Medication-induced thyroid dysfunction: a guide to management

Thyroid diseases
Drug reactions
Medications can affect thyroid hormone production and function or interpretation of thyroid laboratory results. Awareness of these medication effects by GPs allows for early detection of thyroid abnormalities, effective monitoring and prompt intervention when indicated.
- Medications can affect thyroid hormone production and function, or the interpretation of thyroid laboratory results.
- Patients presenting with thyroid dysfunction should be asked about the use of medications, including over-the-counter preparations.
- Thyroid stimulating hormone levels should be measured in all patients before starting a medication that may cause thyroid dysfunction.
- Prompt investigation and appropriate treatment of medication-induced thyroid dysfunction is crucial to limit thyroid-related morbidity.
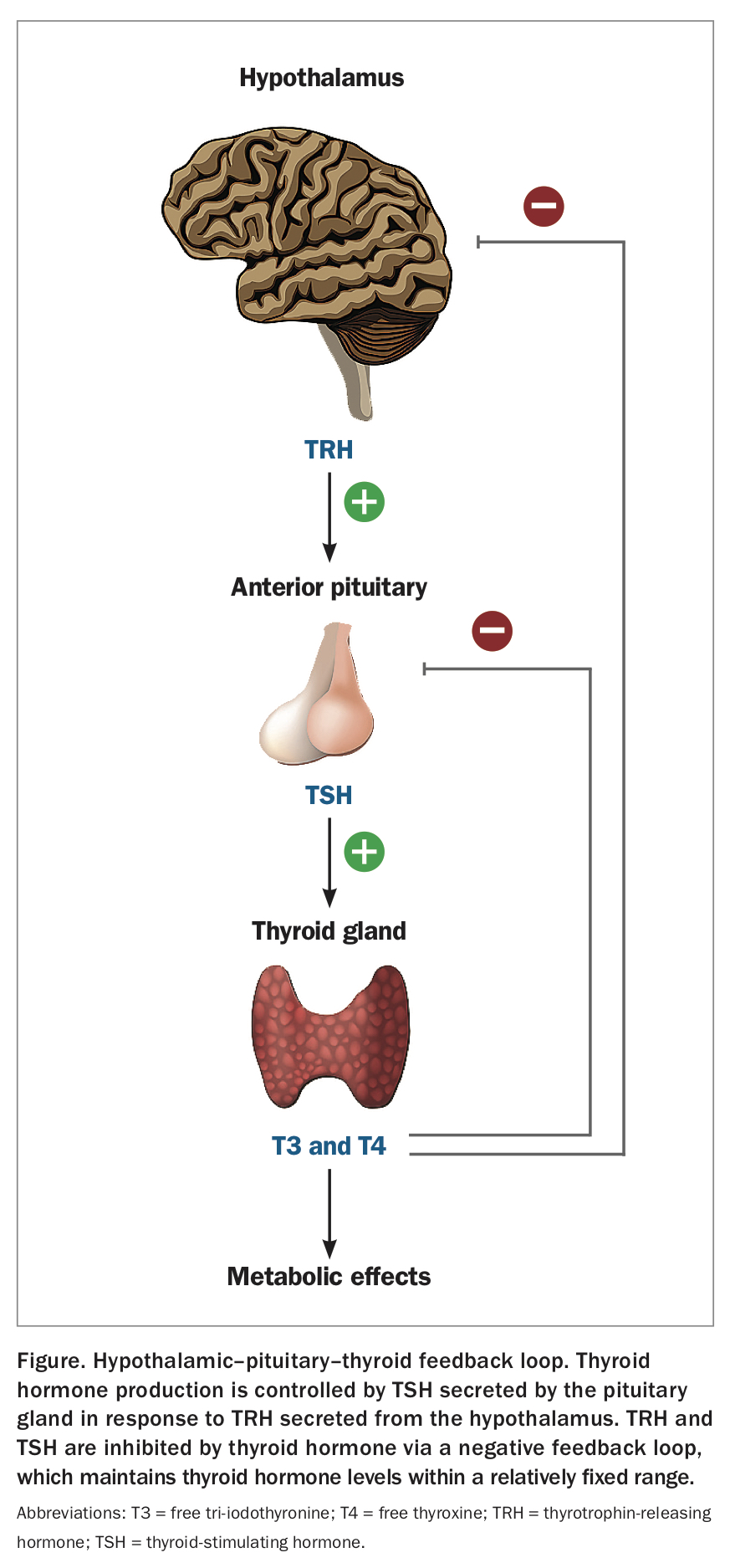
Thyroid hormone synthesis and secretion is regulated by a classic endocrine negative feedback loop (Figure). However, other factors can contribute to the development of thyroid dysfunction. For example, iodine is a crucial component of thyroid hormone synthesis and iodine deficiency can result in progressive hypothyroidism. Exposure to large amounts of iodine can also disrupt thyroid hormone homeostasis and inhibit thyroid hormone production (Wolff-Chaikoff effect) or stimulate thyroid hormone production independent of thyroid stimulating hormone ([TSH] Jod Basedow effect).1
{kind=link}
Numerous medications can cause thyroid dysfunction or interfere with the interpretation of thyroid function tests (TFTs). Each step involved in thyroid hormone synthesis, secretion, transport and metabolism is susceptible to drug interactions.2 Some medications, such as amiodarone and checkpoint inhibitors, can affect multiple steps in this process, whereas biotin-containing compounds can interfere with thyroid function assays resulting in spurious laboratory results.
All patients should be screened for pre-existing thyroid disease by measuring the TSH level before starting on medications that may cause thyroid dysfunction. If the TSH level is abnormal, thyroid hormone levels (free thyroxine [FT4] and free tri-iodothyronine T3 [FT3]) and antithyroid antibodies should be measured. In asymptomatic patients, six-monthly TFT surveillance is sufficient to screen for the development of thyroid dysfunction.
This review focuses on four important medications – amiodarone, lithium, checkpoint inhibitors and biotin-containing products – that may be encountered routinely by GPs in clinical practice.
Medications that can cause thyroid dysfunction
Amiodarone
Amiodarone causes both hypothyroidism and hyperthyroidism, which affects 14 to 18% of treated patients.3,4 Amiodarone is comprised of 37.2% iodine, which is released during its metabolism. A single 200 mg tablet releases 45 times the recommended daily intake of iodine.4
Amiodarone-induced hypothyroidism typically develops within six to 12 months of starting treatment.3 Although it can occur in patients with no underlying thyroid abnormality, the risk is increased in those with abnormal TSH levels before starting amiodarone or positive antithyroid peroxidase antibodies.5 Treatment of amiodarone-induced hypothyroidism is with levothyroxine replacement. After starting levothyroxine, four- to six-weekly thyroid function monitoring is sufficient, with the goal of normalising the TSH level over three to six months.
Amiodarone can induce two distinct types of hyperthyroidism, termed type 1 and type 2 amiodarone-induced thyrotoxicosis. Differentiation between the two subtypes may be difficult, making diagnosis and treatment challenging. A simplified algorithm for screening, diagnosing and managing amiodarone-induced thyroid dysfunction is shown in the Flowchart.
Type 1 amiodarone-induced thyrotoxicosis
Type 1 amiodarone-induced thyrotoxicosis is caused by increased synthesis of thyroid hormone. Typically, this develops in patients with pre-existing or latent subclinical thyroid disease and tends to occur early after amiodarone is started.6 Increased production of thyroid hormone is attributed to the increased availability of iodine from amiodarone, which can provoke hyperthyroidism particularly in the setting of an abnormal gland (e.g. multinodular goitre).
Radioiodine uptake scans are typically unhelpful in the setting of amiodarone because of interference from the high iodine load. However, ultrasound, which usually has no role in the diagnosis of hyperthyroidism, can be beneficial as increased thyroid vascularity is suggestive of the diagnosis.7 Doppler imaging for assessment of thyroid vascularity should be stipulated on the imaging request form, as vascularity is not routinely assessed and may not be reported if not specifically requested.
A trial of antithyroid medication (carbimazole) is first-line treatment for type 1 amiodarone-induced thyrotoxicosis. The starting dose depends on the severity of thyrotoxicosis and in severe cases, doses of up to 15 mg three times daily may be required with prompt referral of the patient to an endocrinologist.
Type 2 amiodarone-induced thyrotoxicosis
Type 2 amiodarone-induced thyrotoxicosis results from toxic effects of amiodarone on the thyroid gland precipitating a destructive thyroiditis. Patients typically have no underlying thyroid disease.8 Clinically, it is characterised by an initial hyperthyroid phase lasting weeks to months, followed by a hypothyroid phase or recovery of normal thyroid function. In contrast to type 1 amiodarone-induced thyrotoxicosis, oral prednisolone, with doses up to 40 mg daily is first-line treatment.5
Management of amiodarone-induced thyrotoxicosis if first-line treatment is suboptimal
A significant proportion of patients with amiodarone-induced thyrotoxicosis have a suboptimal response to initial medical treatment, reported to be up to 48% in one study.9 In these patients, both type 1 and type 2 amiodarone effects may be present and cotreatment with antithyroid medication and prednisone should be trialled. Additionally, in very sick patients or if an ultrasound cannot be obtained, dual treatment with both carbimazole and corticosteroids should be strongly considered. Endocrinology input is recommended. In most cases, there is no immediate benefit to stopping amiodarone because of its long half-life of about 100 days.10 In severe cases or if there is failure to respond to medical treatment, urgent thyroidectomy should be considered early.
Lithium
Lithium causes hypothyroidism in up to 20% of patients through inhibition of thyroid hormone release from the thyroid gland.11 It is important to monitor a patient’s mental state closely, as thyroid dysfunction may exacerbate or destabilise psychiatric symptoms. Female sex, age over 40 years and positive thyroid peroxidase antibodies are associated with increased risk of lithium-related thyroid dysfunction.12 Levothyroxine replacement (1.0 to 1.5 mcg/kg/day) should be initiated in symptomatic patients with biochemical hypothyroidism (elevated TSH level, low FT4 level) and strongly considered in subclinical hypothyroidism, particularly if the TSH level is over 10 mIU/L, irrespective of FT4 and FT3 levels.
Immune checkpoint inhibitors
Immune checkpoint inhibitors have become standard of care in multiple cancer subtypes and are now in widespread clinical use. The most frequently used checkpoint inhibitors include: ipilimumab (CTLA-4 inhibitor); nivolumab and pembrolizumab (PD-1 inhibitors); and atezolizumab, avelumab and durvalumab (PD-L1 inhibitors). Treatment with checkpoint inhibitors can be associated with development of immune-related adverse events in multiple organ systems, although the thyroid is particularly susceptible.13
Up to 40% of patients treated with checkpoint inhibitors develop thyroid dysfunction, particularly when PD-1 and CTLA-4 inhibitors are used in combination.14 Both hyperthyroidism and hypothyroidism can occur. In most patients, no treatment is required, and checkpoint inhibitors can be continued during the period of thyroid dysfunction. The most frequent presentation is transient thyrotoxicosis, developing one to two months after treatment initiation.14 Many of these patients (about 50%) will progress to hypothyroidism after four to six weeks, which is often permanent. Levothyroxine replacement should be started in patients with a TSH level above 10 mIU/L, as the likelihood of recovery in this setting is rare.14 After the first six months of treatment, annual testing of thyroid function is sufficient in asymptomatic patients to identify uncommon cases of late-onset hypothyroidism without a preceding thyrotoxic phase.13
Alemtuzumab
Alemtuzumab, a monoclonal antibody used to treat relapsing-remitting multiple sclerosis, rapidly depletes lymphocytes through inhibition of its target, CD52, followed by gradual immune reconstitution. During reconstitution, autoimmune thyroid disease can develop in 30 to 40% of patients.15 Median onset of thyroid dysfunction is about 18 months after treatment, with most presenting within the first three years.16
Graves’ disease and associated TSH-receptor antibody positive hyperthyroidism is the most common manifestation, representing two-thirds of alemtuzumab-associated thyroid dysfunction.16 However, up to 15% of Graves’ cases can have coexisting blocking antibodies, and Graves’ disease in this context may present with a fluctuating course of rapid transition between periods of hyperthyroidism and hypothyroidism.16 Endocrinology input is recommended for patients with hyperthyroidism, as coexistence of blocking and stimulating antibodies may require a ‘block and replace’ treatment strategy using both thyroxine and antithyroid medication.16
A smaller proportion of patients will develop Hashimoto’s thyroiditis with hypothyroidism and positive thyroid peroxidase antibodies.16 Following treatment with alemtuzumab, thyroid function (TSH, FT4, FT3 levels) should be monitored every three months for the first four years.17 After this period, testing is required only for patients with signs or symptoms suggestive of thyroid dysfunction.
Biotin
Biotin is a water-soluble vitamin widely available in nutritional hair and nail supplements. It can also be found in some treatments for inherited mitochondrial disorders and multiple sclerosis. The amount of biotin varies considerably in over-the-counter preparations and can be as high as 10 mg per tablet.18 In a recent study, 29% of adults reported using biotin-containing supplements, with most being in the form of over-the-counter multivitamin preparations.19
Biotin interferes with biotinylated laboratory reagents used in TSH, FT4, FT3 and TSH receptor antibody assays.20 The direction and degree of interference depend on the type of assay used, but low TSH levels with elevated FT4 and FT3 levels mimicking hyperthyroidism occurs most commonly.2 TSH-receptor antibody levels may also be elevated due to biotin use, artefactually suggesting Graves’ disease. Interference is typically seen with high doses but can occur with doses as low as 10 mg per day.21 GPs should be suspicious of biotin use in patients with abnormal thyroid levels who do not have clinical manifestations of thyroid disease. Retesting 48 hours after stopping biotin-containing supplements or contacting the pathology laboratory to request testing for biotin interference is recommended.22
Conclusion
The thyroid plays a pivotal role in the regulation of whole-body metabolism and energy expenditure. Medications can impact on thyroid function through multiple mechanisms resulting in a spectrum of thyroid dysfunction. Awareness by GPs of the effects of these commonly used medications will enhance monitoring, diagnosis and treatment of drug-related thyroid disorders. In addition, understanding how drug interactions, such as biotin, can produce spurious laboratory thyroid function results will reduce unnecessary imaging and treatment of patients without organic thyroid disorders. ET