Menopausal hormone therapy: current recommendations

Menopause
Women's health
Menopausal hormone therapy (MHT) has proven benefit in reducing vasomotor and vulvovaginal symptoms and fracture rates in menopausal women. However, since the publication of the Women’s Health Initiative study findings in 2002 and 2004, use of MHT has declined. This article aims to alleviate concerns around the use of MHT by providing an evidence-based review of the available literature comparing the benefits and risks of MHT use in its different formulations.
- Menopause can be characterised by vasomotor and vulvovaginal symptoms as well as sleep difficulties and mood disorders.
- Menopausal hormone therapy (MHT) is the most effective treatment for vasomotor symptoms and also alleviates vulvovaginal symptoms.
- Controversies around MHT have resulted in reduced use of this therapy.
- MHT is recommended for women less than 60 years of age within 10 years of menopause.
- Local estrogen therapy is recommended for women with vulvovaginal symptoms in the absence of vasomotor symptoms.
- MHT is currently not recommended for use in the prevention of cardiovascular disease or dementia.
Menopause, marked by the permanent cessation of menses, is an important change in a woman’s physiology. Although the average age of menopause in the western world is 51 years, multiple factors can affect the age at which menopause is reached. Japanese and Malaysian women are known to reach menopause later in life, therefore ethnicity is important to consider. A history of smoking, exposure to alkylating agents and nulliparity are all associated with earlier menopause.
Although every woman’s experience of menopause is different, identification of symptoms provides an opportunity to improve quality of life. The challenge for GPs often lies in differentiating menopausal symptoms from those due to other pathology.
Symptoms of menopause
The few years before menopause can be a period of transition and it is not uncommon for women to exhibit vasomotor symptoms with only a few months of amenorrhoea. The typical symptoms of menopause (hot flushes, night sweats and vulvovaginal symptoms of dryness and dyspareunia) are due to the decline in ovarian oestrogen production. Surgical menopause is likely to cause more severe symptoms. Low mood and poor sleep are also common.1 Once menopause has been identified as the cause of a patient’s symptoms, both lifestyle and pharmacological options are available to varying benefit (particularly lifestyle options).
Australian studies have shown that up to 75% of perimenopausal women can be symptomatic with vasomotor symptoms.2 The challenges of treating menopausal symptoms are highlighted by findings that up to one-third of postmenopausal women between 60 and 65 years of age continue to experience untreated moderate-to-severe vasomotor and vulvovaginal symptoms.3 These studies also suggest that local menopausal hormone therapy (MHT) is under used in the older age group of postmenopausal women (despite severe vulvovaginal symptoms) highlighting an opportunity for intervention.
Physiology of menopause
Menopause is defined as the time period that follows 12 months after a woman’s final menstrual period. This may occur spontaneously or because of surgery or a disease process. Cessation of menses before 40 years of age is classified as premature ovarian insufficiency. Biochemical investigations demonstrate increased follicle stimulating hormone concentrations, although routine measurement is not recommended and should only be performed in unusual circumstances such as in suspected premature ovarian insufficiency.
Reductions in available ovarian follicle cohorts result in reduced inhibin B secretion. Consequent diminution of inhibin B mediated negative feedback on the anterior pituitary results in increased follicle stimulating hormone secretion.4 Availability of testosterone also changes with age. At 20 years of age, 100 to 400 mcg of testosterone is synthesised through ovarian and adrenal androgen secretion; by 40 years of age these levels halve. No direct correlation with menopause has been identified and ovarian androgen production may continue after the last menstrual period.5 However, women who undergo surgical menopause are likely to be symptomatic of testosterone deficiency, particularly lower libido, due to the sudden change in testosterone concentrations. Furthermore, use of estrogen therapy can increase serum hormone binding globulin levels, which reduces free testosterone levels. This phenomenon may result in some women on estrogen replacement therapy experiencing symptoms of testosterone deficiency.6 Oestradiol production by granulosa cells also ceases over time.7
Controversies and considerations about MHT
MHT is the most effective method of alleviating vasomotor symptoms of menopause and can also provide relief from vulvovaginal symptoms. However, its use significantly reduced following publication of the findings of the Women’s Health Initiative (WHI) study in 2002 and 2004.8,9
The WHI was designed to investigate the benefits of MHT in primary prevention of cardiovascular disease. It evaluated the effects of combined estrogen and progestogen in 16,608 postmenopausal women with an intact uterus, and that of estrogen alone on 10,739 postmenopausal women with prior hysterectomy. The primary aim of the trial was to determine the effect of MHT on coronary heart disease and breast cancer, while secondary assessments included effect on bone health and colorectal and endometrial cancers. Women were randomised to receive either conjugated equine estrogen (0.625 mg daily), with or without medroxyprogesterone acetate (2.5 mg daily), or placebo.
The combined estrogen and progestogen arm was stopped in 2002 due to concerns about increased incidence of breast cancer in the women randomised to receive MHT.8 Interim analyses suggested an increased risk of cardiovascular events, although statistical significance was not reached. A higher risk of venous thromboembolic disease was identified in women treated with combined MHT, although deep venous thromboses (DVTs) were the major burden of disease, not pulmonary embolism. In 2004, the estrogen-only arm of the study was stopped due to increased risk of stroke in those randomised to active treatment. It attributed 12 events of strokes per 10,000 person years to MHT.9 Increased risk of DVT was again identified.
However, subsequent review of the participants’ baseline characteristics suggested they had an increased cardiovascular risk profile. The women were older with a mean age of 63 years and only 33% were less than 60 years of age. Only 30% had a normal (less than 25 mg/kg2) body mass index while 34% were in the ‘obese’ category and 50% had a history of smoking.10 About 25% of women in the combined MHT group and almost 50% in the estrogen-only arm had been treated with MHT in the past.8,9 The WHI also did not assess the effect of alternative formulations of estradiol or progestogen therapy on the above outcomes.
Current clinical practice uses different formulations of estrogen (including transdermal options), which are now more commonly used than conjugated equine estrogen. Although the WHI examined effects of MHT on women across a range of age groups postmenopause, this is not representative of usual practice as MHT is most often prescribed within 10 years of menopause for symptom management.
Subsequent analysis of WHI data demonstrated a protective effect of MHT on cardiovascular disease in women less than 60 years of age when prescribed within 10years of menopause whereas a higher relative risk was identified in older women.11 Other studies in women treated with MHT in the first 10 years of menopause for vasomotor symptoms have not shown an increased risk of cardiovascular disease or mortality.12 Furthermore, long-term studies of oral and transdermal estrogen replacement have shown beneficial effects of MHT on women’s lipid profiles with reductions in total cholesterol, triglyceride and low-density lipoprotein levels.13
Subsequent studies have suggested an increased risk of stroke with increasing age for the duration of MHT alone. The 2016 ELITE (Early versus Late Intervention Trial with Estradiol) study also demonstrated that commencement of MHT within six years of menopause in women less than 60 years of age was not associated with progression of carotid artery intima-media thickness whereas MHT commencement at 10 years postmenopause was.14 Although current guidelines recommend against the use of MHT in women with established cerebrovascular disease, a case-control study in 2010 demonstrated that the use of low-dose (50 mcg estrogen or less) transdermal patches was not associated with an increased risk of stroke whereas oral preparations were, with a dose-dependent effect.15
Although the increased risk of venous thromboembolism (VTE) was reproduced in other studies such as HERS (Heart and Estrogen/progestin Replacement Study) and the oral MHT arm of the French E3N (Etude Epidémiologique de femmes de la Mutuelle Générale de l’Education Nationale) study, this risk has not been associated with transdermal estrogen preparations in the E3N study as well as other systematic reviews and meta-analyses.16,17-20 With regard to progestogen formulation and DVT risk, a higher risk was observed in women taking medroxyprogesterone acetate compared with women taking norethisterone when compared with placebo in the Million Women Study.21 Other studies have consistently shown that micronised progesterone is not associated with increased VTE risk.17,20-22 Hence, in women at risk of VTE, transdermal estrogen preparations and micronised progesterone are recommended in favour of oral estradiol preparations.23
MHT and breast cancer
In women without a history of breast cancer, the WHI identified eight incidents of invasive breast cancer per 10,000 women over five years in those treated with combined MHT.8 The Million Women Study also reported an increased risk of breast cancer in women with prior exposure to MHT compared with those who had no exposure.24 The risk seems to be higher in women who commence MHT within five years of menopause.24 This risk seems to return to baseline five years after cessation of therapy. The risk profile also changes with the type of estrogen used and is much higher in women on progestogen in conjunction with estrogen.25 Progestogen use over progesterone is also associated with a higher risk of breast cancer.26
MHT, including tibolone, is currently not recommended in women with breast cancer and nonhormonal therapy is recommended in those who are resistant to lifestyle modifications. In women with severe vasomotor symptoms resistant to nonhormonal therapy, specialist review is recommended.27
MHT and bone health
A reduction in bone mineral density (BMD) of about 10% can be expected with menopause, leading to increased fracture risk. Meta-analyses have demonstrated that use of both opposed and unopposed estrogen therapy is associated with significantly increased BMD at all sites in postmenopausal women.28 This is recommended to be used in conjunction with weightbearing exercise, adequate dietary calcium intake and vitamin D supplementation. The Danish Osteoporosis Study demonstrated reduced forearm fractures whereas the WHI demonstrated reduced hip fracture rates equivalent to five fewer hip fractures per 10,000 person years.8,9,29 One year of treatment with MHT has demonstrated benefits on lumbar spine BMD with an increase by 5.4% and at nonvertebral sites by 2.5 to 3%.30 Although MHT is not routinely recommended for fracture prevention for women more than 60 years of age or more than 10 years from onset of menopause, it is beneficial for younger women.31
MHT and cognition
Despite expectations, research to date has not demonstrated reproducible evidence for improved cognition with MHT use. The heterogeneity in the pathophysiology and aetiology of cognitive decline as well as scarcity of robust trials are likely to contribute. A recently published trial that assessed the effects of MHT on 17 individuals suggested attenuation in progression of cognitive decline in participants randomised to transdermal estradiol and micronised progesterone compared with those randomised to placebo.32
MHT and side effects
In some women, progestogens can lead to symptoms of bloating, breast tenderness, irritability and depression. An alternative regimen or a different route of administration may be trialled. Nausea, cramps, headache, fluid retention and breast tenderness have been reported with the estrogen component.
Progestogens in MHT
The choice of progestogen can be important, especially in women with metabolic syndrome. Use of medroxyprogesterone acetate has been shown to negate the positive effects of estrogen whereas micronised progesterone does not.33 Although micronised progesterone has also been associated with improvements in sleep and mood in menopausal women, only small studies have been conducted and results are yet to be confirmed through more rigorous evaluation.34 Observational studies have also shown that breast cancer risk may be less in women using progesterone compared with those using synthetic progestogens.35
Available hormone preparations
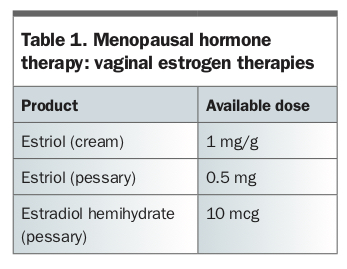
Local estrogen preparations are recommended in women who are concerned only by vulvovaginal symptoms of menopause and adjunct therapy with progestogens is not required. Appropriate advice for application of local estrogen therapy is important to reap the benefits. Current available therapy involves nightly use for two weeks then twice weekly. Table 1 lists current available preparations of vaginal estrogen therapies.
{kind=link}
Transdermal estrogen preparations are recommended for women with increased risk of venous thromboembolic disease.
Oral preparations are available as estrogen-only therapy for women who have had a hysterectomy or combined with progestogens for women with an intact uterus to prevent endometrial hyperplasia. Table 2 describes current available preparations.36-38 For the purpose of vasomotor symptom treatment, 0.625 mg of conjugated equine estradiol has similar efficacy to 1 mg 17-beta estradiol and 50 mcg daily of transdermal 17-beta estradiol.36
{kind=link}
Bazedoxifene (a selective estrogen receptor modulator) is also approved for the use of vasomotor and vulvovaginal symptoms in menopause, in conjunction with conjugated equine estrogens. It has known beneficial effects on BMD and bone turnover markers.39 It is currently not recommended for use in women with renal impairment and is contraindicated in women with hepatic impairment, VTE or history of breast cancer. Muscle spasms, dizziness and gastrointestinal symptoms appear to be the most common adverse effects.40
Tibolone is a synthetic drug that has estrogenic, progestogenic and androgenic effects, and is efficacious in addressing the vasomotor symptoms and vulvovaginal symptoms of menopause.41 Due to its progestogenic effects, concurrent use of progestogens is not required. Tibolone is known to reduce triglyceride levels; however, it also reduces high-density lipoprotein levels. It has protective effects on bone health with reduced risk of vertebral and nonvertebral fractures demonstrated in a randomised study of women between 60 and 85 years of age.42 In this population it also increased risk of stroke while breast cancer risk was decreased.42 However, tibolone is currently not recommended in women with breast cancer due to conflicting evidence.43 Possible side effects of tibolone include vaginal bleeding or discharge, and breast discomfort. Some women may also experience fluid retention, gastrointestinal upset and liver dysfunction.42
Transdermal testosterone preparations have demonstrated benefit in treating hypoactive sexual desire disorder (described as a recurrent or persistent lack of desire for sexual activity not attributable to another psychiatric disorder), substance use or general medical condition.44 Testosterone use in menopausal women is currently not TGA approved for use in Australia. Postmenopausal women on MHT with persistent symptoms of sexual dysfunction may be referred for specialist review for consideration of testosterone therapy if other causes have been excluded or treated. Preparations at 50 mg per week and twice-weekly patches of 300 mcg daily have both been trialled in participants already on estrogen therapy with symptomatic benefit.44-46 These women had improvements in the frequency of sexual activity and desire and also experienced less personal distress. Testosterone therapy appears to be well tolerated with safety data currently available up to 24 months.47 In women who have been prescribed testosterone therapy, measurement of testosterone levels before commencement and at three and six weeks is recommended to ensure dosing is appropriate.48 It is recommended that women on testosterone therapy are reviewed at least every six months for over-androgenisation and, if they do not respond within six months of starting therapy, that treatment is ceased. Transdermal testosterone therapy is contraindicated in women with cardiovascular or liver disease, breast cancer or uterine cancer.
Choice of preparation will depend on whether the woman has had less or more than 12 months of amenorrhoea before evaluation; has an intact uterus; and has vasomotor symptoms, vulvovaginal symptoms or both. The thromboembolic and breast cancer risk profile will also guide therapy. The profile of nonendometrial effects of progestogens may also contribute to the choice of progestogen. Patients require re-assessment at three months for evaluation of response to therapy and development of side effects, and subsequently at least every 12 months. Dose escalation can occur if there is minimal response to therapy. In the event that a patient does not respond to therapy despite dose escalation, referral for specialist review and cessation of medication is recommended.
Ongoing evaluation and minimisation of cardiovascular risk through management of weight and dyslipidaemia are important in minimising complications. Evaluation of adverse symptoms such as vaginal bleeding requires assessment for pelvic pathology.
Conclusion
In women less than 60 years of age and within 10 years of menopause, the benefit of MHT is clear. The cardiovascular and thromboembolic risks appear to be associated with age and time from menopause and risk in this younger population is minimal, especially when transdermal estrogen is used. A small risk of breast cancer in women who have used MHT for more than five years appears to be present, however, the absolute risk does not warrant recommendation against the use of MHT in a population without increased risk of breast cancer. Combination of hormone treatment with lifestyle changes to target other symptoms of menopause is likely to achieve the best outcomes for women with symptomatic menopause. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.