How to investigate weight gain in an adult. ‘I’ve put on so much weight, doc’

Obesity
Weight control
Case scenarios are used in this section to educate doctors on the best approach to the diagnosis and management of patients with different endocrine problems. The appropriate selection of tests and correct interpretation of test results are discussed.
Weight, energy intake and expenditure are regulated by a complex integration of neurological, endocrine and gastrointestinal feedback mechanisms. They can also be influenced by psychological state, physical impairment, chronic disease, endocrinopathies and medications. Although genetics, development, promotion of sedentary lifestyles and easy access to energy-dense food are factors, adults with massive weight gain invariably have excess energy intake, and this is proportional to their weight.5-8 Patients are often embarrassed to disclose their complete dietary history or are genuinely unaware of how much energy they are consuming, in which case they believe their weight gain is caused by a lack of physical activity. Many also believe that short periods of exercise negate any increase in energy intake, and so cannot understand why they are putting on weight.
Although this article discusses the challenges in managing patients with massive weight gain with resultant morbid obesity, it is still relevant to the assessment of patients presenting to their primary care physicians with modest weight gain (i.e. 5 to 10 kg).
Case scenario
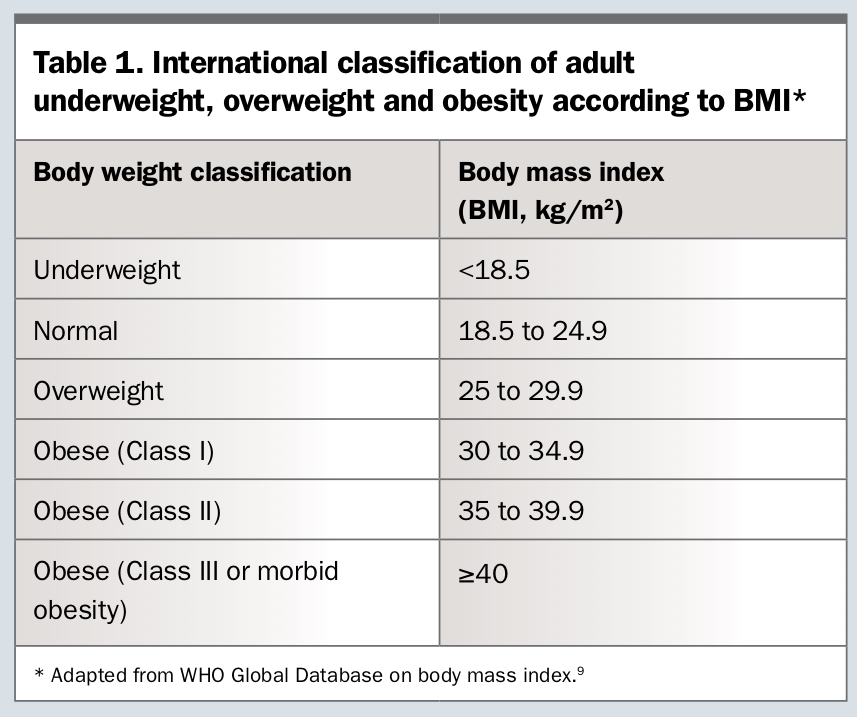
Virginia, a 64-year-old woman presents to her general practitioner with progressive weight gain spanning two decades. She is severely obese (obese class III, 141.5 kg, body mass index [BMI] 57 kg/m2; Table 1)9 and has obesity-related complications including obstructive sleep apnoea (OSA) requiring continuous positive air pressure (CPAP) treatment, impaired fasting glucose, hypertension (160/90 mmHg), nonalcoholic fatty liver disease on ultrasound, and osteoarthritis affecting her spine, hips and knees. She is a nonsmoker, consumes minimal alcohol and has a family history of obesity (her parents and siblings). She moves with difficulty and requires a forearm support frame when she does house cleaning.
{kind=link}
Virginia would like to lose weight but does not think she can achieve this as she cannot exercise. She believes being unable to exercise has caused her weight gain.
What is the first step in managing this patient?
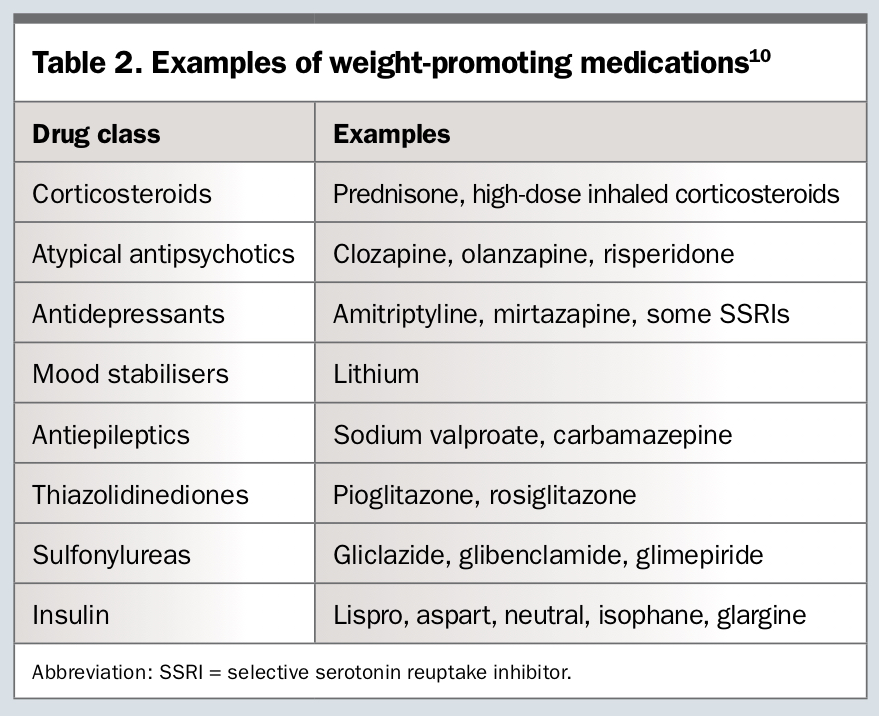
A more detailed history reveals that Virginia takes irbesartan 150 mg daily, amlodipine 5 mg twice a day and mirtazapine 30 mg daily for depression, as well as simple analgesia for osteoarthritis. Use of weight-promoting medications (e.g. mirtazapine) should be sought, and ceased or substituted if possible (Table 2).10
{kind=link}
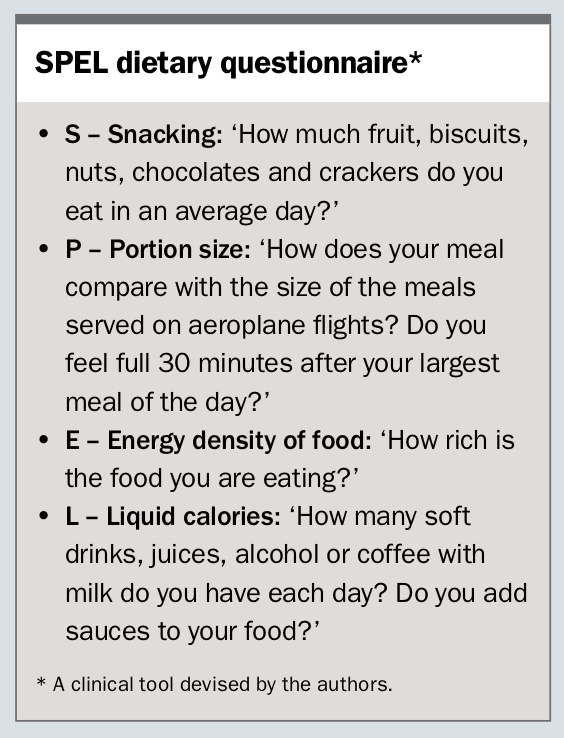
Use of a brief, clinically useful dietary questionnaire developed by the authors (acronym SPEL, see the Box) showed that Virginia consumes large portions as she enjoys feeling ‘full’ and energy dense food as she finds it tasty. She also snacks frequently as she feels it helps with her pain relief. In summary, her weight gain is mainly the result of increased energy consumption coupled with deteriorating mobility.
{kind=link}
What are the key features to assess in the clinical examination?
It is important to weigh patients and measure their height to obtain an accurate BMI, as well as measure their waist circumference. Features of endocrinopathies should be sought (see below). The presence of goitre may alert to contributing thyroid disease but is also important in the setting of OSA.
Examination of the patient’s lower limbs and feet is important as many severely obese patients cannot see or reach their feet. Peripheral oedema, neuropathy tested with monofilament testing if diabetes is present, and vascular disease (e.g. absent peripheral pulses, hair loss or eczema of chronic venous insufficiency) should be documented. Examination for infections in skin folds should also be performed.
What else could be causing this patient’s weight gain?
Endocrinopathies are relatively rare causes of weight gain and, when present, usually amount to about 20 kg in weight gain (Table 3). For example, only a small proportion (<3%) of obese patients with type 2 diabetes will have Cushing’s syndrome so routine screening is not recommended unless more specific features are present (e.g. proximal weakness, easy bruising, wide-purplish abdominal striae, etc.).11 Hypothyroidism rarely leads to massive weight gain and can be easily diagnosed on thyroid function tests.12 Insulinomas can lead to progressive weight gain but are very rare and usually result in recurrent symptomatic hypoglycaemia.
{kind=link}
If an endocrinopathy is suspected, specialist referral is indicated.
What initial investigations are necessary?
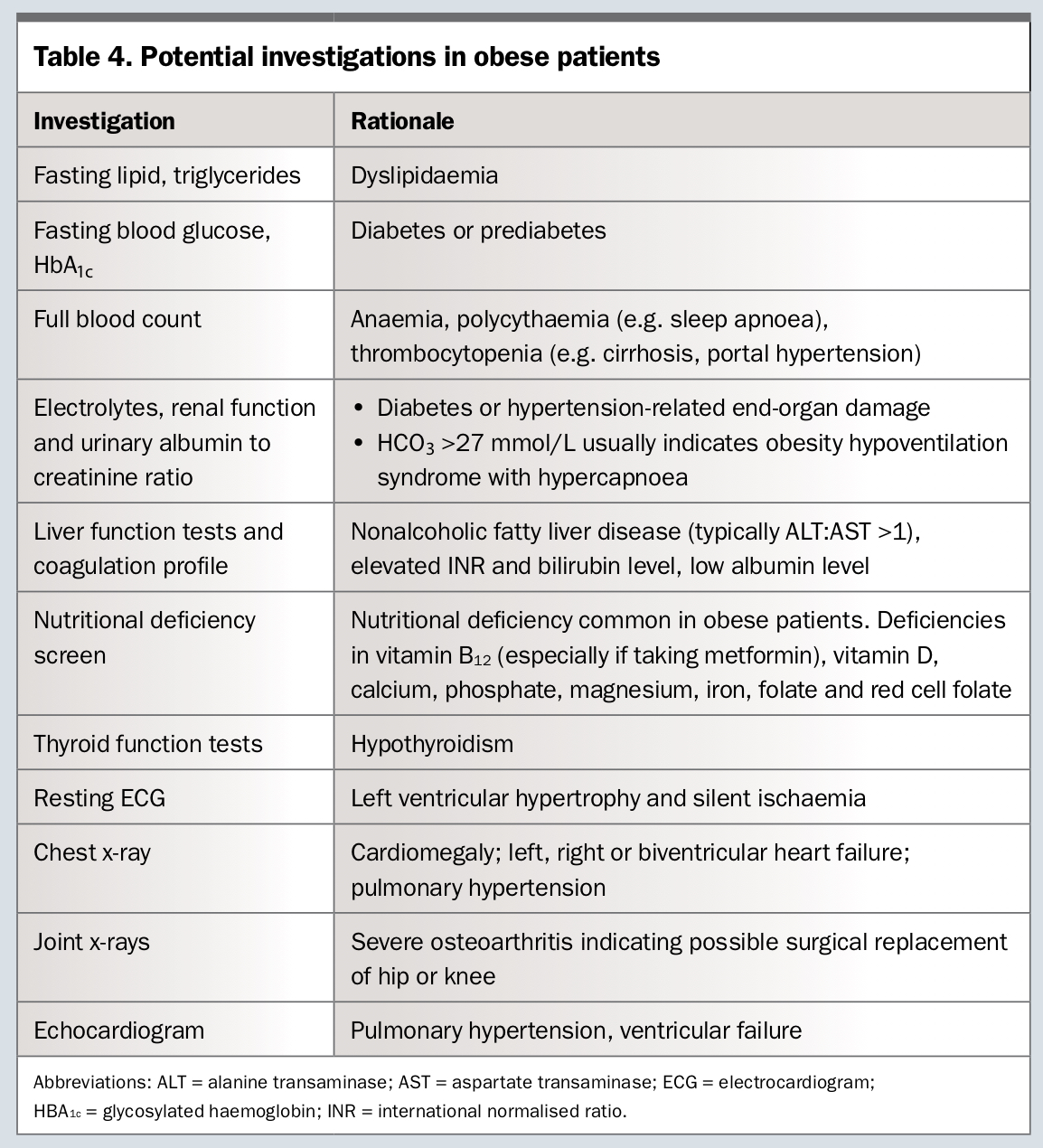
Investigations should be aimed at categorising Virginia’s cardiometabolic risk (e.g. use of the Australian absolute cardiovascular disease risk calculator, www.cvdcheck.org.au) and fitness for exercise, establishing baseline clinical parameters prior to treatment, and assessing for contributing factors to weight gain (Table 4). Undiagnosed OSA and/or obesity hypoventilation syndrome is common in obese patients. Symptoms of OSA (daytime somnolence, drifting asleep while driving or watching TV, waking up unrefreshed) should prompt a referral for a sleep study. Nutritional deficiency is common and vitamin B12 (especially if taking metformin) and vitamin D levels should be assessed and supplemented accordingly.
{kind=link}
What is the best course of action for this patient?
The error most overweight or obese patients and clinicians make is that they believe a lack of exercise is the main problem for the ongoing gain of weight. Experience teaches, however, that ‘You can easily out-eat what you run’. For example, one hour of moderate intensity activity in an obese person equates to approximately 350 kcal (1465 kJ). However, eating energy-dense food equates to an ingestion of an average of 70 kcal every minute (about 300 kJ/minute), and therefore it takes only five minutes of eating this type of food to negate an hour of exercise.
The first step therefore with an overweight or obese patient wanting to lose weight, such as Virginia, is appropriate education regarding their current energy (caloric) intake as well as that required for gradual weight loss. The advice of an experienced dietitian is essential. In general, a negative energy balance of 500 kcal or 1000 kcal each day (about 2100 or 4200 kJ/day, respectively) equates to 0.5 or 1 kg of weight loss per week, respectively. In reality, obese patients will lose much more than this initially because fat, muscle and fluid are lost; weight training exercise should therefore be commenced to preserve muscle bulk and limit bone density loss.
Referral to a physiotherapist or exercise physiologist is the next step, to both prescribe appropriate exercise for the patient and address barriers to activity. Severe osteoarthritis should not preclude exercise. Finally, identification of psychological issues that lead to comfort eating or underlying eating disorders should prompt referral to a clinical psychologist as this intervention takes priority.
Alternatively, Virginia may be referred to a multidisciplinary obesity service, which is available at several major tertiary hospitals. These services may have available all or several of the following staff: dietitian, exercise physiologist, specialist nurse, psychologist and supervising endocrinologist specialising in obesity medicine. A rheumatologist review may be warranted in those patients who may benefit from symptomatic relief with intra-articular corticosteroid injection if simple analgesics are inadequate.
After a period of 12 months, the care team should review the patient. The following should be assessed:
- has the weight loss plateaued despite good application of treatment?
- would the patient benefit from continued weight loss?
- would the patient be compliant with the postoperative requirements of metabolic surgery (previously known as bariatric surgery), such as very low calorie diets, follow-up appointments, exercise?
- are psychological factors related to excess energy intake (e.g. comfort eating, eating disorders) absent or treated?
If the answers to all of the above questions are yes, then a referral to a sugeon specialised in metabolic surgery is warranted, ideally one who participates in the national bariatric surgery registry. The timing and type of surgery are tailored to the patient’s individual goals, and weighed against the risk of postoperative complications.
Conclusion
Excess energy intake, which is often driven by multiple factors, is invariably responsible for longstanding insidious weight gain. A detailed dietary history taken from the patient (or a household cohabitant) in a nonjudgemental fashion using the SPEL dietary questionnaire will, with time, provide the answer. Investigations are not complex and include cardiometabolic and nutritional screens, an assessment for fitness for exercise and possibly, in more complicated patient cases, referral of patients to a multidisciplinary obesity service.
Many patients will, with treatment, be able to lose between 5 and 15% of their initial weight. Metabolic surgery should be considered in patients with persistent obesity-related comorbidities that will likely benefit from further weight loss, as long as their increased energy intake is not primarily caused by a psychological disorder. If the latter is the case, treatment by a clinical psychologist or psychiatrist is the main priority. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.