Diabetes and cardiac health: challenges to risk assessment and prevention strategies

Diabetes complications
Heart diseases--prevention
Current recommendations for primary prevention of cardiovascular disease promote risk stratification and management based on estimation of absolute cardiovascular risk. However, this approach has not been adequately tested in people with type 1 diabetes or young people with type 2 diabetes, who may have a longer lifetime exposure to suboptimal cardiovascular risk factors and will therefore require an individualised management approach.
- Cardiovascular disease is the leading cause of death in people with diabetes.
- Current primary prevention strategies focus on assessment of absolute cardiovascular risk and management of risk factors.
- Gaps in the evidence regarding absolute cardiovascular risk stratification for people with type 1 diabetes and young people with type 2 diabetes means that individual cardiovascular risk factor assessment and management is still advocated.
- A multidisciplinary approach to the prevention of cardiovascular disease should be applied in all patients with diabetes wherever possible.
Picture credit: © Berc/stock.adobe.com Model used for illustrative purposes only
Cardiovascular disease (CVD) is the leading cause of death in Australia among patients with diabetes.1,2 In response to the pervasive nature of CVD, particularly in high-risk groups such as people with diabetes, the National Vascular Disease Prevention Alliance (NVDPA) comprised of Diabetes Australia, the National Heart Foundation of Australia, Kidney Health Australia and the National Stroke Foundation was formed with a shared vision to reduce the burden of CVD.1 This alliance has been instrumental in drawing focus to the absolute risk stratification paradigm for CVD management in Australia. This move is echoed internationally with the acknowledgement that multiple risk factors contribute to an individual’s overall absolute CVD risk synergistically rather than in an additive fashion.3,4
This article discusses primary prevention of CVD using absolute risk stratification, as well as addressing gaps in the evidence relating to people with type 1 diabetes and young people with type 2 diabetes. Individualisation of management targets and the role of new glucose-lowering therapies are also addressed.
Calculating CVD risk in diabetes
An Australian risk calculator (available online at www.cvdcheck.org.au) was developed by the NVDPA in 2012 using the Framingham Risk Equation.1 In adults 45 years of age and older (or ≥35 years for Aboriginal and Torres Strait Islander people), this calculator estimates the absolute risk of a first cardiovascular event over the next five years.1 The estimated absolute risk is then stratified as high (>15% risk), moderate (10 to 15% risk) or low (<10% risk) to guide risk-factor management.1
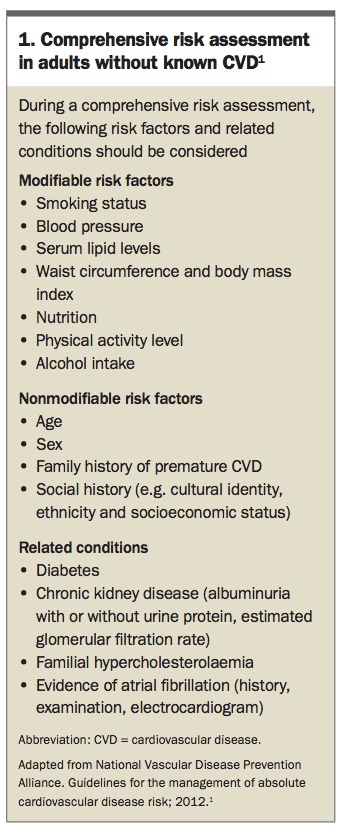
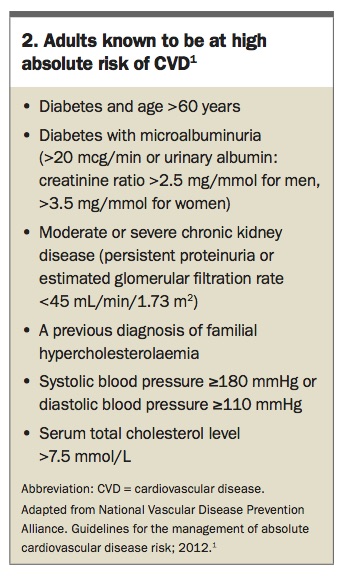
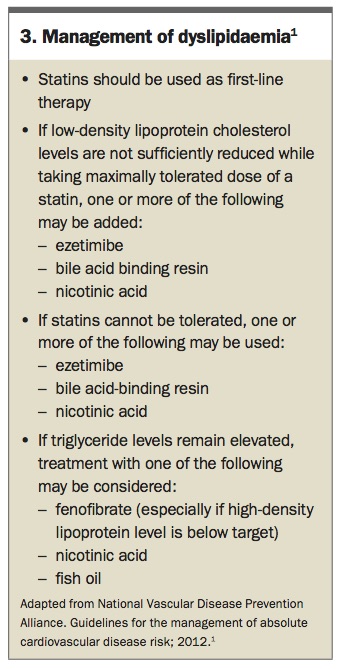
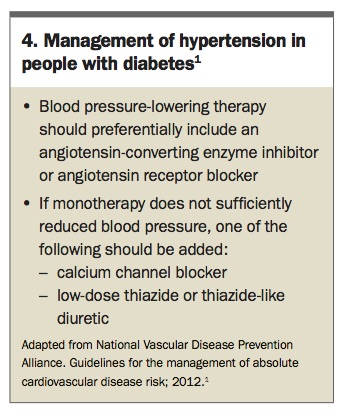
As part of a comprehensive risk assessment (Box 1), the Australian risk calculator helps to develop tailored approaches to subsequent management.1 However, some patients are already known to be at high absolute risk of CVD and can be managed accordingly without a numerical estimation of absolute risk (see Box 2).1,5,6 The key components of CVD management are lifestyle changes, pharmacotherapy, treatment targets, monitoring clinical parameters and calculating absolute risk.1 Optimal lifestyle behaviours, including smoking cessation, adherence to dietary and physical activity recommendations and avoiding excessive alcohol intake, are recommended for all patients regardless of the level of absolute risk.1 In contrast, use of pharmacotherapy is introduced depending on the level of risk, with emphasis on the central role of lipid lowering with statin therapy (Box 3) and blood pressure lowering with blockade of the renin–angiotensin–aldosterone system particularly for patients with diabetes (Box 4).1 A detailed discussion of management strategies can be found in the NVDPA’s guidelines on the management of absolute cardiovascular risk.1
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Challenges to CVD risk assessment and prevention strategies in diabetes
Diabetes approximately doubles the risk of developing CVD.1 However, although the contribution of diabetes per se to increased cardiovascular risk is well established, the intensity and method by which to manage glycaemic control and its impact on absolute risk continues to be debated.
Use of CVD risk calculators
Much of the existing guidance on CVD risk stratification and management of people with type 1 diabetes or those with type 2 diabetes aged under 45 years is based on evidence from mid-to-older aged populations with type 2 diabetes.7-11 The risk calculator developed by the NVDPA uses the Framingham Risk Equation which has been reported to be a poor predictor of events in patients with type 1 diabetes, and to generally underestimate CVD risk in populations with diabetes.1,5,6 It also lacks consideration of the duration of exposure to various risk factors which may be of particular relevance to younger patients.9 Furthermore, the calculator is not applicable to people under 45 years of age (or <35 years for Aboriginal or Torres Strait Islander people).1 This is an issue as people with type 1 diabetes experience cardiovascular events about 10 years earlier than a matched population without diabetes, and have an age-adjusted relative risk of CVD of up to 10 times that of the general population.9
Current guidelines are therefore unable to provide an adequate approach to risk stratification and management for people with type 1 diabetes or those with type 2 diabetes younger than 45 years of age. A practical approach may be to acknowledge gaps in the evidence and recognise that applying the risk calculator to these groups will provide at most a conservative estimate of absolute CVD risk. In combination with clinical judgment, specialist referral and individual patient preferences, CVD risk factors may then be addressed using a tailored approach.
Effects of intensity of glycaemic control
The role of intensive therapy to lower blood glucose levels in patients with type 2 diabetes has yielded moderate benefits with regards to CVD. This is notable by comparison to patients with type 1 diabetes in whom there is strong evidence of substantial benefits.
The landmark Diabetes Control and Complications Trial (DCCT) and follow up Epidemiology of Diabetes Interventions and Complications (EDIC) study have led the call for intensive management of glycaemia for all patients with type 1 diabetes after reporting clear reductions in microvascular complications and cardiovascular events persisting after 30 years of follow up.12,13
In contrast, the United Kingdom Prospective Diabetes Study (UKPDS) investigating the effects of more versus less intensive glycaemic control (achieving an HbA1c of 7.0% vs 7.9% [53 vs 63 mmol/mol] at the end of follow up) in patients with newly diagnosed type 2 diabetes did not demonstrate a significant reduction in CVD events at the completion of the trial.14,15 However, after an additional observational follow up of 10 years, a significantly decreased risk of myocardial infarctions and death from any cause were observed.14
Further trials of patients with type 2 diabetes, including the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial, the Action in Diabetes and Vascular Disease: Preterax and Diamicron MR Controlled Evaluation (ADVANCE) trial and the Veterans Affairs Diabetes Trial (VADT), have failed to separately demonstrate clear benefit of more (targeting HbA1c levels <6.5% [<48 mmol/mol]) versus less intensive glycaemic control on cardiovascular outcomes.16-19 Quite unexpectedly, the ACCORD trial also reported increased mortality risk with more intensive therapy.17 Results combined in subsequent meta-analyses demonstrated a modest reduction in risk of major CVD events and microvascular complications without significant impact on all-cause mortality.19,20
Taken together the findings of these randomised trials as well as the management strategies used may be important for individualisation of glucose management. For example, intensive therapy after diagnosis may be safer than later on, caution may need to be applied to the speed of glycaemic improvement in older patients, hypoglycaemia may limit titration of therapy, and weight gain with therapy intensification may be counterproductive when managing cardiovascular risk.16-19 Overall, an intensive approach to glycaemic control reduces risk of CVD regardless of diabetes type, and should be offered to most patients with type 1 and many patients with type 2 diabetes.
The role of new glucose-lowering therapies in type 2 diabetes
More recent trials are reporting cardiovascular benefit of some glucose-lowering therapies, independent of glycaemic impact.21 Rather than considering primary prevention of CVD most of these studies have been designed as noninferiority trials to determine cardiovascular safety in patients with pre-existing CVD and type 2 diabetes. Perhaps the strongest evidence for cardiovascular benefit comes from the Empagliflozin, Cardiovascular Outcome Event Trial in Type 2 Diabetes Mellitus Patients (EMPA-REG OUTCOME) trial.22 Not only did empagliflozin meet the prespecified noninferiority margin for cardiovascular safety, but it also demonstrated reduced cardiovascular and all-cause mortality.22 Empagliflozin has subsequently become the first oral antihyperglycaemic agent to receive Therapeutic Goods Administration approval for the prevention of cardiovascular death.23
Promising results also come from the Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes (CANVAS) Program.24 In patients with pre-existing CVD or in those at high cardiovascular risk (≥50 years of age with two or more trial-defined risk factors), canagliflozin met both noninferiority and superiority margins for the primary composite outcome of death from cardiovascular causes, nonfatal myocardial infarction or nonfatal stroke.24 However, concerns regarding increased rates of foot amputation and fracture are being further examined as well as differences among the agents within the class of sodium glucose cotransporter-2 inhibitors.24
Glucagon-like peptide-1 (GLP-1) receptor agonists have also demonstrated cardiovascular safety, and perhaps a role in CVD secondary prevention.21 The Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes (LEADER), Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes (SUSTAIN-6), and Lixisenatide in Patients with Type 2 Diabetes and Acute Coronary Syndrome (ELIXA) trials met their respective noninferiority margins, with the former two trials reporting reduced cardiovascular morbidity in people with pre-existing CVD (semaglutide is currently not available in Australia).25-27 However, only the LEADER study was powered to demonstrate superiority.25 A recent meta-analysis of 189 trials of incretin-based therapies has reported the possibility of a mortality benefit with use of GLP-1 agonists.28 Tempered by a potential negative impact on microvascular complications and inconsistent CVD findings, further studies aim to clarify the role of GLP-1 agonists beyond improvements in glycaemia and weight reduction.21
Individual targets
Although an integrated approach to absolute CVD risk is advocated, it should not occur at the expense of management of individual risk factor levels.1 Increasing blood pressure, high cholesterol levels and poor glycaemic control, for example, each have independently positive associations with cardiovascular risk.1 Therefore, although management decisions should focus on the over-arching ‘absolute risk’ profile, monitoring should also focus on individual risk factor levels.1 These need to be tailored to each patient considering the benefits and risks, as well as patient acceptability.
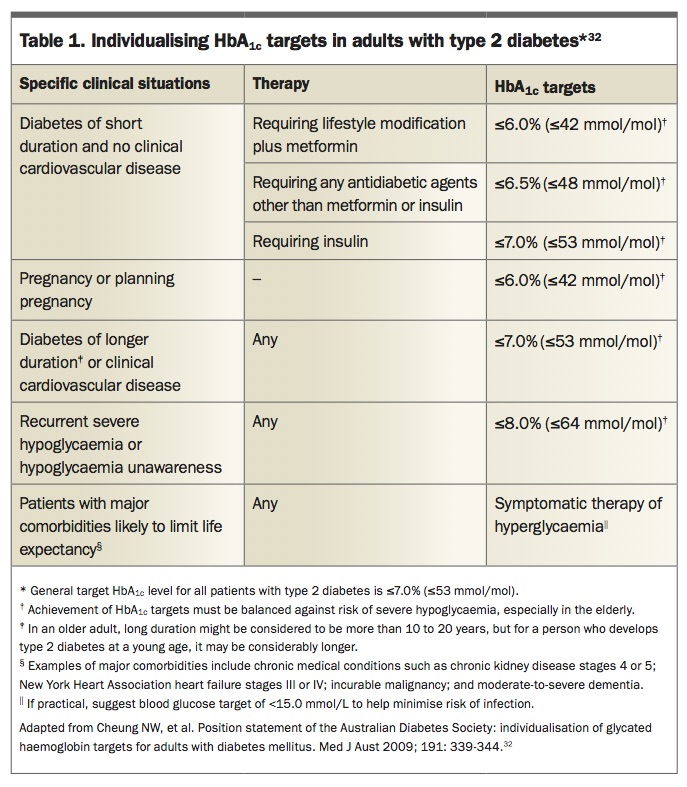
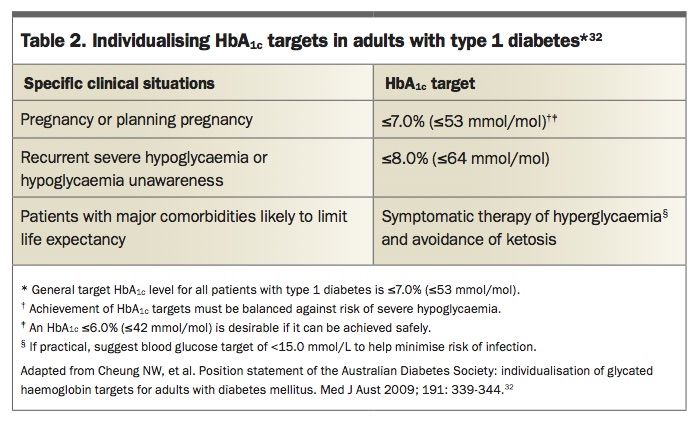
Important changes to recommendations on treatment include the more relaxed optimal blood pressure target (<140/90 mmHg) and the individualisation of HbA1c targets.29 However, consideration must be given to the need for lower blood pressure targets in younger patients with diabetes, patients with albuminuria and patients at high risk of stroke.29,30 Similarly, consideration must be given to the need for lower HbA1c targets for patients with type 1 diabetes, younger patients with type 2 diabetes and women with diabetes who are of reproductive age planning pregnancy,31,32 as well as higher HbA1c targets for patients with frequent or severe hypoglycaemia, those with comorbidities and those who are frail (Table 1 and Table 2).29,32
{kind=link}
{kind=link}
A multidisciplinary care approach
The Royal Australian College of General Practitioners have published guidelines and a structured patient-centred care plan to facilitate an integrated approach to diabetes management as well as cardiovascular risk assessment.29 Further discussion of management strategies can be found in the NVDPA guidelines for the management of absolute cardiovascular risk.1 Referral of complex patients to relevant subspecialist physicians and allied healthcare professionals may also assist in addressing relevant CVD risk factors and aid risk stratification. This may be of particular relevance to patients whose care is not directly addressed by current guidelines and relies more on integration and communication of developing evidence as it pertains to the care of individual patients.
Conclusion
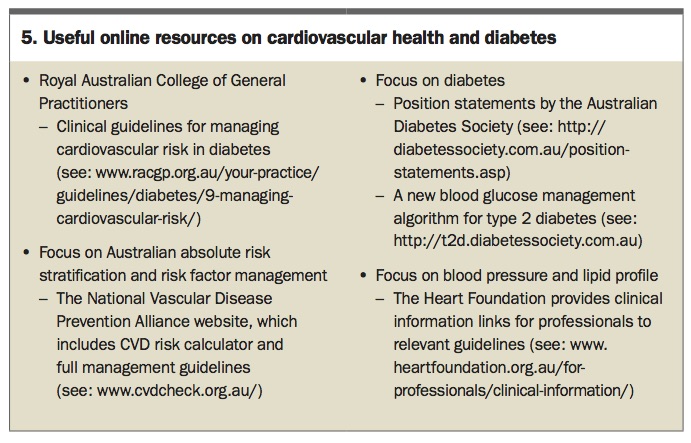
Prevention of CVD has moved to a paradigm of risk stratification and management based on estimation of absolute cardiovascular risk. Diabetes is a major driver of CVD and by virtue of its multisystem effects requires a broad and comprehensive management strategy (see Box 5 for some useful online resources). Available evidence has led to the development of absolute cardiovascular risk calculators that provide a good approach to stratifying risk. Patients with type 1 diabetes and young patients with type 2 diabetes may require particular consideration and a more individualised approach. Given the complex interplay between different risk factors and treatments in patients with diabetes, a multidisciplinary team approach is advocated. ET
{kind=link}
Professor Zoungas has participated on the advisory boards and/or received honoraria from AstraZeneca/Bristol-Myers Squibb, Eli Lilly, Janssen-Cilag, Merck Sharp & Dohme, Sanofi Aventis, Novo Nordisk, Servier Laboratories and Takeda Pharmaceuticals Australia Pty Ltd. She also holds a NHMRC Senior Research Fellowship.
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.