Testosterone treatment for hypogonadal men: clinical update

Testicular disorders
Men's health
Men with androgen deficiency require careful assessment of symptoms and signs as well as investigation to confirm the diagnosis and identify the underlying causes. Testosterone therapy will benefit men who are hypogonadal because of pituitary or testicular disease.
- Men with androgen deficiency can present with a broad range of symptoms including lethargy, decreased energy, low mood, low libido, osteopenia, reduced muscle mass and increased fat mass.
- Careful clinical assessment is required, including assessment of testicular volumes.
- Confirmatory biochemical testing is via early morning, fasting serum testosterone levels measured using an accurate assay, with sex hormone-binding globulin, luteinising hormone and follicle stimulating hormone levels providing additional information.
- Testosterone therapy is available on the PBS for men with androgen deficiency due to an established pituitary or testicular disorder.
- The patient’s desire for fertility and their cardiovascular and prostate risks should be assessed before commencing testosterone therapy.
Androgen deficiency causes substantial morbidity in affected men. Recognising men who are androgen deficient and identifying the underlying causes are essential prerequisites to commencing testosterone therapy, which requires pretreatment assessment and ongoing monitoring for efficacy and safety.
How do men with androgen deficiency present?
Presenting symptoms of androgen deficiency in men include:
- lethargy
- fatigue
- decreased energy
- low mood
- irritability
- poor concentration
- osteopenia or osteoporosis
- reduced muscle mass
- increased fat mass
- appearance of breast tissue (gynaecomastia)
- decreased libido.1
By contrast, erectile dysfunction tends to have multifactorial origins and is a marker of increased cardiovascular risk, but is uncommon as a presenting feature of androgen deficiency, and then only at very low testosterone concentrations.1 Many men have symptoms such as decreased energy, low mood and poor concentration for reasons unrelated to gonadal dysfunction, yet conversely it is important not to miss the diagnosis of hypogonadism in a man presenting with nonspecific symptoms.
Common causes of hypogonadism in men
Abnormalities of the testes causing primary testicular failure are more common than abnormalities of the hypothalamus or pituitary gland causing secondary testicular failure.1 Testicular diseases, such as Klinefelter’s syndrome, or testicular trauma, torsion, infection, atrophy or removal result in impairment of spermatogenesis and low testosterone concentrations with elevated levels of luteinising hormone (LH) and follicle stimulating hormone (FSH). If fertility is impaired, assisted reproduction may be required, or donor sperm if this is unsuccessful.
Hypothalamic disorders, such as Kallmann syndrome, or pituitary disorders, such as tumours, surgery or radiotherapy, result in impaired spermatogenesis, low testosterone concentrations and low or normal LH and FSH levels (hypogonadotrophic hypogonadism). In this setting, fertility can be restored with gonadotrophin therapy.1 Management of androgen deficiency usually entails testosterone therapy, with certain exceptions. Prolactinoma causes hypogonadotrophic hypogonadism: this is responsive to cabergoline which restores endogenous testosterone production. Iron overload due to untreated hereditary haemochromatosis can result in iron deposition within the pituitary gland and hypogonadotrophic hypogonadism; with this presentation, preventing or reversing iron overload is the first approach.
Evaluation
Enquire about pubertal development, prior fertility, any history of testicular conditions, medications, alcohol intake, smoking and recreational drug or androgen use, in addition to any systemic diseases or other medical comorbidities. The physical examination offers an opportunity to assess for muscle, fat and body hair distributions and the presence of gynaecomastia.
Test for visual field defects and perform a scrotal examination including assessing testicular volumes using an orchidometer.1 Klinefelter’s syndrome can be detected by scrotal examination, with the presentation of characteristically small testes.
Investigations
Biochemical testing is best performed early in the morning (fasting if possible). Serum testosterone level should be measured using an accurate assay: ideally mass spectrometry where available, if not, then immunoassay in a laboratory with established quality controls to ensure accuracy of the results.1 If this level is normal, androgen deficiency is unlikely. If it is low, the result must be confirmed with a second blood sampling. Reference ranges for testosterone are: 10.4 to 30.1 nmol/L in reproductively normal men between 21 and 35 years of age, and 6.4 to 25.7nmol/L in healthy men between 70 and 89 years of age.2,3 For men from 35 to 70 years of age, the lower cut-off for testosterone can be interpolated and would correspond to 8 nmol/L.4
Measurement of sex hormone-binding globulin (SHBG) is also useful to test whether a testosterone result is low due to low SHBG (seen in obesity, insulin resistance or following exposure to exogenous androgens). Elevated LH and FSH levels point to a primary testicular disorder. If LH and FSH levels are low or normal and hypogonadotrophic hypogonadism suspected, prolactin level, iron studies and MRI of the pituitary could be considered for further investigation. Where pituitary disease is suspected, assessment of other anterior pituitary function (early morning cortisol, free thyroxine, insulin-like growth factor-1 levels) may be helpful.
Pathological hypogonadism
Australian and US endocrine societies emphasise the importance of identifying the underlying cause of androgen deficiency.1,5 Testosterone treatment is warranted in men with androgen deficiency due to pathological hypogonadism caused by disease of the hypothalamus, pituitary or testes.1 This concurs with the PBS providing subsidised treatment for androgen deficiency in a patient with an established pituitary or testicular disorder. However, men can have low testosterone concentrations with low or normal LH and FSH levels in a range of conditions where the function of the hypothalamo-pituitary-testicular (HPT) axis is inhibited, especially in the setting of obesity, systemic illness or depression, or with the use of opioids and corticosteroids.1 Here, the optimal approach is to address the underlying condition and to minimise the use of interfering medications to allow the HPT axis function to recover.
Older men with disorders of the hypothalamus, pituitary or testes may benefit from testosterone therapy; age in itself is not a contraindication to treatment. However, testosterone treatment is not recommended for older men, who may have chronic disease and lower testosterone concentrations, in the absence of pathological hypogonadism.1 The PBS specifically excludes subsidisation of testosterone therapy for men who are more than 40 years of age with low testosterone concentrations who do not have an established pituitary or testicular disorder, and in whom a low testosterone level is due to age, obesity, cardiovascular disease or drugs. The US Endocrine Society guidelines also emphasise the importance of distinguishing ‘organic’ from ‘functional’ (and potentially reversible) causes.5
Treatment
Testosterone is the native hormone and the replacement therapy of choice to reverse the symptoms and signs of androgen deficiency. PBS-listed options include long-acting depot intramuscular testosterone undecanoate given at three-monthly intervals, or daily transdermal testosterone gel or testosterone cream formulations.6 In men with bleeding disorders or on anticoagulants, deep intramuscular injections carry some risk of haematoma formation. Transdermal gel or cream requires precautions against inadvertent transfer to others from skin contact.6 Men may express a personal preference for one or other route of administration. Oral testosterone undecanoate capsules are not preferred, as absorption is limited necessitating frequent dosing.
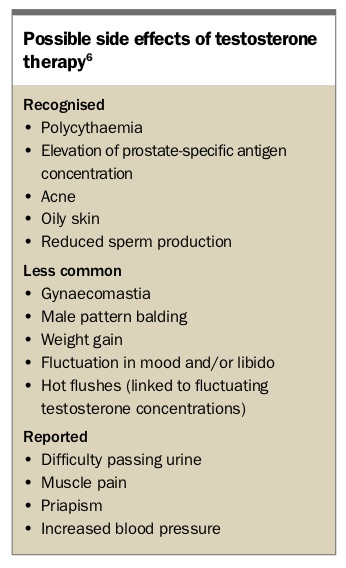
Testosterone patches have fallen out of favour due to skin irritation: this is much less of an issue with gel and cream formulations, which are usually well tolerated. Short-acting testosterone intramuscular injections given every two weeks tend to result in marked peaks and troughs in circulating testosterone concentrations and are no longer PBS listed. Men should be counselled regarding possible side effects of testosterone therapy (Box).
{kind=link}
Precautions and monitoring
Exogenous testosterone will inhibit spermatogenesis to reduce fertility, therefore if fertility is desired this should be addressed before starting testosterone therapy. Testosterone therapy is contraindicated in men with prostate or breast cancer. Precautions requiring evaluation and management before consideration of testosterone therapy are undiagnosed prostate abnormalities with or without elevated prostate-specific antigen (PSA), severe lower urinary tract symptoms, untreated polycythaemia, untreated severe sleep apnoea and unstable or inadequately treated cardiac disease.1,5 Although testosterone is unlikely to cause prostate problems, it may unmask underlying prostate conditions.6 Men in whom there is a substantive risk of pre-existing or underlying prostate disease, including cancer, should be counselled regarding screening with digital rectal examination of the prostate and PSA testing.5,6
There is uncertainty over whether testosterone therapy has beneficial, neutral or adverse effects on the cardiovascular system.5,7 Men with cardiovascular disease (or symptoms suggestive of this) should have their cardiovascular therapy optimised before consideration of testosterone therapy.6 The US Endocrine Society recommends against testosterone therapy in men with uncontrolled heart failure, myocardial infarction or stroke within the past six months, and in men with thrombophilia.5
Efficacy is monitored by the resolution of symptoms of androgen deficiency. Improved body composition and bone mineral density may be expected. It can be helpful to check trough testosterone concentrations (before the next dose after a period of treatment), which should be in the lower part of the reference range for eugonadal men.6 Safety monitoring should include monitoring for any adverse effects of therapy and PSA screening. Full blood count for assessment of haemoglobin and haematocrit should be performed after three months of treatment and annually thereafter.6
Referral to specialist and shared care
There are reasons to refer a patient to a specialist. First, the PBS criteria require treatment with a specialist such as an endocrinologist or an appointment for assessment by one. Second, a patient should be referred if the indication for testosterone treatment is unclear. High-quality evidence is lacking to justify testosterone supplementation for men with low testosterone concentrations in the setting of obesity, systemic disease or medical comorbidities, or medications including opioids and corticosteroids. The results of the Australia-wide randomised controlled trial Testosterone Intervention for the Prevention of Diabetes Mellitus in High-risk Men (T4DM) will be available in 2019 and may prompt reconsideration of existing guidelines. Until then, addressing the underlying issues in a holistic fashion is the preferred strategy.8 There is scope for individualised approaches, for example in men receiving opioids or corticosteroids for medical indications at the lowest necessary doses who have symptoms in the context of very low testosterone concentrations. Assessment by an endocrinologist may be useful for these complex patients.
Referral may also be useful for re-evaluation and optimisation of treatment options in men who are not achieving satisfactory improvement or who have side effects on treatment. Shared care is important to optimise supervision and monitoring of therapy. In men with pathological hypogonadism who have been stabilised on testosterone therapy with good results, GPs are in a primary position to provide long-term follow up.
Conclusion
Men with androgen deficiency require careful assessment of symptoms and signs as well as investigation to confirm the diagnosis and identify the underlying causes. Testosterone is the treatment of choice to reverse the symptoms and signs, and men should be counselled regarding the possible side effects of therapy. Ongoing monitoring for efficacy and safety is essential. ET
References
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.