy Eating provide general dietary advice.42,43 Options for reducing energy intake include:
- reduced energy diet (RED): modest energy deficit of 2000 to 4000 kJ/day (480 to 960 kcal/day)
- low energy diet (LED): aim to reduce total daily energy intake to 4200 to 5000 kJ (1000 to 1200 kcal)
- very low energy diet (VLED): aim to reduce energy intake to less than 3300 kJ/day (800 kcal/day) by substituting meals with formulated meal replacements. Medical supervision and regular clinical review are required when using VLED in patients with obesity-related complications including type 2 diabetes and chronic kidney disease
- dietary counselling to ensure nutrient quality is maximised.
People with a BMI of 30 to 39.9 kg/m2 and no obesity-related complications could trial RED or LED initially, and then consider VLED if weight loss is inadequate.44 People with a BMI of 30 to 39.9 kg/m2 and obesity-related complications and those with a BMI of 40 kg/m2 or more should generally start VLED.44 Refer to the latest Australian obesity management algorithm for further details, such as contraindications to VLED and the use of VLED in special groups (e.g. in people with chronic kidney disease, diabetes or using warfarin).44
Regular physical activity is a key component of weight management (for increasing energy expenditure, maintaining muscle mass and improving cardiovascular health) and exercise programs should be titrated to individual needs. For example, people with musculoskeletal problems may benefit from choosing aquatic activities, and those with cardiovascular or respiratory diseases will likely require a gentler program as tolerated. An exercise physiologist will be able to provide tailored advice on suitable exercise programs for the patient. For general advice on physical activity, please refer to the physical activity and exercise guidelines produced by the Australian Government.45
What pharmacotherapies are available for weight loss?
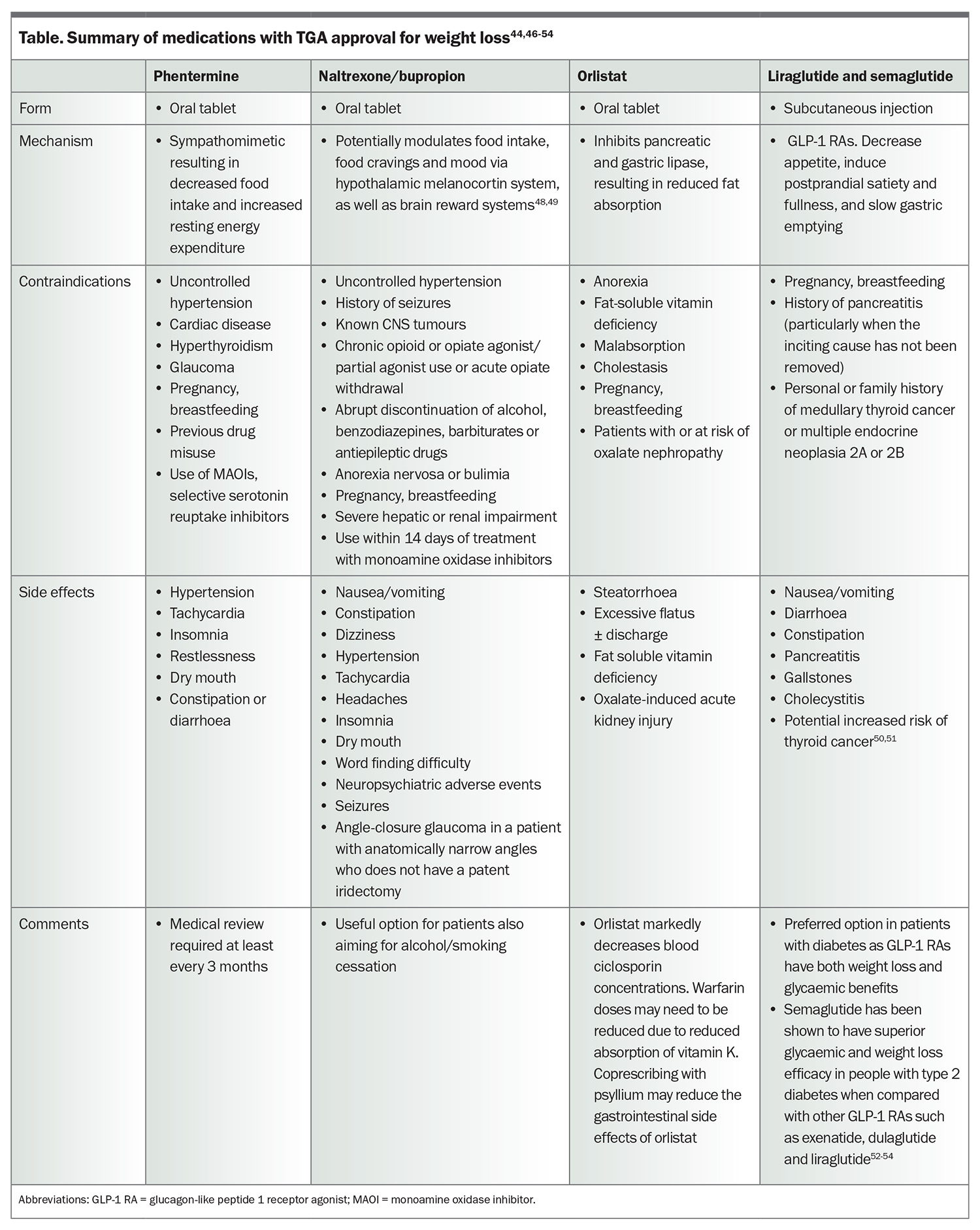
At present, liraglutide, semaglutide, phentermine, naltrexone/bupropion and orlistat are approved by the Therapeutic Goods Administration (TGA) for weight loss. There is a lack of long-term (>5 year) safety data regarding the use of these medications for weight loss. Topiramate and phentermine–topiramate are often used off-label for weight loss but do not currently have TGA approval for this indication. The choice of pharmacotherapy should be based on a careful assessment of factors such as patient age, comorbidities (e.g. diabetes, chronic kidney disease, or liver disease), medication side effect profiles and patient preference (Table).44,46-54 Metformin is a useful adjunct to reduce insulin resistance and menstrual irregularity, and promotes modest weight loss in women with obesity and PCOS.55,56 Metformin is not approved by the TGA as a pharmacotherapy for weight loss.
{kind=link}
What if pharmacotherapy does not result in the required weight loss?
If lifestyle and pharmacotherapy have not resulted in the required weight loss, metabolic surgery can be considered as part of a comprehensive treatment plan. The potential benefits of metabolic surgery should be carefully weighed against the individual risk profile, and close evaluation of mental health and psychosocial factors is crucial. Surgery should ideally be performed in high-volume centres with experienced multidisciplinary teams. After metabolic surgery, patients will require long-term monitoring of micronutrient and nutritional status, as well as ongoing review of lifestyle and psychological factors.
The latest Australian obesity management algorithm states that metabolic surgery should be considered if target weight loss is not achieved with VLED with or without pharmacotherapy, and either a BMI of 40 kg/m2 or more, or a BMI of 30 to 39.9 kg/m2 and the presence of obesity-related complications.44 Ethnicities such as South Asian, East Asian, South-East Asian, Australian Aboriginal and Torres Straight Islanders have been shown to have higher adiposity and risk of diabetes for a given BMI.44,57-60 The Australian obesity management algorithm adopts lower BMI cut-offs for these populations, in which a BMI of 27.5 to 37.5 kg/m2 is equivalent to a BMI of 30 to 40 kg/m2, and a BMI above 37.5 kg/m2 is equivalent to BMI above 40 kg/m2.44
The Australian Diabetes Society endorsed the 2nd Diabetes Surgery Summit meeting guidelines, which states that metabolic surgery is recommended for individuals with type 2 diabetes with:61
- BMI of 40 kg/m2 or more regardless of the level of glycaemic control or complexity of glucose-lowering regimens
- BMI of 35.0 to 39.9 kg/m2 with inadequate glycaemic management despite lifestyle and optimal medical therapy.
The American Diabetes Association Standards of Medical Care in Diabetes state that metabolic surgery:62
- should be a recommended option to treat type 2 diabetes in screened surgical candidates with a BMI of 40 kg/m2 or more (BMI ≥37.5 kg/m2 in Asian Americans) and in adults with a BMI of 35.0 to 39.9 kg/m2 (32.5 to 37.4 kg/m2 in Asian Americans) who do not achieve durable weight loss and improvement in comorbidities (including hyperglycaemia) with nonsurgical methods
- may be considered as an option to treat type 2 diabetes in adults with a BMI of 30.0 to 34.9 kg/m2 (27.5 to 32.4 kg/m2 in Asian Americans) who do not achieve durable weight loss and improvement in comorbidities (including hyperglycaemia) with nonsurgical methods.
Summary
Therapies for managing obesity should be guided by an individual’s BMI, comorbidities, and the presence and severity of obesity-related complications. A network of experienced clinicians providing support and supervision is crucial for the success of lifestyle interventions. Patients can access allied health and mental health services via a chronic disease management plan and mental health treatment plan co-ordinated by their GP. If lifestyle and pharmacotherapy have not resulted in the required weight loss, metabolic surgery should be considered as part of a comprehensive treatment plan. ET
COMPETING INTERESTS: None.
References
2. Whitlock G, Lewington S, Sherliker P, et al. Body-mass index and cause-specific mortality in 900 000 adults: collaborative analyses of 57 prospective studies. Lancet 2009; 373: 1083-1096.
3. Chen Y, Copeland WK, Vedanthan R, et al. Association between body mass index and cardiovascular disease mortality in east Asians and south Asians: pooled analysis of prospective data from the Asia Cohort Consortium. BMJ 2013; 347: f5446.
4. Abdullah A, Wolfe R, Stoelwinder JU, et al. The number of years lived with obesity and the risk of all-cause and cause-specific mortality. Int J Epidemiol 2011; 40: 985-996.
5. Menke A, Rust KF, Fradkin J, Cheng YJ, Cowie CC. Associations between trends in race/ethnicity, aging, and body mass index with diabetes prevalence in the United States: a series of cross-sectional studies. Ann Intern Med 2014; 161: 328-335
6. Kotsis V, Stabouli S, Papakatsika S, Rizos Z, Parati G. Mechanisms of obesity- induced hypertension. Hypertens Res 2010; 33: 386-393.
7. Howard BV, Ruotolo G, Robbins DC. Obesity and dyslipidemia. Endocrinol Metab Clin North Am 2003; 32: 855-867.
8. Kopelman PG. Obesity as a medical problem. Nature 2000; 404: 635-643.
9. Wang Y, Chen X, Song Y, Caballero B, Cheskin LJ. Association between obesity and kidney disease: a systematic review and meta-analysis. Kidney Int 2008; 73: 19-33.
10. Fan R, Wang J, Du J. Association between body mass index and fatty liver risk: A dose-response analysis. Sci Rep 2018; 8: 15273.
11. Haase CL, Eriksen KT, Lopes S, Satylganova A, Schnecke V, McEwan P. Body mass index and risk of obesity-related conditions in a cohort of 2.9 million people: evidence from a UK primary care database. Obes Sci Pract 2020; 7: 137-147.
12. Doumouchtsis SK, Loganathan J, Pergialiotis V. The role of obesity on urinary incontinence and anal incontinence in women: a review. BJOG 2022; 129: 162-170.
13. Bliddal H, Leeds AR, Christensen R. Osteoarthritis, obesity and weight loss: evidence, hypotheses and horizons - a scoping review. Obes Rev 2014; 15: 578-586.
14. Lauby-Secretan B, Scoccianti C, Loomis D, et al. Body fatness and cancer-- viewpoint of the IARC Working Group. N Engl J Med 2016; 375: 794-798.
15. Alford S, Patel D, Perakakis N, Mantzoros CS. Obesity as a risk factor for Alzheimer’s disease: weighing the evidence. Obes Rev 2018; 19: 269-280.
16. Best D, Avenell A, Bhattacharya S. How effective are weight-loss interventions for improving fertility in women and men who are overweight or obese? A systematic review and meta-analysis of the evidence. Hum Reprod Update 2017; 23: 681-705.
17. Lim SS, Hutchison SK, Van Ryswyk E, Norman RJ, Teede HJ, Moran LJ. Lifestyle changes in women with polycystic ovary syndrome. Cochrane Database Syst Rev 2019; 3: CD007506.
18. Pi-Sunyer X. The medical risks of obesity. Postgrad Med 2009; 121: 21-33.
19. Roberts RE, Kaplan GA, Shema SJ, Strawbridge WJ. Are the obese at greater risk for depression? Am J Epidemiol 2000; 152: 163-170.
20. Tronieri JS, Wurst CM, Pearl RL, Allison KC. Sex differences in obesity and mental health. Curr Psychiatry Rep 2017; 19: 29.
21. Tomiyama AJ, Carr D, Granberg EM, et al. How and why weight stigma drives the obesity ‘epidemic’ and harms health. BMC Med 2018; 16: 123.
22. Lean ME, Leslie WS, Barnes AC, et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): an open-label, cluster-randomised trial. Lancet 2018; 391: 541-551.
23. Schauer PR, Bhatt DL, Kirwan JP, et al. Bariatric surgery versus intensive medical therapy for diabetes - 5-year outcomes. N Engl J Med 2017; 376: 641-651.
24. Promrat K, Kleiner DE, Niemeier HM, et al. Randomized controlled trial testing the effects of weight loss on nonalcoholic steatohepatitis. Hepatology 2010; 51: 121-29.
25. Look ARG, Gregg EW, Jakicic JM, et al. Association of the magnitude of weight loss and changes in physical fitness with long-term cardiovascular disease outcomes in overweight or obese people with type 2 diabetes: a post-hoc analysis of the Look AHEAD randomised clinical trial. Lancet Diabetes Endocrinol 2016; 4: 913-921.
26. Foster GD, Borradaile KE, Sanders MH, et al. A randomized study on the effect of weight loss on obstructive sleep apnea among obese patients with type 2 diabetes: the Sleep AHEAD study. Arch Intern Med 2009; 169: 1619-1626.
27. Skubleny D, Switzer NJ, Gill RS, et al. The impact of bariatric surgery on polycystic ovary syndrome: a systematic review and meta-analysis. Obes Surg 2016; 26: 169-176.
28. Kim SY, Park ES, Kim HW. Effectiveness of non-pharmacological interventions for overweight or obese infertile women: a systematic review and meta-analysis. Int J Environ Res Public Health 2020; 17.
29. da Luz FQ, Hay P, Gibson AA, et al. Does severe dietary energy restriction increase binge eating in overweight or obese individuals? A systematic review. Obes Rev 2015;16: 652-665.
30. Hruby A, Hu FB. The epidemiology of obesity: a big picture. Pharmacoeconomics 2015; 33: 673-689.
31. Styne DM, Arslanian SA, Connor EL, et al. Pediatric obesity - assessment, treatment, and prevention: an Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2017; 102: 709-757.
32. van der Valk ES, van den Akker ELT, Savas M, et al. A comprehensive diagnostic approach to detect underlying causes of obesity in adults. Obes Rev 2019; 20: 795-804.
33. Bessell E, Markovic TP, Fuller NR. How to provide a structured clinical assessment of a patient with overweight or obesity. Diabetes Obes Metab 2021; 23 Suppl 1: 36-49.
34. Bell K, Shaw JE, Maple-Brown L, et al. A position statement on screening and management of prediabetes in adults in primary care in Australia. Diabetes Res Clin Pract 2020; 164: 108188.
35. Snider AP, Wood JR. Obesity induces ovarian inflammation and reduces oocyte quality. Reproduction 2019; 158: R79-R90.
36. Purcell SH, Moley KH. The impact of obesity on egg quality. J Assist Reprod Genet 2011; 28: 517-524.
37. Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Best practice statement Management of Obesity in Pregnancy. March 2022. Available online at: https://ranzcog.edu.au/wp-content/uploads/2022/05/Management-of-Obesity-in-Pregnancy.pdf (accessed January 2023).
38. Catalano PM, Shankar K. Obesity and pregnancy: mechanisms of short term and long term adverse consequences for mother and child. BMJ 2017; 356: j1.
39. Yao R, Ananth CV, Park BY, Pereira L, Plante LA. Obesity and the risk of stillbirth: a population-based cohort study. Am J Obstet Gynecol 2014; 210: 457.e1-9.
40. Kislal S, Shook LL, Edlow AG. Perinatal exposure to maternal obesity: lasting cardiometabolic impact on offspring. Prenat Diagn 2020; 40: 1109-1125.
41. LeBlanc ES, Patnode CD, Webber EM, Redmond N, Rushkin M, O’Connor EA. Behavioral and pharmacotherapy weight loss interventions to prevent obesity- related morbidity and mortality in adults: updated evidence report and systematic review for the US preventive services task force. JAMA 2018; 320: 1172-1191.
42. National Health and Medical Research Council. Australian Dietary Guidelines. Canberra: National Health and Medical Research Council; 2013.
43. National Health and Medical Research Council. Australian Guide to Healthy Eating, 2013. Available online at: http://www.eatforhealth.gov.au/guidelines/australian-guide-healthy-eating (accessed January 2023).
44. Markovic TP, Proietto J, Dixon JB, et al. The Australian Obesity Management Algorithm: a simple tool to guide the management of obesity in primary care. Obes Res Clin Pract 2022. 16: 353-363.
45. Australian Government. Physical activity and exercise guidelines for adults (18 to 64 years), 2021. Available online at: https://www.health.gov.au/health-topics/physical-activity-and-exercise/physical-activity-and-exercise-guidelines-for-all-australians/for-adults-18-to-64-years (accessed January 2023).
46. Müller TD, Blüher M, Tschöp MH, DiMarchi RD. Anti-obesity drug discovery: advances and challenges. Nat Rev Drug Discov 2022; 21: 201-223.
47. Garvey WT, Mechanick JI, Brett EM, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Comprehensive Clinical Practice Guidelines for Medical Care of Patients with Obesity. Endocr Pract 2016; 22 Suppl 3: 1-203.
48. Billes SK, Sinnayah P, Cowley MA. Naltrexone/bupropion for obesity: an investigational combination pharmacotherapy for weight loss. Pharmacol Res 2014; 84: 1-11.
49. Billes SK, Greenway FL. Combination therapy with naltrexone and bupropion for obesity. Expert Opin Pharmacother 2011; 12: 1813-1826.
50. Bezin J, Gouverneur A, Pénichon M, et al. GLP-1 receptor agonists and the risk of thyroid cancer. Diabetes Care. 2022: dc221148.
51. Thompson CA, Stürmer T. Putting GLP-1 RAs and thyroid cancer in context: additional evidence and remaining doubts. Diabetes Care 2022: dci220052.
52. Capehorn MS, Catarig AM, Furberg JK, et al. Efficacy and safety of once-weekly semaglutide 1.0mg vs once-daily liraglutide 1.2mg as add-on to 1-3 oral antidiabetic drugs in subjects with type 2 diabetes (SUSTAIN 10). Diabetes Metab 2020; 46: 100-109.
53. Pratley RE, Aroda VR, Lingvay I, et al; SUSTAIN 7 investigators. Semaglutide versus dulaglutide once weekly in patients with type 2 diabetes (SUSTAIN 7): a randomised, open-label, phase 3b trial. Lancet Diabetes Endocrinol 2018; 6: 275-286.
54. Ahmann AJ, Capehorn M, Charpentier G, et al. Efficacy and safety of once- weekly semaglutide versus exenatide ER in subjects with type 2 diabetes (SUSTAIN 3): A 56-week, open-label, randomized clinical trial. Diabetes Care 2018; 41: 258-266.
55. Harborne LR, Sattar N, Norman JE, Fleming R. Metformin and weight loss in obese women with polycystic ovary syndrome: comparison of doses. J Clin Endocrinol Metab 2005; 90: 4593-4598.
56. Jensterle M, Kravos NA, Ferjan S, Goricar K, Dolzan V, Janez A. Long-term efficacy of metformin in overweight-obese PCOS: longitudinal follow-up of retrospective cohort. Endocr Connect 2020; 9: 44-54.
57. Caleyachetty R, Barber TM, Mohammed NI, et al. Ethnicity-specific BMI cutoffs for obesity based on type 2 diabetes risk in England: a population-based cohort study. Lancet Diabetes Endocrinol 2021; 9: 419-426.
58. Deurenberg P, Yap M, van Staveren WA. Body mass index and percent body fat: a meta analysis among different ethnic groups. Int J Obes Relat Metab Disord 1998; 22: 1164-1171.
59. Razak F, Anand SS, Shannon H, et al. Defining obesity cut points in a multiethnic population. Circulation 2007; 115: 2111-2118.
60. Hsu WC, Araneta MR, Kanaya AM, Chiang JL, Fujimoto W. BMI cut points to identify at-risk Asian Americans for type 2 diabetes screening. Diabetes Care 2015; 38: 150-158.
61. Rubino F, Nathan DM, Eckel RH, et al. Metabolic Surgery in the Treatment Algorithm for Type 2 Diabetes: a joint statement by international diabetes organizations. Diabetes Care 2016; 39: 861-877.
62. American Diabetes Association. Obesity management for the treatment of type 2 diabetes: Standards of Medical Care in Diabetes – 2021. Diabetes Care 2020; 44: S100-S110.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.