Bone health in women with premature ovarian insufficiency

Women with premature ovarian insufficiency (POI) have poor bone health and increased susceptibility to fractures due to a combination of oestrogen deficiency and the presence of POI-associated risk factors. Thorough evaluation and management of bone health are necessary to achieve better skeletal outcomes in these women.
- Comprehensive screening and evaluation of bone health should be performed at the diagnosis of premature ovarian insufficiency (POI).
- Multiple mechanisms contribute to skeletal fragility in women with POI. These include oestrogen deficiency, compromised muscle health and presence of POI-associated risk factors.
- Management of bone health requires a multimodal approach, including provision of information, nonpharmacological interventions and use of hormone replacement therapy (HRT) (in the absence of contraindications).
- HRT with oestrogen (and progestogen in women with an intact uterus) should be initiated at the diagnosis of POI unless contraindicated (e.g. in women with hormone-sensitive cancers) and continued until the average age of menopause to maximise bone health, alleviate menopausal symptoms and prevent long-term sequelae, such as cardiovascular disease and cognitive impairment.
- Women with POI should be referred to a specialist if they require pubertal induction, HRT is contraindicated or they have a history of thrombophilia.
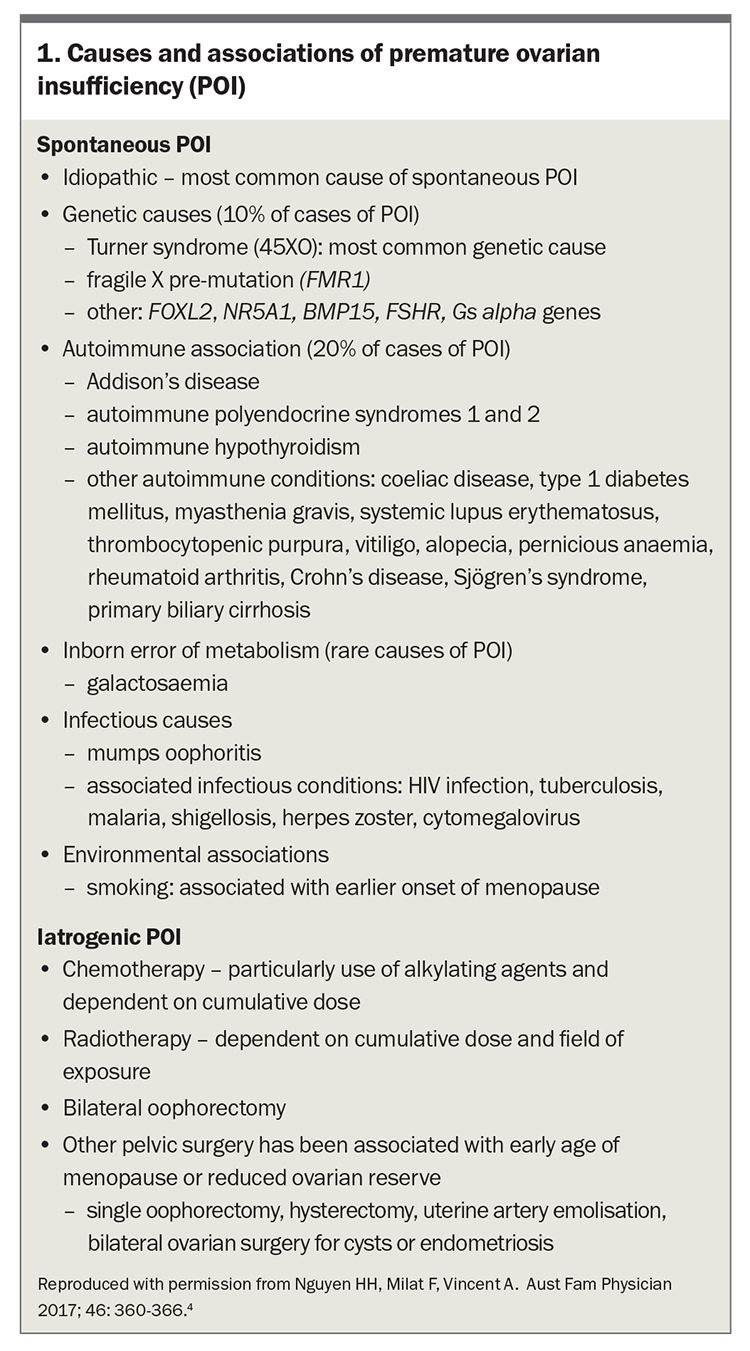
Premature ovarian insufficiency (POI) is the loss of ovarian function before 40 years of age, typically presenting with primary or secondary amenorrhoea or infertility. It is diagnosed by an elevated follicle-stimulating hormone (FSH) level in the menopausal range on two occasions at least four to six weeks apart in a woman under 40 years of age, after more than four months of amenorrhoea or menstrual irregularity. The International Menopause Society guidelines suggest using an FSH level of above 40 IU/L to define the menopausal range, whereas recent guidelines from the European Society of Human Reproduction and Embryology recommend an FSH level above 25 IU/L.1,2 POI affects 3 to 4% of women worldwide and can be broadly classified into spontaneous and iatrogenic categories (Box 1).3,4
{kind=link}
Women with POI experience multiple physical and psychological consequences, including reproductive manifestations, compromised musculoskeletal health, increased cardiometabolic risk and neurocognitive decline. Importantly, bone loss is the most feared complication in women with POI.5 The reported prevalence of osteoporosis in women with POI is between 8 and 15%, and fracture risk is increased up to 1.5 times compared with age-matched premenopausal women.6-9 This article focuses on the assessment and management of bone health in women with POI.
Diagnosis of osteoporosis
Osteoporosis is characterised by low bone mass or impaired bone quality, leading to an increased risk of fracture. It is routinely diagnosed using dual-energy x-ray absorptiometry (DXA)-derived measures of bone mineral density (BMD) in postmenopausal women and men aged over 50 years. Osteoporosis is diagnosed by a BMD that is 2.5 standard deviations or more below that of a young adult population (T-score ≤–2.5), and osteopenia is defined by a T-score between –2.5 and –1.0.
In younger adults, ambiguity exists regarding the definition of osteoporosis based on BMD. According to the International Society of Clinical Densitometry, low bone mass in premenopausal women is defined by an age- and sex-matched BMD Z-score of less than –2.0.10 Other expert groups recommend using a BMD T-score of –2.5 or less to diagnose osteoporosis in women under 50 years of age with chronic disorders known to affect bone metabolism, such as POI.11
Risk factors for osteoporosis in women with POI
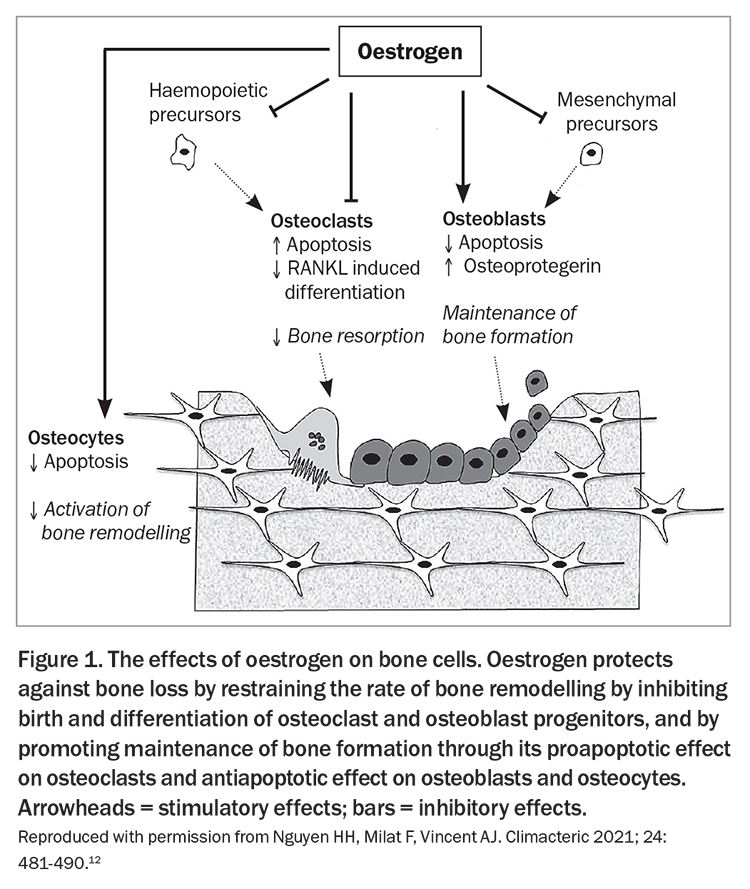
Oestrogen plays a crucial role in defining overall bone structure directly by affecting differentiation, proliferation and activities of various bone cells (Figure 1) and indirectly through its effects on muscle health, leading to an overall increase in bone formation and suppression of bone resorption.12 Women with POI have compromised muscle structure and function because of oestrogen deficiency and factors specific to the underlying cause of POI (such as radiotherapy, glucocorticoid use, nutritional deficiencies), causing defective muscle-bone interaction and mechanical loading leading to bone loss.12,13 Additionally, oestrogen is crucial in bone mass accrual during pubertal development, and hence bone loss can be more pronounced in women with an early age of POI onset (puberty or adolescence) because of insufficient peak bone mass accrual. In adult women with POI, premature bone loss caused by accelerated bone resorption may be the primary mechanism for low BMD.
{kind=link}
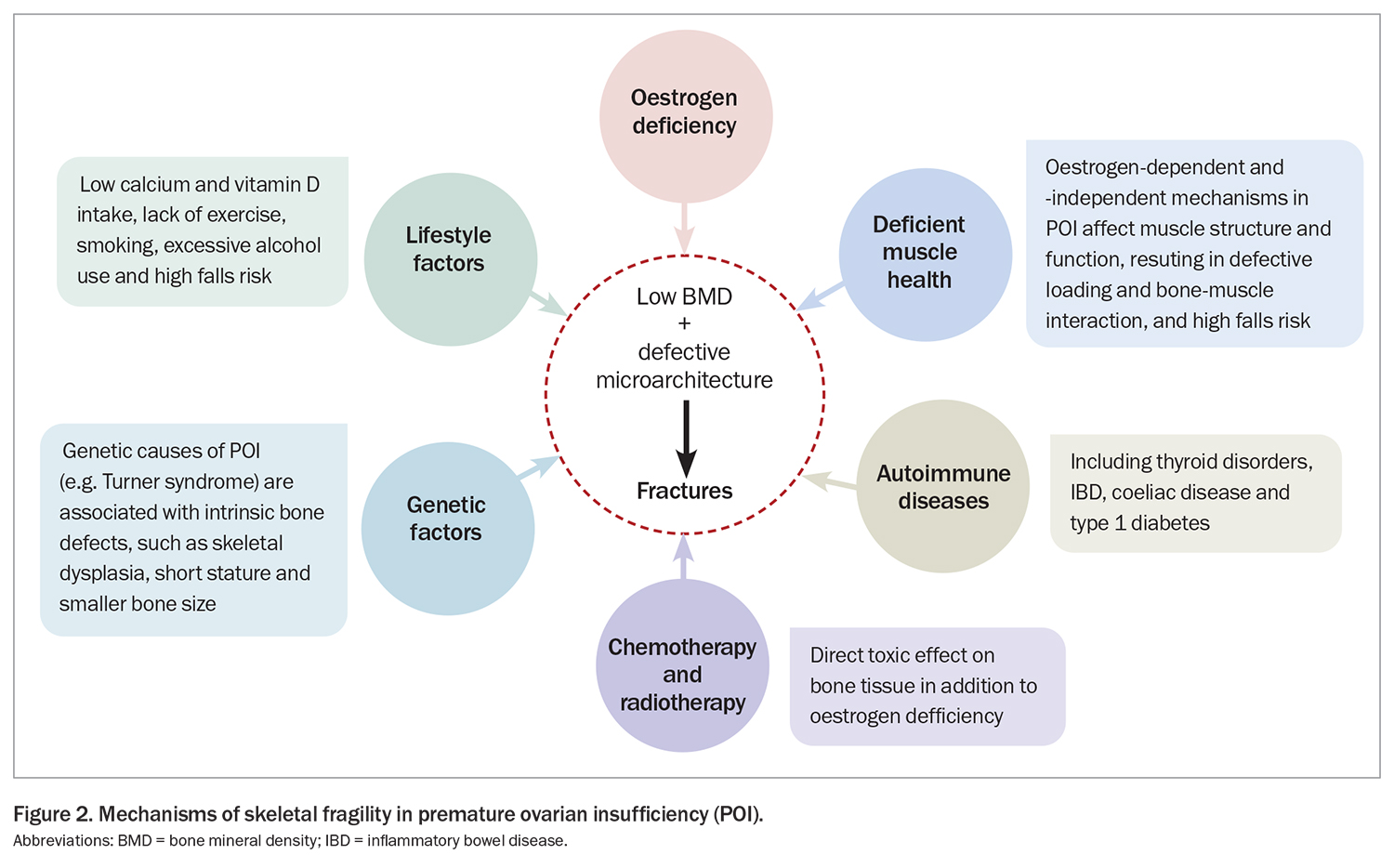
Moreover, autoimmune conditions commonly associated with POI, such as coeliac disease, inflammatory bowel disease, Addison’s disease, type 1 diabetes mellitus and thyroid disorders, as well as chemotherapy- and radiotherapy-associated toxic effects on bone, can have additional detrimental effects on skeletal health (Figure 2).
{kind=link}
In summary, hypoestrogenism is the major risk factor for low bone mass and susceptibility to fractures in women with POI because of decreased bone accrual, failure to attain peak bone mass as well as increased bone loss, leading to an overall decline in bone health. However, other POI-associated risk factors and traditional osteoporosis risk factors may also contribute to bone loss.
Assessment of bone health
Bone health should be assessed at the diagnosis of POI and then monitored during follow up. A detailed clinical assessment is required, followed by investigations such as dual-energy x-ray absorptiometry (DXA) and blood and urine biochemistry (Flowchart).14 Fracture risk assessment tools, such as FRAX that helps determine an individual’s 10-year probability of hip or other major osteoporotic fracture (lumbar spine, humerus or wrist), are not validated for use in women under 40 years of age.
History and examination
Detailed clinical history taking and physical examination should be performed in women with POI, taking into consideration POI-associated risk factors for low bone density, as well as traditional risk factors for osteoporosis (see Flowchart).
Pathology tests
Bone-specific pathology tests, including serum biochemistry tests, measurement of calcium, phosphate and 25-hydroxyvitamin D levels, and liver and renal function tests, should be performed at the initial assessment of women with POI. If there is evidence of a low bone density or history of fractures, consider further biochemical evaluation for other secondary causes of osteoporosis in young adults, such as hyperparathyroidism, coeliac disease and thyroid disorders (Flowchart). Measurement of bone turnover markers, such as C-terminal telopeptide of type 1 collagen and procollagen type I N-propeptide, may be useful in monitoring drug response and adherence to osteoporosis therapies.
Imaging
DXA-derived BMD remains the gold standard for assessing skeletal strength and is widely available, noninvasive and inexpensive. An initial DXA scan is indicated at the initial diagnosis of POI and, if osteoporosis or low bone mass is diagnosed, a repeat DXA scan at two to five years should be considered.
Although DXA-derived BMD strongly correlates with the risk of fracture in older populations, it has limitations in younger women with POI. In women with short stature, delayed bone age or smaller bone size, such as Turner syndrome (the most common genetic cause of POI), DXA underestimates BMD. Moreover, BMD only partly explains skeletal fragility, as a substantial proportion of patients experience fracture despite a normal BMD. Compromised bone microarchitecture can lead to skeletal fragility but is not assessed by routine DXA scans.
Advanced techniques to assess bone strength, geometry and microarchitecture, such as trabecular bone score, advanced hip analysis, peripheral quantitative CT, high-resolution peripheral quantitative CT and quantitative ultrasound, are currently being investigated. A recent study found that a low trabecular bone score was more common in women with POI than in healthy premenopausal women.15 These emerging techniques may be useful adjunctive tools in the assessment of fracture risk; however, they require further validation, and DXA remains the gold standard imaging tool for investigating osteoporosis.
In case of any bony tenderness or back pain, further evaluation with spinal x-rays to exclude fractures should be performed.
Management
Management of bone health encompasses nonpharmacological measures, pharmacological interventions and treatment of comorbidities that may affect bone health (Flowchart).14,16 However, a formal appraisal of guidelines for bone health showed variable quality and recommendations and a variable consensus on the optimal hormone replacement therapy (HRT) regimen and DXA screening and monitoring.14 Providing information to women is an integral part of management (Box 2); lack of knowledge on bone health is associated with suboptimal health-related behaviours.17
{kind=link}
Nonpharmacological measures
Routine lifestyle measures to maintain adequate nutrition, a healthy body mass index, calcium intake and vitamin D status and high-intensity progressive resistance training should be adopted to optimise bone health. Women should be counselled on smoking cessation and avoiding excess alcohol. Furthermore, coexisting causes of secondary osteoporosis should be diagnosed and appropriately managed as ongoing disease activity contributes to ongoing bone loss or inadequate treatment responses.18
Pharmacological interventions
HRT with oestrogen (with added progestogen in women with an intact uterus) should be initiated at the time of POI diagnosis unless contraindicated (e.g. in women with hormone-sensitive cancers) and continued until the average age of menopause.2 This not only improves skeletal outcomes but also helps alleviate menopausal symptoms, prevents long-term sequelae, such as cardiovascular disease and cognitive impairment, and is required for pubertal induction.19
The use of HRT has been shown to maintain or increase lumbar spine, femoral neck and hip BMD compared with placebo; however, the optimal dose and formulation is still debated.20 A recent observational study showed an increase in spine BMD in women with POI taking continuous combined oral contraceptive pills (COCPs) or high-dose HRT; the BMD response in the low-dose HRT or no therapy groups were inferior to the former two groups in the study.21 These findings were corroborated in a systematic review and suggest that continuous COCP or HRT containing at least 2 mg oral estradiol are required for bone health, whereas low-dose HRT, cyclical COCPs or no treatment are associated with unfavourable bone outcomes.22 Additionally, the cause of POI also impacts BMD response to HRT. Bisphosphonate therapy is more effective than HRT for women with iatrogenic POI following allogeneic stem cell transplantation.23
Nevertheless, when selecting HRT, an individual’s preference should be considered to ensure compliance, as nonadherence to HRT can compromise bone health. Transdermal HRT is preferred in women with risk factors for venous thromboembolism or stroke, as oral HRT preparations have a higher risk of hypercoagulability than transdermal preparations because of hepatic first-pass effects, which cause altered production of hepatic coagulation proteins.24 Continuous COCP may be noninferior to traditional HRT regimens and may be preferred by women with POI, as this provides a more ‘peer similar’ and socially acceptable option.
Spontaneous ovulation and conception can occur in 5% of women with POI;25 therefore, appropriate contraceptive options should be discussed with women not desiring pregnancy. Transdermal oestrogen combined with the levonorgestrel intrauterine device is a useful regimen providing contraception, symptom management and prevention of long-term sequelae of hypoestrogenism. Continuous or long cycles of COCP can be prescribed to prevent periods of symptomatic oestrogen deprivation. Women considering pregnancy should be informed regarding possible bone loss during pregnancy and breastfeeding, and the importance of maintaining healthy nutrition and exercise.
Specialist management is recommended for women with POI who require pubertal induction, in whom HRT is contraindicated or who have a history of thrombophilia. Additionally, the use of HRT is controversial in women with iatrogenic POI in the context of risk-reducing bilateral salpingo-oophorectomy for BRCA1 mutation and in the absence of breast cancer. Limited data suggest that oestrogen-only HRT does not increase the risk of breast cancer.26,27 Women with low bone mass, osteoporosis or evidence of significant declines in bone mass on serial DXA scans should be referred to an osteoporosis specialist for consideration of other osteoporosis-specific pharmacological therapies such as bisphosphonates. Limited literature exists on the clinical use of denosumab, raloxifene and tibolone in this group of women, whereas anabolic agents such as romosozumab and teriparatide have not been trialled in women with POI. Teriparatide has been shown to be efficacious in young premenopausal women with idiopathic osteoporosis, medication-induced amenorrhoea, anorexia nervosa, pregnancy, lactation-associated osteoporosis and glucocorticoid-induced osteoporosis, and may prove useful in women with POI.28-32
The desire for future pregnancy must be considered in women in whom osteoporosis-specific treatment is indicated. Although the chance of spontaneous pregnancy in women with POI is low, many will achieve pregnancy with a donor egg and, thus, the potential impact of bone-specific therapies needs to be recognised. Safety data in humans for bisphosphonates are limited, and nonexistent for teriparatide and denosumab. Bisphosphonates accumulate in the maternal skeleton, cross the placenta, accumulate in the fetal skeleton and cause toxic effects in pregnant rats, hence should be used with caution in women planning pregnancy.33-35 An oral bisphosphonate such as risedronate may be preferable over an intravenous bisphosphonate or alendronate due to its shorter half-life in women with osteoporosis and high fracture risk who are intending pregnancy. However, it is recommended to withdraw bisphosphonate therapy for at least 12 months before pregnancy/conception.24 Specialist review by a physician with expertise in osteoporosis is recommended for these women. Denosumab and teriparatide are not recommended for use in pregnant women, as adverse events have been observed in animal studies.
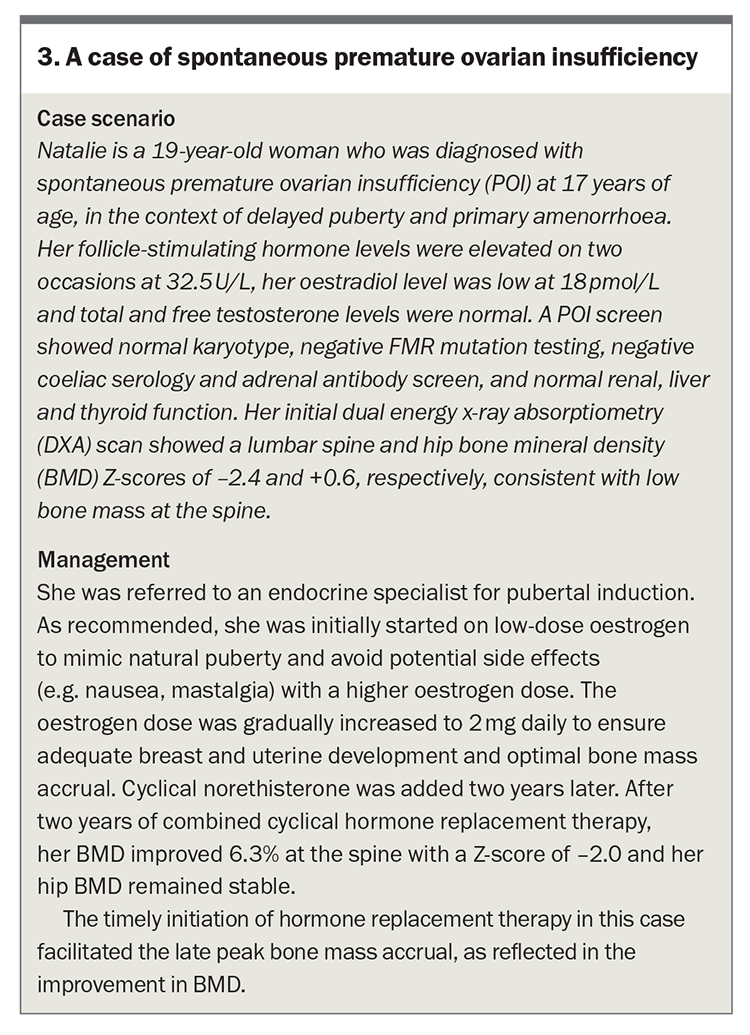
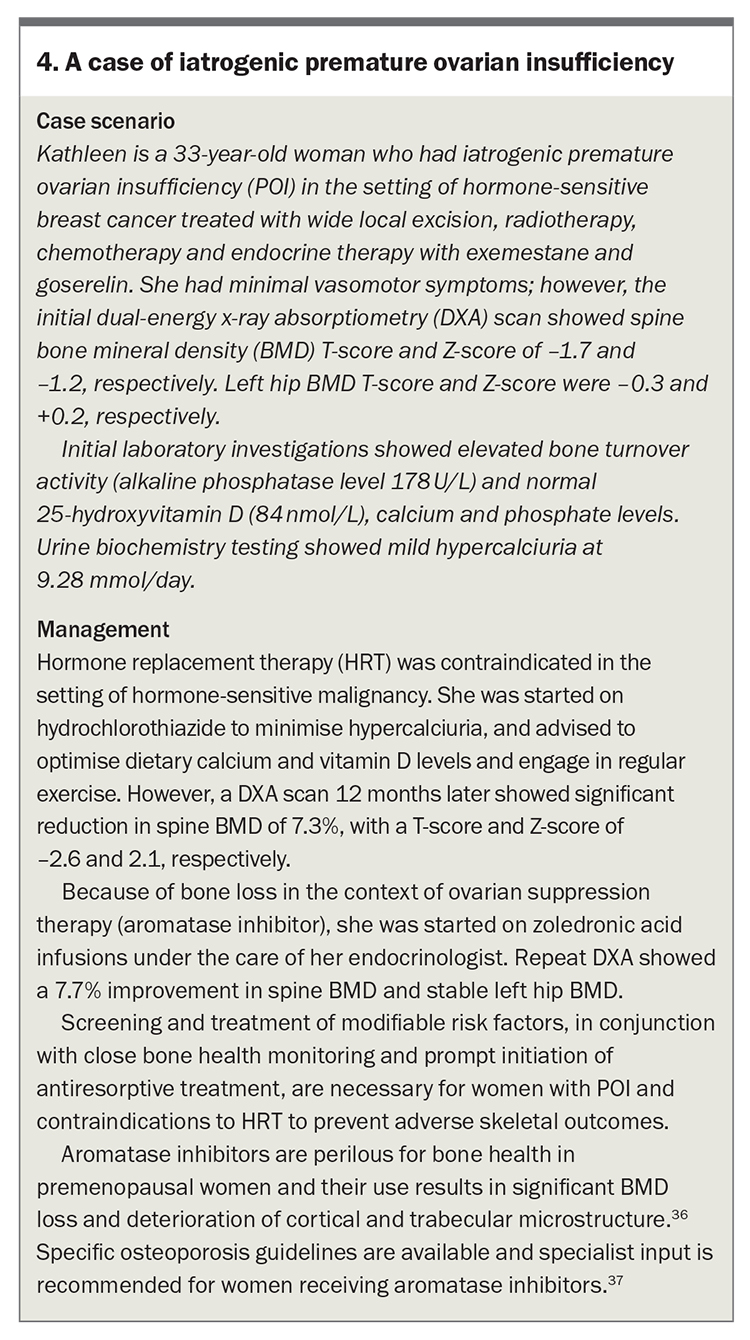
A management algorithm for bone health in women with POI is outlined in the Flowchart. The case studies discuss specific management of bone health in women with POI (Box 3 and Box 4).36,37
{kind=link}
{kind=link}
Conclusion
Poor bone health is common in women with POI, with loss of oestrogen a major risk factor for fragility, fractures, morbidity and mortality. Management to prevent premature and accelerated bone loss involves careful evaluation, optimisation of risk factors, regular surveillance of bone health, timely initiation of HRT (if not contraindicated) or antiresorptive drugs and provision of information. Future studies are needed to evaluate modern diagnostic techniques for assessment of bone health and determine the optimal HRT regimen to preserve bone health. ET
COMPETING INTERESTS: Dr Nguyen, Dr Samad, Associate Professor Milat: None. Associate Professor Vincent has received payment or honararia from Amgen, Besins and Merck.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.