Stefan, a 50-year-old man, presents to you with a new onset of unexplained weight loss and palpitations over the past two months. He reports that he often feels his pulse has been racing and that he has been getting quite sweaty and agitated at times when this occurs. In addition, he has observed increased swelling in his ankles over the past couple of weeks and states that he feels hot and flushed most of the time. There has been associated diarrhoea but no chest pain, dyspnoea or abdominal symptoms. He denies infective symptoms. His past medical history includes atrial fibrillation, for which he has been taking amiodarone for 10 years, and hypertension.
He has had some thyroid function tests (TFTs), which showed the following results:
- thyroid stimulating hormone (TSH) level of 0.004 mIU/L (reference range [RR], 0.40 to 4.00 mIU/L)
- free thyroxine (FT4) level of 32 pmol/L (RR, 9.0 to 19.0 pmol/L)
- free triiodothyronine (FT3) level of 7.5 pmol/L (RR, 2.6 to 6.0 pmol/L).
Autoantibody testing showed an antithyroglobulin level of 25 kIU/L (RR, below 4 kIU/L) and antithyroperoxidase level of 50 kIU/L (RR, below 5.6 kIU/L). His TSH receptor antibody test result was negative.
What are your main concerns for Stefan?
Answer: Although there are multiple differential diagnoses for Stefan’s presentation, the main concern is amiodarone-induced thyroiditis (AIT) and the possibility that he may develop thyroid storm. His TFTs showed a suppressed TSH level with a high FT4 level and he has had ongoing symptoms for two months. Thyroid storm is a concerning manifestation of thyrotoxicosis and often involves multiple organ systems, including the cardiovascular, gastrointestinal and central nervous systems. Stefan’s history shows that he is already demonstrating certain features from several of these domains, which suggests he is at risk of deteriorating rapidly. He does not have antibodies to the TSH receptor, which are commonly seen in Graves’ disease, and this is an important consideration in this case (and is discussed later). Another concern is that differentiating between type I and type II AIT is often difficult and, as the management for these conditions is different, patients are often commenced on combination therapy initially.
Advertisement
What key features should you assess for on physical examination?
Answer: The first step is to check Stefan’s vital signs to assess if he is acutely unwell. Then proceed with cardiorespiratory and abdominal examinations, as well as examining the thyroid gland and looking for peripheral signs of hyperthyroidism, which should also include an assessment for proximal myopathy. Additionally, look for signs of cardiac failure, as he has new peripheral oedema.
Stefan is of medium build with a body mass index of 24 kg/m2. He has mild proximal myopathy. His pulse is irregularly irregular, with a heart rate of 110 beats per minute, and his blood pressure is 140/85 mmHg. He is otherwise comfortable, with warm peripheries. Cardiorespiratory examination reveals dual heart sounds without any murmurs. There are occasional crepitations at the lung bases. Abdominal examination findings are normal. There is bilateral peripheral pitting oedema below the ankles. On examination of the neck, there is a goitre which is nontender. There is no thyroid bruit or palpable cervical lymphadenopathy.
An early diagnosis is required to prevent the development of more severe forms of thyroid disease, such as a thyroid storm.
How is hyperthyroidism defined and what are some causes?
Answer: Hyperthyroidism can be classified as subclinical or overt, based on TFTs. Overt hyperthyroidism is diagnosed by low serum TSH with high FT3 and/or high FT4 levels and can be caused by the following:
- excess stimulation by trophic factors
- autonomous synthesis and secretion
- excessive passive release of preformed thyroid hormone
- endogenous (either due to metastatic thyroid carcinoma or struma ovarii) or exogenous hormonal excess1
What imaging does Stefan require?
Answer: After biochemical testing has confirmed the presence of hyperthyroidism, and when TSH receptor antibody testing is negative, the usual next step is to perform a thyroid uptake scan. Common causes of hyperthyroidism that can be distinguished using this scan include Graves’ disease, which would show increased uptake; toxic nodule, which would show patchy uptake; and thyroiditis, which would show low uptake.2 Stefan’s thyroid uptake scan reveals low uptake throughout the gland, which is consistent with AIT, but does not distinguish between type I or II.
Generally, ultrasonography has less utility in determining the cause of hyperthyroidism, but in the case of a possible false negative due to iodine, it may offer additional informtion, including the vascularity of the gland using colour flow doppler and the presence of abnormal nodules. Stefan’s ultrasound scan reveals a grossly enlarged thyroid with increased vascularity and no discrete solid nodules.
Advertisement
How does amiodarone affect the thyroid gland?
Answer: Amiodarone can cause both hypothyroidism and hyperthyroidism due to the iodine load. There are two main types of AIT, type I and type II. Type I AIT occurs when deiodination of amiodarone leads to a high organic iodide concentration, resulting in increased iodine availability and subsequent synthesis of thyroid hormone in the presence of underlying thyroid disease such as a toxic multinodular goitre or Graves’ disease. Often thyroid autoantibodies will be present.2,3
In type II AIT, an inflammatory state is created when excess iodine results in the production of organic metabolites of amiodarone.3 There is usually no underlying thyroid disease, instead the amiodarone has a direct toxic effect on the thyroid follicular epithelial cells resulting in a release of thyroid hormones T3 and T4, also known as destructive thyroiditis.3,4 It can be challenging to distinguish between the two types, though it is important to do so as this may determine the treatment and long-term prognosis of AIT. Some patients may have a combination of type I and type II AIT.
How would you manage Stefan in the first instance for his AIT-induced hyperthyroidism?
Answer: As Stefan likely has type I AIT, management in the first instance will involve initiating antithyroid drugs at a dose appropriate to his thyroid function, with a view to titrating as tolerated. Usually, endocrinologists will start with a higher dose (around 20 to 40 mg daily of carbimazole in split doses) when managing Graves’ disease, toxic nodules, or AIT that is likely type I because of drug resistance in iodine-induced hyperthyroidism, then titrate down after the first month.5,6 If patients with AIT are symptomatic, consider upfront addition of corticosteroids, directed at the management of AIT type II and at reducing inflammation. Typically, prednisone at 40 mg daily is commenced in these patients initially.4 Stefan should also be on a maximal dose of a beta-blocker, with noncardiac specific propranolol or atenolol as the preferred options.4,5
The elimination half-life of amiodarone is about 100 days; therefore, ceasing it will not bring an immediate benefit to the patient and the possibility for further episodes of hyperthyroidism or a relapse can last up to six months after its cessation.3,5 If amiodarone is not being used for a life-threatening arrhythmia, then the recommendation is to discuss switching to an alternative antiarrhythmic with the patient’s cardiologist.3,4 Seeking advice from an endocrinologist early in the management of AIT is also important, particularly to prevent progression to thyroid storm.
Carbimazole is the recommended first-line antithyroid therapy as it has a more favourable side effect profile and a longer half-life than other drugs in this class.3 However, because of carbimazole’s modest teratogenic effects, propylthiouracil is preferred for pregnant patients in the first trimester. Concerning side effects of these classes of medications include jaundice, vasculitis and agranulocytosis. Additionally, ongoing use of methimazole, a drug in the same class as carbimazole but not available in Australia, has recently been associated with an increased risk of acute pancreatitis; however, this risk has not been demonstrated with propylthiouracil.6
For patients with AIT who are refractory to corticosteroid and first-line carbimazole therapy, rapid escalation of dosing may be required. Once response to the medical treatment has been observed, monitoring typically involves repeat blood tests including full blood count, liver function and thyroid function at two weeks, and then repeat TFTs every six- to 12-weekly, and as clinically indicated thereafter. Initially, the serum TSH level may remain suppressed for several months so titration of antithyroid therapy is based on the FT3 and FT4 levels.1,3-5
Advertisement
Stefan is reviewed two weeks later. He was initially commenced on carbimazole at 15 mg three times daily and propranolol at 20 mg twice daily but became breathless and stopped all his medications a week ago. He continues to report palpitations and proximal myopathy and has now developed a fine tremor in both hands. A repeat eye examination demonstrates an appreciable lid lag. Also, he has noticed around 5 kg of unintended weight loss during this period. His heart rate is now an irregular 150 beats per minute, blood pressure 90/60 mmHg and he has a temperature of 38.8 degrees. You have repeated his TFTs, which show:
- TSH levels below 0.001 mIU/L
- FT4 level of 80.4 pmol/L
- FT3 level of 12 pmol/L
What is a thyroid storm?
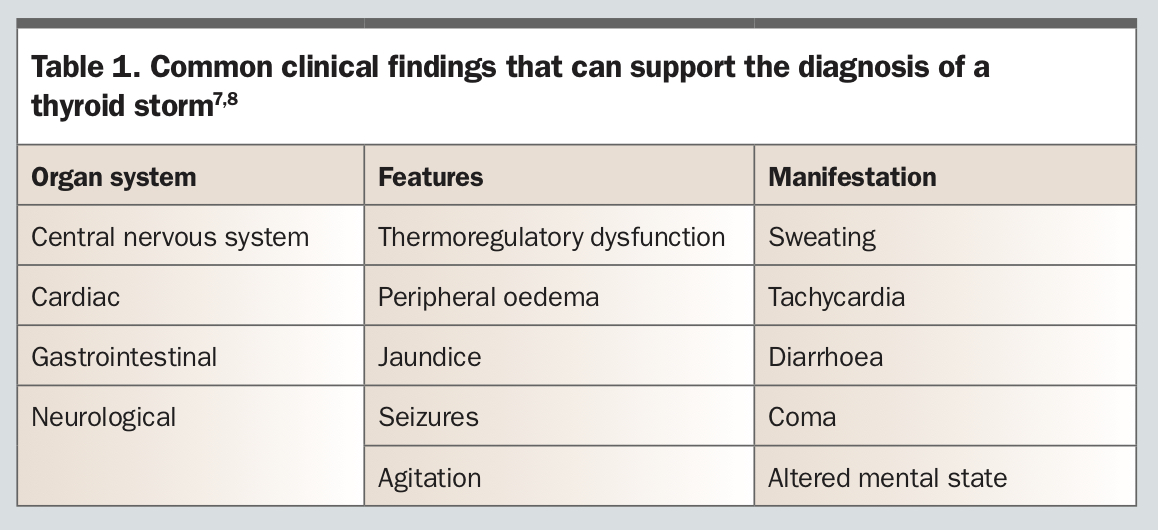
Answer: A thyroid storm is a rare manifestation within the spectrum of thyrotoxicosis, with mortality estimated at 10 to 20%, and constitutes a medical emergency.
7 It is most commonly seen in patients with Graves’ disease but can be seen in any form of hyperthyroidism. Fever is the most common manifestation. Other supporting features are shown in
Table 1.
7,8 There is no specific ‘cut-off’ in TFT levels that delineates between thyrotoxicosis and a thyroid storm; however, it should be noted that it is also important to assess cortisol, as a normal cortisol level can indicate a degree of adrenal insufficiency.
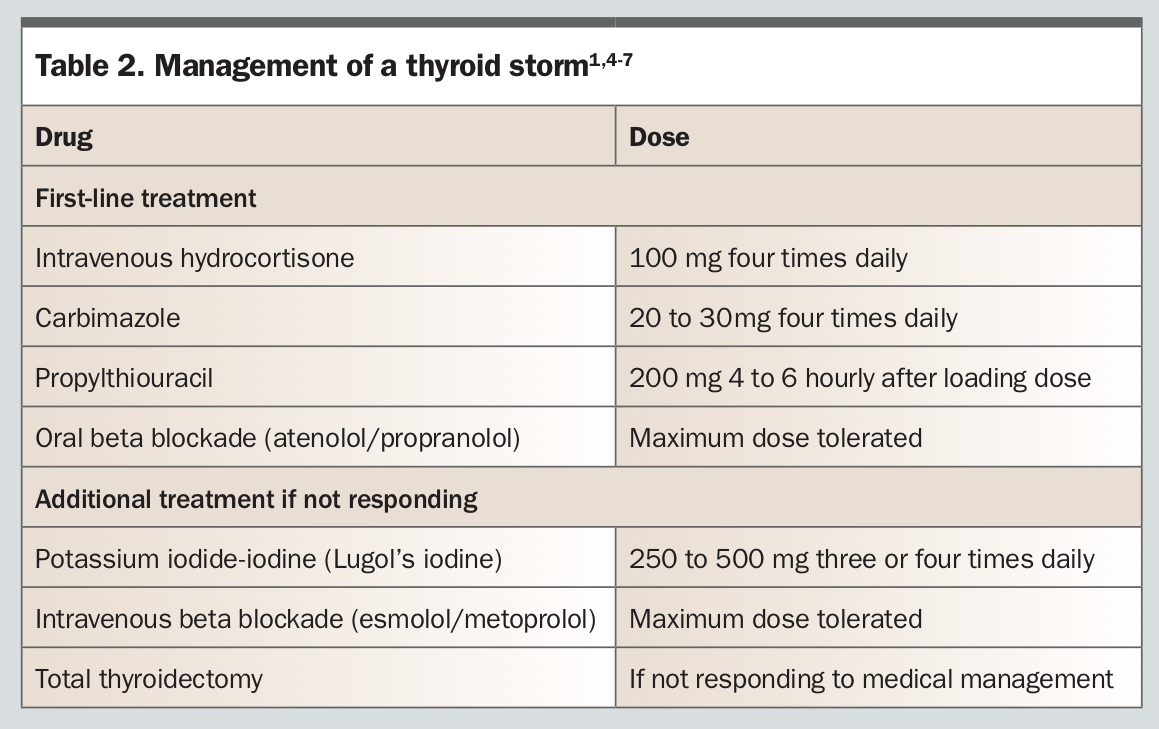
8 Patients should be admitted to hospital for close monitoring and further management (
Table 2).
1,4-7
It may also be pertinent to switch from carbimazole to propylthiouracil, which offers the additional benefit of reduced FT4 to FT3 deiodination, thus reducing the acute effects of hyperthyroidism.9 This is especially beneficial for patients with potential thyroid storm. Finally, if maximal tolerated medical therapy is insufficient in improving outcome, and in the face of haemodynamic instability, presentation and admission to hospital for stabilisation is indicated.
Other therapies to trial in stabilising thyroid function include lithium, cholestyramine (to reduce enterohepatic circulation), haemodialysis and potassium iodide-iodine followed by thyroidectomy.1,3-5,7-9 A relative indication for thyroidectomy may also include reactions to antithyroid drugs, such as agranulocytosis, liver function abnormalities and vasculitis, which are reversible once antithyroid drugs are stopped.
What is the role of a thyroidectomy in AIT?
Answer: In patients whose medical therapy (antithyroid drugs, beta blockade, potassium iodide-iodine, corticosteroids) has not been successful or is not tolerated, surgical management is the next option. It is often indicated in cases of AIT when amiodarone is unable to be withdrawn due to the underlying arrhythmia that is being treated. Surgery has multiple advantages including rapid return to a euthyroid state and removal of iodine stores within the thyroid gland. Total thyroidectomy may be the treatment of last resort, but can proceed once patients are haemodynamically stable.10 The important consideration with perioperative management is to ensure the patient is euthyroid (generally achieved with an antithyroid drug over several weeks, although often not in AIT, especially type II), although iodine can be used if the antithyroid drug is not tolerated. If thyroidectomy is required more urgently, a combination of beta blockade, an antithyroid drug and potassium iodide-iodine should be administered, typically for three days before the procedure.7,8 Potassium iodide-iodine is a combination of elemental iodine, potassium iodide and distilled water that, when used before surgery, can achieve biochemical euthyroidism within five to 10 days through an acute Wolff-Chaikoff effect.11 If a patient is deemed too unstable for surgery, particularly if they are haemodynamically unstable, have severe cardiac failure, ongoing sepsis, severe renal impairment or are too high an anaesthetic risk, then the aforementioned therapies should be trialled in the first instance.
Advertisement
What management does Stefan now require?
Answer: Patients with suspected thyroid storm should be admitted to hospital for monitoring of haemodynamic stability and consideration for thyroidectomy if they deteriorate further regardless of escalation of medical treatment. After thyroidectomy, they can cease taking oral therapies and will require lifelong thyroxine with regular thyroid function monitoring.
See Box for helpful practice points.
Outcome: Stefan’s symptoms combined with his repeat TFTs indicate that he has developed potential thyroid storm, despite being on oral antithyroid therapy for two weeks. He is admitted to hospital and commenced on intravenous hydrocortisone at 100 mg four times daily with intravenous metoprolol at 5 mg. He is haemodynamically unstable and despite intravenous medical management remains agitated and delirious. The decision is made for operative management, so he is administered 10 mL of potassium iodide-iodine and achieves a euthyroid state. He successfully undergoes a total thyroidectomy and is discharged five days later. He is commenced on thyroxine 100 mcg daily with a plan to follow up with an endocrinologist and repeat TFTs in six weeks. ET
COMPETING INTERESTS: None.
References
1. Ross DS, Burch HB, Cooper DS, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis. Thyroid 2016; 10: 1343-1421.
2. Ross DS. Diagnosis of hyperthyroidism. Cooper and Mulder JE, ed. UpToDate: 2019. [login required]
3. Ross DS. Amiodarone and thyroid dysfunction. Cooper and Mulder JE, ed. UpToDate 2020. [login required]
4. Bartalena L, Bogazzi F, Chiovato L, Hubalewska-Dydejczyk A, Links TP, Vanderpump M. 2018 European Thyroid Association (ETA) guidelines for the management of amiodarone-associated thyroid dysfunction. Eur Thyroid J 2018; 7: 55-66.
5. Kolcsár M, Gáll Z. Prevention and treatment of iodine-induced thyrotoxicosis. In: Goiter – causes and treatment. London: IntechOpen; 2019.
6. Brix TH, Lund LC, Henriksen DP, et al. Methimazole and risk of acute pancreatitis. Lancet Diabetes Endocrinol 2020; 8: 187-189.
7. Nayak D, Burman, K. Thyrotoxicosis and thyroid storm. Endocrinol Metab Clin N Am 2006; 35: 663-686.
8. eTG complete. Endocrinology. Thyrotoxicosis and hyperthyroidism. Melbourne: Therapeutic Guidelines Limited; 2019 (updated March 2020). [login required]
9. Ross DS. Thyroid storm. Cooper and Mulder JE, ed. UpToDate: 2020. [login required]
10. Sutherland J, Robinson B, Delbridge L. Anaesthesia for amiodarone-induced thyrotoxicosis: a case review. Anaesth Intensive Care 2001; 29: 24-29.
11. Calissendorff J, Falhammar H. Rescue pre-operative treatment with Lugol’s solution in uncontrolled Graves’ disease. Endocr Connect 2017; 6: 200-205.

{kind=link}
{kind=link}
{kind=link}