Solid organ transplantation and endocrine sequelae. What to be aware of

Organ transplantation
Endocrine diseases
Recipients of solid organ transplant are managed by a specialist team. However, as the number of transplantations increases and survival improves, the care of these patients will be shared with GPs and other physicians. Endocrine pathology is common after transplantation and requires lifelong monitoring and management.
- Endocrine complications such as diabetes and osteoporosis are common after solid organ transplantation.
- Management of post-transplant diabetes needs to be individualised, but standard monitoring for diabetic complications should be continued.
- If the corticosteroid dose increases, glucose levels should be closely monitored and treatment titrated.
- Osteoporosis is common before and after transplantation, and nonpharmacological management should be optimised, with individualised therapeutic treatment.
- If a fracture occurs in a patient, osteoporosis management should be reassessed.
Solid organ transplantation (kidney, liver, heart and lung) is an increasingly common management option for end-stage organ disease. In Australia, there are an average of 1200 solid organ transplant recipients per year.1 In 2019, 857 kidney transplants, 308 liver transplants, 113 heart transplants and 183 lung transplants were performed in Australia.1 Graft survival rates continue to improve, with Australian five-year survival at 74 to 87%.2 Subsequently, management of long-term complications is increasingly important. Endocrine complications are common and include diabetes, obesity and osteoporosis.
Post-transplant diabetes mellitus
Diagnosis of diabetes
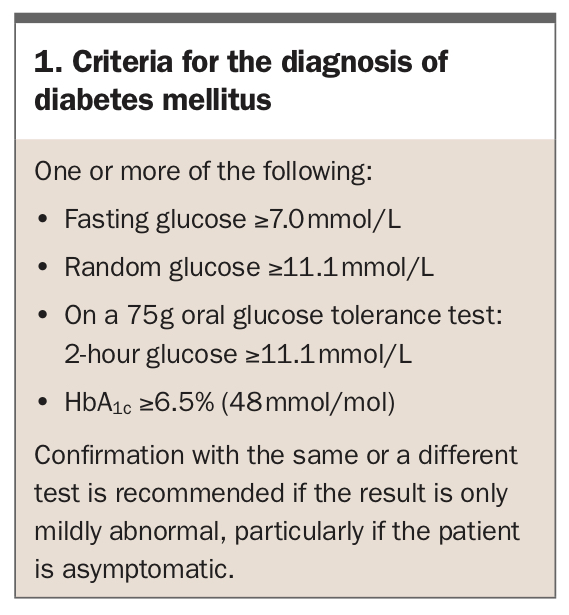
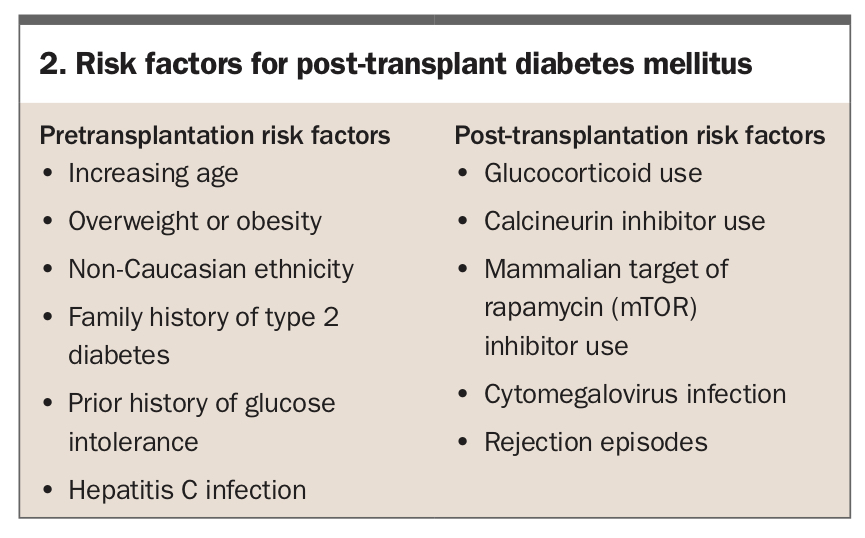
The diagnosis of diabetes mellitus is made when two pathology tests demonstrate hyperglycaemia, as defined in Box 1.3,4 Patients may have a diagnosis of diabetes before solid organ transplantation and may have steroid-induced hyperglycaemia after transplantation. Patients without a prior diagnosis of diabetes will likely develop hyperglycaemia in the early post-transplant period, which may be transient. Risk factors for post-transplant diabetes mellitus (PTDM) are shown in Box 2.
{kind=link}
{kind=link}
An international consensus meeting on PTDM recommended delaying screening and making a definitive diagnosis of PTDM for at least 45 days after transplantation, as transient post-transplant hyperglycaemia often resolves after rationalisation of immunosuppression regimens.5
The oral glucose tolerance test (OGTT) is the gold standard tool for the diagnosis of PTDM.5,6 Because the nature of PTDM is to cause increased postprandial hyperglycaemia, the OGTT identifies more patients with PTDM than fasting glucose measurement alone.7,8 The OGTT also allows identification of impaired glucose tolerance, a precursor to the development of type 2 diabetes and PTDM. The OGTT should ideally be performed when the patient is treated with a stable maintenance dose of glucocorticoid therapy. Glycated haemoglobin (HbA1c) is a convenient test for screening for diabetes but has several limitations in the diagnosis of PTDM. The use of HbA1c testing should be limited to screening patients who are not treated with glucocorticoids (e.g. before transplantation) and who have a low clinical suspicion of diabetes.
Management of diabetes in the post-transplant patient
Immediate post-transplant phase (0 to 45 days)
Insulin is the mainstay of therapy for hyperglycaemia in the immediate post-transplant phase because of its immediate action and safety profile.9 High-dose glucocorticoids may induce marked insulin resistance. In patients with hyperglycaemia in the postoperative phase, there is some evidence that using basal insulin, rather than bolus insulin as required, can reduce the risk of developing PTDM, which may be due to less glucose toxicity and/or beta-cell rest.10,11
Later post-transplant phase (>45 days)
Lifestyle modification remains an important factor in the long-term management of diabetes after transplantation. Addressing lifestyle factors such as diet and physical activity with a dietitian and exercise physiologist, respectively, has been shown to improve glycaemic control in transplant recipients.12
Pharmacological therapy, if needed, is tailored to the individual. No specific algorithm has been developed, and it should be initiated in conjunction with the transplant team if possible.
Metformin is first-line therapy for the management of type 2 diabetes and can be used in post-transplant patients with preserved renal function. As with all patients on metformin, it is important to titrate the dose to renal function and withhold when contrast agents are used. Monitoring of vitamin B12 levels by the GP is recommended. There are no known drug interactions between metformin and immunosuppressive agents.13
Gliclazide, a sulfonylurea, has traditionally been used as an alternative to insulin to treat glucocorticoid-induced hyperglycaemia. There is limited evidence on its safety and efficacy in the post-transplant setting. There is a possible interaction with CYP2C9 inhibitors (such as fluconazole, trimethoprim and metronidazole), which may be used to treat infection in solid organ recipients; this can result in reduced metabolism of gliclazide and hence increased exposure and risk of hypoglycaemia.13
Dipeptidyl peptidase-4 (DPP-4) inhibitors have been shown to be safe and effective in the treatment of PTDM.14-17 There is possible interaction between sitagliptin and ciclosporin (increase in ciclosporin trough levels); and vildagliptin and tacrolimus (decrease in tacrolimus trough levels).13 As linagliptin is the only DPP-4 inhibitor that is not renally excreted it does not require renal dose adjustment; in addition, it has no known drug interactions with immunosuppressive agents.
Glucagon-like peptide-1 (GLP-1) receptor agonists have also been shown to be safe and effective in the treatment of PTDM.18 There are no known drug interactions between GLP-1 receptor agonists and immunosuppressive agents.
Sodium-glucose cotransporter-2 (SGLT-2) inhibitors have been used in the treatment of PTDM.19-21 There are no known drug interactions between SGLT-2 inhibitors and immunosuppressive agents. Empagliflozin has been shown to have a protective effect on tacrolimus-induced renal injury.22 However, it should be noted that SGLT-2 inhibitors are not recommended when estimated glomerular filtration rate (eGFR) is less than 30 mL/min/1.73m2. Empagliflozin may have beneficial longer-term benefits in heart transplant recipients.20 As with all patients on SGLT-2 inhibitors, it is important to discuss the risk of euglycaemic diabetic ketoacidosis with the patient. The risk is increased when the patient is fasting for procedures, reducing carbohydrate intake and during intercurrent illness such as infection; hence, patients should be advised to withhold this medication in these situations.
Insulin remains a common treatment modality for PTDM, particularly in the setting of severe hyperglycaemia or renal impairment. The glycaemic profile of PTDM (when prednisone is used in the morning) is postprandial hyperglycaemia, with peak glucose levels in the afternoon and lowest glucose levels in the early morning.6,23 Therefore, choosing an insulin type with a similar profile is recommended, such as human or biosynthetic human isophane insulin used in the morning (Protaphane, Humulin NPH) and rapid-acting insulin with meals if needed. Mixed insulin may also be used at breakfast and supplemental rapid-acting insulin with lunch and, possibly, dinner, although the latter needs to be given with care as glucose levels typically decrease overnight.
If glucocorticoid doses change, or if a patient requires a pulse of corticosteroids for rejection, glucose levels should be closely monitored and treatment will likely need to be escalated. This also applies to a reduction in glucocorticoid dose, as there is risk of hypoglycaemia necessitating a reduction in pharmacological treatment.
Ongoing monitoring
Any patient who is treated with insulin should self-monitor capillary glucose levels. It is also useful to monitor capillary glucose levels when on other diabetic medication. The value of monitoring glucose levels after lunch or before dinner is important when the patient is taking morning prednisone as this is when the peak hyperglycaemic effect occurs. In Australia, the National Diabetes Services Scheme (NDSS) subsidises products including blood glucose testing strips and insulin pen needles. Patients with PTDM should be registered with the NDSS under the category of ‘other’ diabetes, with supporting documentation from an authorised health professional.
Flash glucose monitors and continuous glucose monitors provide extensive information about glucose levels and glucose profiles. These devices are not subsidised for PTDM and need to be privately funded.
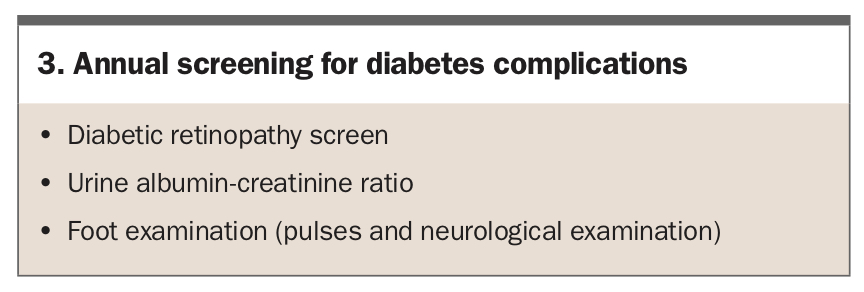
Any patient with diabetes should have an annual review for complications, as listed in Box 3. PTDM is a complex disease in patients with complex comorbidities; hence patients should ideally be assessed by a diabetes team including endocrinologists and diabetes educators.
{kind=link}
Fitness to drive
Patients with PTDM are subject to the same driver licensing rules as any other patient with diabetes. Advice about restrictions and Australian medical requirements for unconditional and conditional licences can be found in the Austroads guidelines.24
Weight gain and obesity
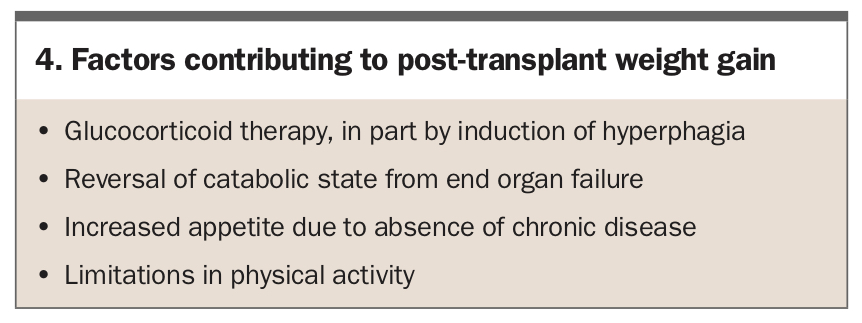
Weight gain is common after solid organ transplantation, with an increased prevalence of overweight and obesity.11,25-27 Factors contributing to weight gain after receiving a solid organ transplantation are listed in Box 4.
{kind=link}
Healthy dietary choices are important in the postoperative management of transplant patients. Exercise may be limited in the immediate postoperative period and when acute illness or rejection occurs. Information on eating well can be found on the Diabetes Australia website (https://diabetesaustralia.com.au/food-activity/eating-well).
Two classes of diabetic medications, GLP-1 receptor agonists and SGLT-2 inhibitors, have been shown to reduce weight in transplant patients with diabetes.18,19 In nontransplant patients, there is evidence that GLP-1 receptor agonists are safe and effective for weight loss in nondiabetic patients with obesity.28 However, in Australia, GLP-1 receptor agonists are only subsidised by the PBS for management of type 2 diabetes. Liraglutide (as Saxenda) is the only approved weight loss GLP-1 agonist medication in nondiabetic patients.
Bariatric surgery has been reported as a therapeutic option in renal and liver transplant patients.29,30
Bone health
Patients undergoing solid organ transplantation often already have low bone mineral density and increased risk of fracture prior to transplantation.31,32 Assessing bone health should be included in solid organ transplantation work up. Bone mineral density should be assessed through dual-energy x-ray absorptiometry. Trabecular bone score has been used to assess bone microarchitecture in renal transplant patients but is also not routinely available.33 Following solid organ transplantation, immunosuppressive agents further contribute to deterioration in bone health.34
Management of osteoporosis before transplantation
Treatment of osteoporosis should be considered before transplantation, as renal dysfunction after transplantation may limit therapeutic options. General guidelines by the International Society for Heart and Lung Transplantation, the American Association for the Study of Liver Disease and the Kidney Disease Improving Global Outcomes Transplant Work Group include the treatment of osteoporosis.35-37
Management of osteoporosis after transplantation
After transplantation, nonpharmacological measures for managing osteoporosis including weight-bearing exercise and adequate dietary calcium intake should be optimised. Many post-transplant protocols include oral calcium supplementation.
Vitamin D deficiency is common in transplant recipients and is contributed to by poor nutrition, limited sunlight exposure and glucocorticoid use.38,39 Most patients are started on maintenance therapy of cholecalciferol 1000 units daily. Vitamin D levels should be monitored to ensure a level of at least greater than 50 nmol/L, particularly before considering bisphosphonate therapy.40
Bisphosphonate therapy has a strong evidence base for the prevention and treatment of osteoporosis after solid organ transplantation.39 There are no clear guidelines on the optimal bisphosphonate and the timing. Zoledronic acid is often used because of prolonged bone turnover suppression. Dental review before starting bisphosphonate therapy is recommended.
Denosumab has limited evidence regarding its efficacy and safety in the treatment of post-transplant osteoporosis.41,42 It must be stressed that if denosumab is used then there must be strict six-monthly administration. It should also be noted that there is an increased risk of hypocalcaemia with renal impairment or when vitamin D levels are not adequate, so these require monitoring. Dental review before starting denosumab therapy is recommended.
Teriparatide (recombinant parathyroid hormone) is not routinely used in transplant patients. There is evidence that teriparatide is effective in treating glucocorticoid-induced osteoporosis; however, this was not reflected in a study of renal transplant recipients.43,44
Romozosumab (monoclonal antibody against sclerostin) has not been studied in transplant patients or in patients with glucocorticoid- induced osteoporosis.
Calcitriol (1,25-dihydroxycholecalciferol, activated vitamin D) has limited evidence for the treatment of post-transplant osteoporosis.45,46 This may be a treatment option used in renal impairment, but careful monitoring of serum calcium concentration is required.
Notification of the occurrence of a fracture is important. If a fracture occurs in a transplant patient, management of osteoporosis needs to be reassessed and should be escalated to an endocrinologist. Key points in the management of bone health after transplantation are shown in Box 5.
{kind=link}
Thyroid disease
Thyroid dysfunction can occur after transplantation in the context of medications and acute illness. Thyroid function tests should be requested if symptoms of hyper- or hypothyroidism are present. Amiodarone, an antiarrhythmic medication, is often used to treat atrial fibrillation and can cause hyper- and hypothyroidism.47 Glucocorticoids can reduce thyroid function through reduced conversion of thyroxine (T4) to triiodothyronine (T3), and through reduced thyroid stimulating hormone production.48,49 Hyperthyroidism should be investigated to determine the underlying aetiology, with a measurement of thyroid receptor antibody, which will be positive in Graves’ disease.50 A nuclear medicine technetium thyroid scan may be required to differentiate Graves’ disease and thyroiditis. Treatment will depend on the underlying aetiology. Hypothyroidism should be treated with thyroxine replacement. Due to the complex nature of thyroid disease in transplant patients, management should be discussed with an endocrinologist.
Conclusion
Endocrine complications are common following solid organ transplantation and should be monitored for. Treatment decisions will normally be made by specialists linked to transplant units. However, as the number of transplant recipients increases and survival outcomes improve, the care of these patients will be shared with GPs. Diabetes treatment is guided by glucose profile and comorbidities and, as with any patient with diabetes, it is important to screen for complications. Diabetic management needs reassessment when glucocorticoid dose is changed. Osteoporosis is common before and after solid organ transplantation, and treatment should be individualised. ET
COMPETING INTERESTS: None.