Toxic waist: practical interventions for metabolic syndrome

Obesity
In this opinion piece, GPs are encouraged to recognise metabolic syndrome early as a treatable disease entity in their patients. Practical interventions for metabolic syndrome are described and some tips that GPs can implement themselves even before other multidisciplinary team members have contributed are given.
- Recognise and treat metabolic syndrome with urgency as a disease state in its own right rather than after patients develop diabetes, cardiovascular events, depression, sleep apnoea, osteoarthritis or cancer.
- Encourage patients to focus on reductions in waist circumference rather than merely focusing on weight in kilograms, and to note rewards such as improved wellbeing, reduction in medication burden, reduction in clothing size, and improved fertility and libido.
- Adopt the basic principles of the NHMRC guidelines for diet and exercise prescription and consider prescribing a version of the Mediterranean diet with emphasis on vegetables, whole grains and less refined carbohydrates that may help reduce hyperinsulinaemia and adiposity, as well as beneficially alter the lipid profile.
- Be aware of habitual ‘force-feeding’ patterns (e.g. three meals per day) and consider experimenting with eating only when hungry.
- Akin to ‘five serves of veg per day’, suggest to patients new normal expectations for exercise, for example: ‘Have you done your six doses a day of 20 repetitions of resistance exercise or 10,000 steps each day?’
- Consider prescribing drugs such as metformin, liraglutide and the combination of bupropion and naltrexone in patients whose waist circumference measurement is plateauing despite an appropriate lifestyle intervention.
- Recalibrate the dietary and exercise prescription and motivation levels at each patient visit.
A growing majority of people in Australia are overweight and face a future of chronic disease and crippled healthcare budgets.1 The Australian health culture is mirroring that in the US, and the level of medical urgency to address metabolic syndrome may be inadequate to fight instinctive human sedentarism. Dietary advice pales next to sophisticated marketing of processed food that capitalises on hard-wired urges for carbohydrate, fat and salt. Thus, we might rethink our approach and learn from the same marketing industry to ‘nudge’ (manipulate choice and create a new-normal expectation) and incentivise patients in a leaner, less inflammatory direction.2
Management of metabolic syndrome and its comorbidities ideally involves a multidisciplinary team approach to risk-factor management including motivational interviewing, diet and exercise prescriptions, pharmacotherapy and bariatric surgery. However, the scope of this article is not a comprehensive review of the evidence for each of these specialised disciplines. The NHMRC Clinical practice guidelines for the Management of Overweight and Obesity in Adults, Adolescents and Children in Australia and The Australian obesity management algorithm (developed by the Australian Diabetes Society, the Australian and New Zealand Obesity Society and the Obesity Surgery Society of Australia and New Zealand) both provide evidence-based guidelines for treatment of patients with a body mass index (BMI) of 30 to 40 kg/m2.3,4
The aim of this article is to encourage GPs to recognise metabolic syndrome early as a treatable disease entity in their patients (especially Australian Indigenous and Asian patients in whom morbidity is associated with BMIs <30 kg/m2) and offer tips that GPs might implement themselves even before other multidisciplinary team members have contributed.
What is metabolic syndrome?
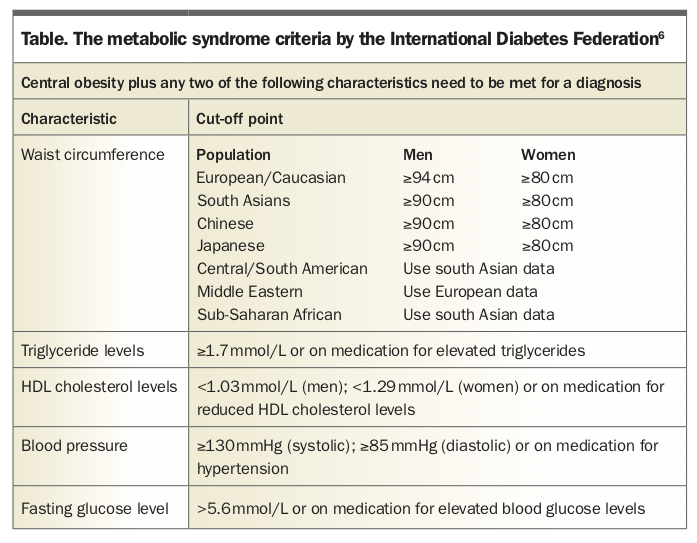
Although obesity per se (BMI >30 kg/m2) is known to increase all-cause mortality rates by more than 50%, the term metabolic syndrome refers to the clustering of central adiposity, atherogenic dyslipidaemia, insulin resistance, dysglycaemia and hypertension. Each of these increases an individual’s risk of developing coronary artery disease, diabetes, fatty liver disease and cancer.5 The International Diabetes Federation consensus definition of the metabolic syndrome is the most practical in the clinic as it is based on easily measurable parameters without the requirement to quantify insulin resistance per se (Table).6
{kind=link}
Pathophysiology: an inflammatory vicious cycle
Genetic causes of metabolic syndrome synergise with an obesogenic environment: increasingly sedentary or screen-centric lifestyles and overconsumption of addictive, energy-dense and processed foods.7 Insulin resistance appears to be a central cause of metabolic syndrome and probably also an effect of it as inflammatory adipocytokines (factors released by adipose tissue) may exacerbate the defective signalling down stream of the insulin receptor.8 This may in turn lead to a further compensatory hyperinsulinaemia, leading to a vicious cycle of adiposity, dyslipidaemia, endothelial dysfunction, a hypercoaguable state and systemic inflammation.
Myocytokines, released by skeletal muscle, might be possible ‘antidotes’ to the aforementioned inflammatory adipocytokines and possible mediators of the benefits of resistance training in people with insulin resistance and metabolic syndrome and survivors of cancer.9 A relative deficiency of these skeletal muscle factors due to a lack of physical work may explain some of the disease states proliferating with sedentary lifestyles.
Barriers to treating metabolic syndrome
Central adiposity is now so normal in society that it may often be ignored in clinics. Even if noted by the doctor, a natural reticence to cause offence or ‘fat shame’, especially in children or vulnerable adults, may prevent a discussion about losing weight. In a limited consultation time, the focus might have to be on only one component of the metabolic syndrome such as hypertension, dysglycaemia or other common complications of obesity such as arthritis or dyspnoea. The adiposity might only be addressed in passing with well meaning platitudes (‘you should really lose some weight’) or be outsourced to a dietitian. Treating the individual risk factors of the metabolic syndrome is crucial to the prevention of cardiovascular disease but failure to address the central cause (central adiposity) may result in sequential polypharmacy adding one risk factor medication or anti-inflammatory after another.
Weight-loss interventions can cause frustration because successful weight loss leads to hormonal changes (the appetite hormone ghrelin rises and the satiety hormone leptin decreases) that drive weight regain to an original set point. Autonomic nervous system changes decrease the resting metabolic rate, the major contributor to energy utilisation.
Inevitable psychosocial pressures can erode motivation, adherence to diet and exercise, and clinical follow up. Doctors might be prone to a sense of futility given that weight loss is followed ultimately by weight regain in many patients.
Doctors, voters and policymakers may also view obesity or metabolic syndrome as being self-inflicted due to laziness or lack of willpower. Thus effective pharmacological and surgical strategies for obesity may be ignored if perceived by patients or clinicians as expensive indulgences, a last resort or an easy way out.
Role of the GP in management
Although a multidisciplinary team approach is ideal for managing patients with metabolic syndrome, primary care is the most important setting for capturing and treating more patients with metabolic syndrome (Box). A pragmatic first step is to encourage all doctors to recognise and document metabolic syndrome in the process of addressing other presentations. Time could then be scheduled to address metabolic syndrome and prepare the care plan.
{kind=link}
Practically, this might involve including waist circumference measurement as part of the routine examination of all new patients and applying a checklist for the clinical features of metabolic syndrome in those with central adiposity (Table). People fulfilling the criteria for metabolic syndrome could be educated about insulin resistance, central adiposity, their relationship to food and exercise, and the attendant cardiovascular risks and receive immediate interventions from the GP.
On diagnosing metabolic syndrome, I recommend that a chronic disease care plan be prepared by the patient’s GP with negotiated goals and outcome measures. This would allow subsidised allied health care with input from exercise physiologists, dietitians and psychologists to assist the GP and patient in a co-ordinated approach to reducing waist circumference and each of the risk factors of metabolic syndrome.
All doctors, especially those in training, can learn tactful ways of addressing central adiposity. The term obesity is accepted as the standard term used for staging and researching the condition internationally, and many clinicians remain adamant about ‘calling a spade a spade’. However, I find that labelling patients as ‘morbidly obese’ in referral letters (often read by patients) is not particularly motivating and can be deeply hurtful especially for stigmatised patients battling low self-esteem. Thus an alternative approach is to document the current waist circumference measurement in a nonjudgemental tone, as a manageable metric that becomes a goal for improvement over a set time period (e.g. a reduction of 5 cm over 10 to 12 weeks).
Patients can be instructed to measure their own waist circumference in the same manner (e.g. at the level of their navel) and to document it periodically as a motivational tool. Waist or clothing size reduction might provide a subconscious ‘nudge’ for some patients that might influence the intervening week’s eating and moving. In measuring and addressing adiposity, particular care is needed with some patients’ (particularly adolescents) fragile self-image, especially if the history revealed prior bullying or eating disorders.
The focus in any given consultation may be on one morbidity, for example, dysglycaemia in a person with metabolic syndrome and type 2 diabetes or oligomenorrhoea in a woman with polycystic ovary syndrome (PCOS). However, it is important to address all the risk factors and potential morbidities of metabolic syndrome. In both of these multirisk scenarios, it would be easy to overlook the patient’s lipid management, nonalcoholic fatty liver disease, daytime fatigue due to obstructive sleep apnoea or the importance of appropriate cancer screening while addressing their central adiposity.
Clinical steps
Recognise
Recognise metabolic syndrome in a patient with central adiposity who presents for other reasons or accompanies their family member with metabolic syndrome.
Clinical history
- Is there a history or family history of diabetes, cancer or cardiovascular disease?
- Consider lifestyle roadblocks (e.g. seated and driving hours, care of dependents).
- Consider calculating the risk of developing type 2 diabetes using the Australian Type 2 Diabetes Risk
- Assessment Tool (AUSDRISK) and if high risk (score >12) investigate for type 2 diabetes.10
- Ask about motivating opportunities or major milestones (e.g. weddings, awaiting grandchildren, attempts to conceive).
- Assess dietary carbohydrates, liquid calories, alcohol, vegetable, protein, fibre and fat intake over the past 48 hours.
- Quantify activity and exercise hours over the past week.
- Enquire about depression, anxiety and eating disorders.
- Enquire about smoking status.
- Enquire about snoring and daytime fatigue as symptoms of obstructive sleep apnoea.
- Is the patient taking any drugs that promote adiposity or insulin resistance (e.g. some psychotropic medications, corticosteroids)?
- Ask about previous elite-level sports (I often see metabolic syndrome after retirement in insulin-resistant athletes).
Physical examination
- Perform a cardiovascular examination.
- Measure waist circumference and/or BMI.
- Assess thyroid status.
- Look for signs of insulin resistance: acanthosis nigricans or dark skin tags on neck or axillae.
- Is hirsutism or acne present, as manifestations of PCOS?
- Exclude Cushing’s stigmata.
Initial investigations
- Measure lipid levels, blood glucose levels, and electrolytes, urea and creatinine levels. Perform liver function tests.
- In patients with indicative history perform thyroid function tests, oral glucose tolerance test, stress ECG,
- sleep study and liver ultrasound. Measure HbA1c and cortisol levels.
Interventions
Goal setting and motivation
The principle of the SMART goal setting may be helpful in clinical practice.11 This refers to goals that are specific (e.g. waist reduction), measurable (cm), agreed on, relevant (e.g. HbA1c of 6% in a 95-year-old patient), and time based (e.g. reduction of 5 cm over 10 to 12 weeks).
Motivational interviewing involves developing an understanding of patients’ goals, fears and limitations and expressing empathy for their frustrations. For example, the goal of weight loss measured in kilograms can be problematic. Some patients are so traumatised by this perceived goal that standing on the scales is an ordeal. Weight loss in kilograms is often confounded by lean muscle gain through resistance exercise, thus the kilogram metric may be counter motivational. Clinicians might therefore consider encouraging a reduction in waist circumference and improvement of metabolic risks, as well as aiming for a 5 to 10% weight loss in kilograms. An example of a realistic goal agreed on between the clinician and patient might be 5 cm waist circumference reduction over 10 to 12 weeks or 5 to 10% weight loss over 12 months.
Opportunities to ‘nudge’ (motivate change to desired health behaviours) should be seized. Such teachable moments include close shaves with existential threats such as cancer or heart attack wherein patients may have increased perception of their risk. Positive nudge opportunities include goals related to upcoming life events (e.g. wedding or planning conception).
Scheduled follow-up visits and recalibration of goals and interventions are crucial. Emphasising the rewards of weight loss when they occur is important. Rewards such as improved energy, clarity, sleep and libido and reductions in clothing size and medication burden can be powerful motivators to persist with behavioural changes. At these follow-up visits, roadblocks to lifestyle change, such as depression, fatigue due to sleep apnoea or care responsibilities for family members, need navigating.
Food prescription
The NHMRC Australian Guide to Healthy Eating (www.eatforhealth.gov.au/guidelines/australian-guide-healthy-eating) provides a comprehensive evidence base for dietary prescription.
Before and after referral to a dietitian, it may be impactful for patients to receive dietary prescription from their doctor. The food strategy might begin with auditing the past 24 hours’ intake of macronutrients, for example:
- carbohydrates
— simple (e.g. added sugar, confectionary, soft drinks, cakes)
— complex (e.g. whole grain cereals, vegetables, fruits) - fibre (e.g. beans, legumes, whole grains)
- protein
- saturated fats.
Dietary dogma is pervasive and can be counterproductive to fat loss in people with metabolic syndrome. For example, ‘breakfast is the most important meal of the day’, which leaves many insulin-resistant patients with metabolic syndrome guilt ridden about skipping this meal. There is emerging doubt that skipping a meal leads to excess caloric intake at subsequent meals and indeed being given the liberty to skip breakfast may indeed be a weight-loss strategy for patients with metabolic syndrome who are not hungry at that time.12 Similarly, being advised to eat six small meals per day may be less effective than eating as often as needed – for example, two meals a day, a late breakfast and early dinner.13
Several dietary approaches have gained popularity recently including the paleo diet, ketogenic diet and 5:2 fasting, which afford weight loss for some but carry risk for certain groups such as pregnant women and children. The strongest evidence for a specific dietary prescription in people with metabolic syndrome is for the Mediterranean diet, as shown in the PREDIMED study, which reported a significant rate of reversion of metabolic syndrome.14 This diet emphasises fresh vegetables, olive oil, omega 3-rich nuts, fish and whole grains. Very low carbohydrate diets have emerging evidence for improving lipid profiles and blood glucose levels and reducing diabetes medication requirements in patients with type 2 diabetes.15 This has lead to new dietary recommendations from the American Diabetes Association.16
I prescribe a version of the Mediterranean diet emphasising fibre and vegetables of many colours (‘eat the rainbow’) as the staple along with occasional whole grains, quinoa, brown rice and buckwheat. There is evidence for increasing the volume of low-energy density foods (e.g. vegetables) as a strategy to promote satiety and thus maintenance of reduced energy diets.17 A practical example for patients might be to explain that 250 g of carrots contain approximately the same calories as 20 g of chocolate but the volume of the former would be far more filling.
Reducing the volume of wheat bread, rice, pasta and breakfast cereals might accompany high-quality proteins from fish, poultry and smaller quantities of red meat. In all patients, a daily dose of omega-3 rich nuts has strong evidence from the PREDIMED study for decreasing cardiovascular risk.14
A dietitian, might then fine tune the doctor’s preliminary prescription based on the patient’s results over the next few weeks. This recalibration of the diet is crucial, as patients may fail to increase their fibre and vegetable intake adequately when attempting to cut their cereal carbohydrates or energy-dense foods, resulting in constipation and fatigue.
Exercise prescription
Exercise improves the central pathophysiology of metabolic syndrome, that is, insulin resistance and central adiposity, as well as improving blood pressure and wellbeing. Exercise has also been shown to have beneficial effects in preventing the onset of type 2 diabetes.18-22
It is recommended that patients with type 2 diabetes or prediabetes accumulate a minimum of 210 minutes per week of moderate-intensity exercise (e.g. achieved by 30 to 60 minutes per day of brisk walking on most days of the week) or 125 minutes per week of vigorous-intensity exercise with no more than two consecutive days without training.23 This will also confer benefits in the prevention of cardiovascular disease, but the more intense exercise prescription should be made after assessing any underlying coronary risk.
Given that skeletal muscle is the largest site by mass of insulin and carbohydrate metabolism, I believe a specific daily ‘dose’ of anaerobic (resistance) training could be prescribed by the GP as it improves insulin resistance.
Referral of the patient to an exercise physiologist as part of the GP care plan allows uptitration of the doctor’s exercise prescription and safe tailoring around comorbidities to avoid injury.
For all patients, I initiate an exercise prescription before they see an exercise physiologist, by ‘nudging’ them as follows.
- A daily aerobic dose expectation of 10,000 steps (recorded on a wrist pedometer or smart phone), 45 minutes walking or a fitness class.
- In younger patients, a beep test score (a commonly used fitness indicator involving shuttle running between cones 20 meters apart) or a 2 km time trial with their partners for patients who are able to run. For older patients, they could be asked to take a minute off their lap time on each long walk.
- An anaerobic dose of six sets of 20 repetitions of light upper body resistance exercise such as bicep curls with 1 to 3 kg dumbbells, lower body squats or sit-stands from a chair in older patients. This unsophisticated but do-able prescription can be nudged by linkage to automatic acts, such as eating meals or ensuring the first ‘dose’ is done before leaving the bedroom in the morning, the second as squats while brushing their teeth.
- Nonexercise activity can be encouraged by parking further from the station, leaving the office for a walking
- lunch rather than eating at their desk, and decreasing sitting time by using stand-up desks or smart watches that signal it is time to get up and walk.
Pharmacotherapy
Drug therapy to assist weight loss is an option for patients whose waist circumference is plateauing despite an adequate dietary and exercise strategy. The Australian obesity management algorithm provides an excellent resource on lifestyle changes, reduced energy diets, very low energy diets, pharmacotherapy and surgery.3
Several agents may be efficacious for weight loss in people with metabolic syndrome and prediabetes, including liraglutide, orlistat, phentermine, and a combination of naltrexone and bupropion, which are all TGA-approved for weight loss. Metformin and topiramate can also be used for weight loss, but are used off label for this indication. All drugs should be used only within a medically supervised program of diet and exercise change and none as yet attract a PBS subsidy for a metabolic syndrome indication.
The glucagon-like peptide 1 (GLP-1) agonist liraglutide administered as subcutaneous injections in doses of up to 3.0 mg daily can deliver substantial weight loss and potential cardiovascular benefits but the unsubsidised cost can be prohibitive for many patients.24
Orlistat impairs fat absorption and its use can be limited by adverse effects on stool quality and fat soluble vitamin absorption.
Phentermine is an effective, centrally-acting appetite suppressant that can have sympathomimetic side effects and is contraindicated in patients with significant cardiovascular disease.
The combination of naltrexone and bupropion has been recently approved by the TGA.25 Naltrexone, an opioid receptor antagonist, inhibits the rewards centres in the brain and bupropion, an antidepressant, has an appetite suppressant effect similar to that of amphetamines. The combination is effective for weight loss in combination with lifestyle change but is contraindicated in patients with renal failure, cardiovascular disease or seizure activity.
Metformin in addition to lifestyle change has been proven to be more efficacious for fat loss than lifestyle change alone in patients with antipsychotic-induced weight gain, as well as restoring menstrual regularity in women with PCOS.26-28 In the absence of randomised controlled trial data, there are suggestions from observational clinical and in vitro studies that metformin might also have a role in optimising the gut biome, and possibly a protective role against some cancers.29,30 In my opinion, metformin provides a relatively cheap and safe initial adjuvant to behavioural change to aid fat loss in patients with metabolic syndrome or prediabetes.
In patients with metabolic syndrome and suboptimally controlled type 2 diabetes, there are PBS reimbursed options for addressing hyperglycaemia that facilitate weight loss. These include the oral sodium-glucose cotransporter-2 (SGLT-2) inhibitors, such as empagliflozin and dapagliflozin, which can be added to metformin, sulfonylurea or insulin therapy in patients with an adequate glomerular filtration rate. The loss of glucose in the urine with these agents can result in weight loss of several kilograms in the first year of therapy.31 The popularity of this class of drug has been enhanced by a significant reduction in death from cardiovascular causes in patients with type 2 diabetes at high risk for cardiovascular events, as shown in the Empagliflozin Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG) study.31 Risks with use of the SGLT-2 inhibitors include ketoacidosis as a rare complication especially in the setting of general anaesthesia. Similarly, weekly injections of the GLP-1 agonists exenatide or dulaglutide can be added to metformin therapy and may assist with weight loss as well as improved glycaemic control.32
The addition of medications to assist with weight loss should be balanced with attempts to decrease drug burden (e.g. insulin doses in people with type 2 diabetes and antihypertensive drug requirements) when weight loss eventuates.
Bariatric surgery
Bariatric surgery may be the most effective fat loss intervention for patients with a BMI greater than 35 kg/m2 or greater than 30 kg/m2 with comorbidities, with up to 33% weight loss achieved. Bariatric surgery has also been shown to reduce death due to myocardial infarction by 48% and cancer mortality by 38%.33
Depending on the type of surgery (sleeve gastrectomy or gastroduodenal bypass) weight loss results from a combination of restriction of the stomach’s capacity but also through neuroendocrine effects on energy balance such as a decrease in the appetite hormone ghrelin, an increase in small intestinal secretion of GLP-1 and possibly a change in the intestinal biome. The Australian obesity management algorithm provides a comprehensive pathway for consideration of surgery in patients with a BMI above 30 kg/m2 who have failed at weight loss with behavioural and pharmacological strategies and in those with uncontrolled type 2 diabetes.3
Role of shared care between a specialist and the GP
Management of metabolic syndrome should be co-ordinated through the patient’s GP and may include input from endocrinologists, bariatric surgeons, dieticians, exercise physiologists and clinical psychologists.
Structured recall for GP follow up is crucial in a process that is rife with lapses in motivation. The rewards of successful fat loss and muscle gain in metabolic syndrome, for both the doctor and patient, include a reduction in the number of prescription medicines and a significant increase in quality of life.
Prevention strategies
Opportunities to prevent metabolic syndrome should be seized by encouraging at-risk people to adopt similar dietary and exercise changes to those recommended for people with existing metabolic syndrome. People at risk include those with overweight family members and insulin-resistant individuals (e.g. women with previous gestational diabetes or PCOS, former elite athletes and those in sedentary jobs).
Summary
The multiple risk factors and morbidities associated with metabolic syndrome need to be addressed individually to prevent cardiovascular disease, type 2 diabetes, sleep apnoea, depression, cancer and arthritis. However, addressing the syndrome early as a whole by recognising central adiposity and the clusters of the metabolic syndrome provides an opportunity to prevent such patients manifesting these diseases and becoming victims of sequential polypharmacy.
GPs and other doctors should consider documenting metabolic syndrome early in high-risk patients and preparing a chronic disease care plan, focusing on a reduction in waist circumference (fat loss) rather than a decrease in kilograms (affected by lean muscle mass gain). Goal setting, motivational interviewing and an initial food and exercise prescription can be easily implemented by GPs, before refinement (if feasible) by dietitians and exercise physiologists. Effective pharmacotherapy for weight loss is available but only as an adjunct to GP-monitored behavioural change. Specialist input from endocrinologists and bariatric surgeons may be worth considering in patients plateauing with these initial measures. ET
References
376: 595-605.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.