Bariatric surgery: the GP’s role in patient selection and management

Obesity
GPs have a crucial role in selecting patients for consideration of bariatric surgery and providing long-term follow up and support after surgery. Practical tips are provided on selecting patients, managing them immediately after surgery, recognising complications, long-term monitoring and preventing nutritional deficiencies.
- Over 20,000 bariatric surgical procedures are performed annually in Australia.
- GPs have a key role in selecting patients for consideration of bariatric surgery and, after initial postsurgical management, most patients are discharged into the care of their GP.
- In addition to complications associated with all surgery, immediate postoperative complications can include dehydration, hypotension and hypoglycaemia.
- Eating disorders and mental health problems are common in people presenting for bariatric surgery; identification and stabilisation of these disorders are needed before surgery, and patients need ongoing support after surgery.
- Long term follow up is important to identify, treat and prevent nutritional, metabolic, mechanical and psychosocial complications of bariatric surgery; patients invariably require lifelong multivitamin and micronutrient supplementation.
Bariatric surgery, also termed metabolic surgery, results in greater and more durable weight loss than existing medical or lifestyle interventions and has metabolic and mechanical benefits. It is safe, with a reported mortality of less than 0.1% according to the Australian Bariatric Surgery Registry.1 The number of bariatric surgical procedures performed annually in Australia doubled between 2005 and 2014, highlighting the demand for weight management options.2 The Australian Bariatric Surgery Registry reported over 27,857 surgeries performed in 2018-19 alone.3,4
Patients with a body mass index (BMI) over 35 kg/m2 and a significant weight-related disorder or a BMI over 40 kg/m2 qualify for bariatric surgery if they have exhausted all other nonsurgical treatments.5 Bariatric surgery encompasses an expanding list of procedures. Laparoscopic sleeve gastrectomy is the most popular, accounting for around three-quarters of primary procedures in Australia. Other procedures include Roux-en-Y gastric bypass, one anastomosis gastric bypass (or minibypass) and laparoscopic adjustable gastric band surgery.
Over 90% of bariatric procedures are performed in private hospitals, and after immediate postoperative management, most patients are followed up in primary care. Bariatric surgery performed in public hospitals has been shown to be as effective as that performed in private hospitals despite a more medically and psychosocially complex patient population.6 This complex subpopulation is mostly followed up in specialist obesity clinics within the public system, managed in concert with their GPs and eventually discharged to primary care.
GPs have a key role in referring patients for consideration of bariatric surgery and in their long-term management after surgery. This article provides practical tips on how to select the appropriate patients for bariatric surgery and how to recognise complications, as well as recommended monitoring and long-term care.
Patient selection and referral
Management of patients who wish to have bariatric surgery should importantly start before referral to a surgeon. Patient selection should include consideration of the likelihood of a good weight loss outcome, potential mechanical and metabolic recovery and safety. Patients should be able to adhere to the recommended postoperative management plan in the opinion of their GP.
About 20% of patients who undergo bariatric surgery do not have adequate weight loss (defined as more than 15% of total body weight after two years). Although it is difficult to predict long-term success, our experience is that patients who consume excess energy predominantly to alleviate psychological distress are less likely to have a successful outcome. The patient’s regular GP may be in the best position to assess this. If psychological distress is suspected, we recommend the patient be screened by a clinical psychologist to help with assessment and stabilisation before referral to a bariatric surgeon.
Screening of new patients at a public metabolic program in Sydney with a standard questionnaire suggested that 84% of patients had a moderate, high or very high risk of psychological distress, and over half were at risk of having an eating disorder.7 This population has a high rate of undiagnosed and untreated mental health disorders, with a study in Western Australia identifying new psychiatric illness in 6.9% of their postsurgical patients.8
Contraindications to bariatric surgery include severe or untreated mental health disorder, concomitant drug abuse, smoking and general contraindications to anaesthesia. Although patients with type 2 diabetes benefit significantly from weight loss and bariatric surgery, those with type 1 diabetes and obesity should be reviewed by an endocrinologist before consideration of bariatric surgery.
The patient’s expectations of bariatric surgery are crucial for longer-term success. Average long-term weight loss after surgery is about 20%.1,9 Data suggest that as many as half of patients would be disappointed if they did not lose more than 20% of their body weight; in our experience, most patients would prefer to lose 40% or more of their total body weight. Patients often misunderstand the term used by surgeons: percentage excess weight loss (%EWL). Percentage EWL is defined as the difference between the initial and final BMI divided by the difference between the initial and ‘normal’ BMI (typically 25 kg/m2). Patients may incorrectly believe this to be the percentage of total weight lost. Percentage EWL can also give the appearance of better weight loss in patients with a smaller amount of initial excess weight.
We recommend referring patients to surgeons who specialise in bariatric surgery and also participate in the Australian Bariatric Surgery Registry. This registry monitors not only weight outcomes but also complications.
Early postoperative management: zero to six weeks
The treating bariatric team, which should include a specialist dietitian, will need to provide close support for the patient in the first six weeks after surgery. Postoperatively, patients are discharged from hospital on a liquid diet, with advice to consume more than 1 L volume daily and to avoid carbonated drinks. We generally recommend patients test thicker liquids such as yoghurt and milk after 48 hours. Two weeks after surgery, they can transition onto pureed foods if they have tolerated thickened fluids in the preceding week without dysphagia or vomiting. Patients should aim to eat slowly after surgery, which will help them recognise early satiety signals and stop eating before they feel full.
Adequate protein intake is crucial at this time to avoid excess muscle catabolism, as protein deficiency remains the most common and severe macronutrient deficiency after bariatric surgery.10 We recommend 1.5 to 2.0 g of protein per kilogram of ideal body weight per day. Intake can be supplemented with commercially available protein water if needed. We also recommend that patients immediately start taking a multivitamin that matches the required daily intake (RDI) of most micronutrients. Not all commercially available multivitamins meet the requirements of patients who have undergone bariatric surgery. Prophylactic replacement of vitamin D and calcium is also recommended. The bariatric dietitian should be able to recommend an appropriate multivitamin.
Patients may also be recommended to continue taking thromboprophylaxis for two weeks (usually 20 mg enoxaparin daily), depending on their risk factor profile. Venous thromboembolic events were historically responsible for a large proportion of the preventable morbidity and mortality after bariatric surgery.11,12
Potential metabolic complications after bariatric surgery are listed in Table 1.13 For patients taking antihypertensive medication, we recommend routine blood pressure measurements every one to two weeks, as hypotension is a common consequence of rapid weight loss. Antihypertensive medications may need to be reduced or stopped. Patients needing glucose-lowering medications immediately after surgery should monitor their blood glucose levels daily and have their medications titrated as necessary. For people with diabetes and evidence of retinopathy, repeat retinal screening is advised before surgery. This is particularly important in patients with poor glycaemic control before bariatric surgery, as sudden large improvements in glycaemic control have been shown to worsen diabetic retinopathy.
{kind=link}
We also recommend that patients be counselled to avoid or be judicious in their alcohol consumption as the first-pass gastric metabolism of alcohol is lost. This increases the risk of intoxication at minimal to modest levels of alcohol consumption. Further, the rapidly rising blood alcohol level may exceed the legal limit to drive after only one or two standard drinks.
Postoperative complications
Patients need monitoring for both complications and general changes to their health status as they continue to lose weight. These changes can be broadly divided into mechanical, metabolic and psychological.
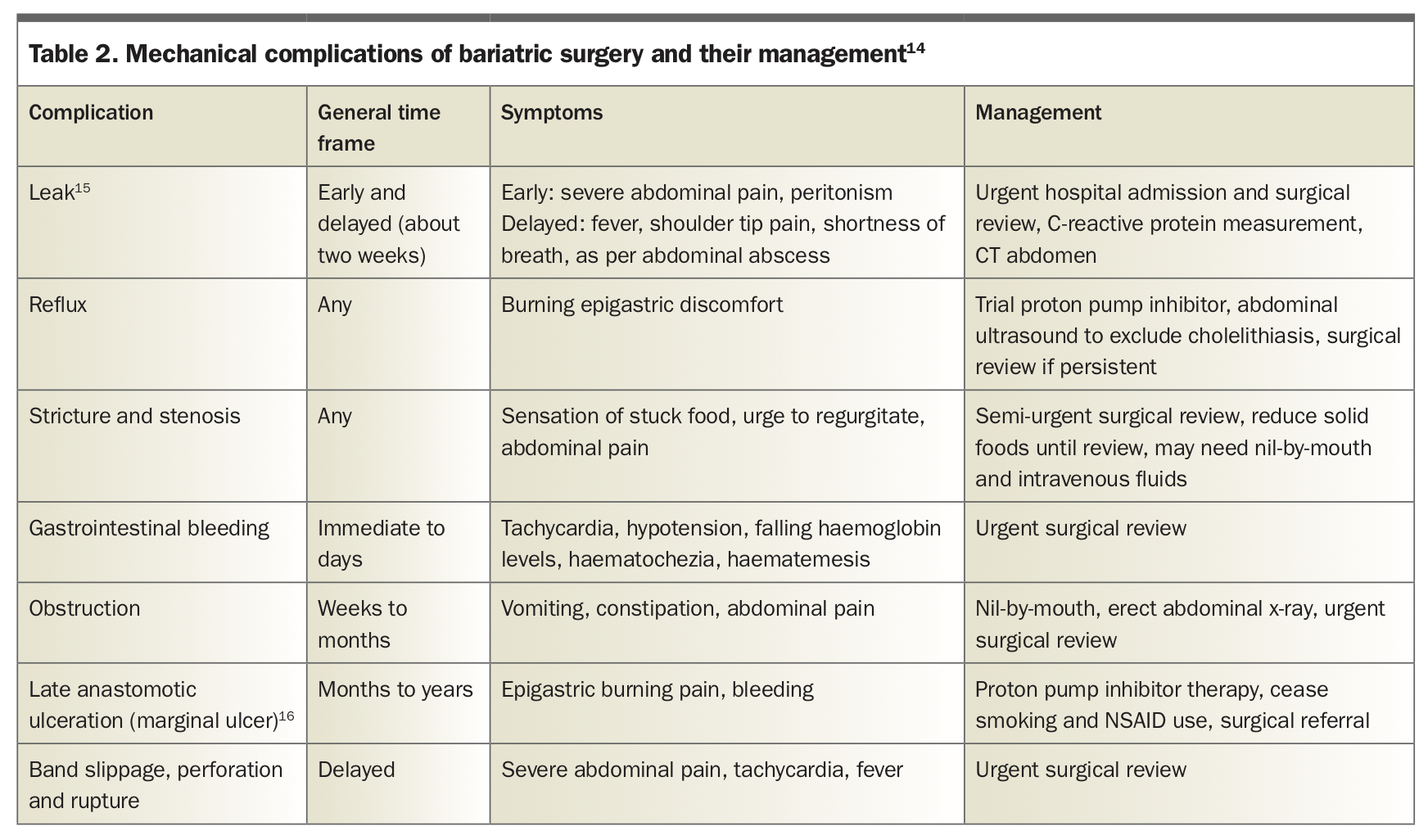
Potential mechanical complications of bariatric surgery are listed in Table 2.14-16 Red flags to be aware of include tachycardia, abdominal pain, systemic signs of inflammation or infection and intractable vomiting. Patients presenting with intractable vomiting should be given parenteral vitamin B1 (thiamine) before they are given glucose to prevent the development of Wernicke’s encephalopathy. Worsening gastroesophageal reflux after sleeve gastrectomy despite significant weight loss is not uncommon and necessitates review by the surgeon if unresponsive to proton pump inhibitor therapy.
{kind=link}
Late-stage complications
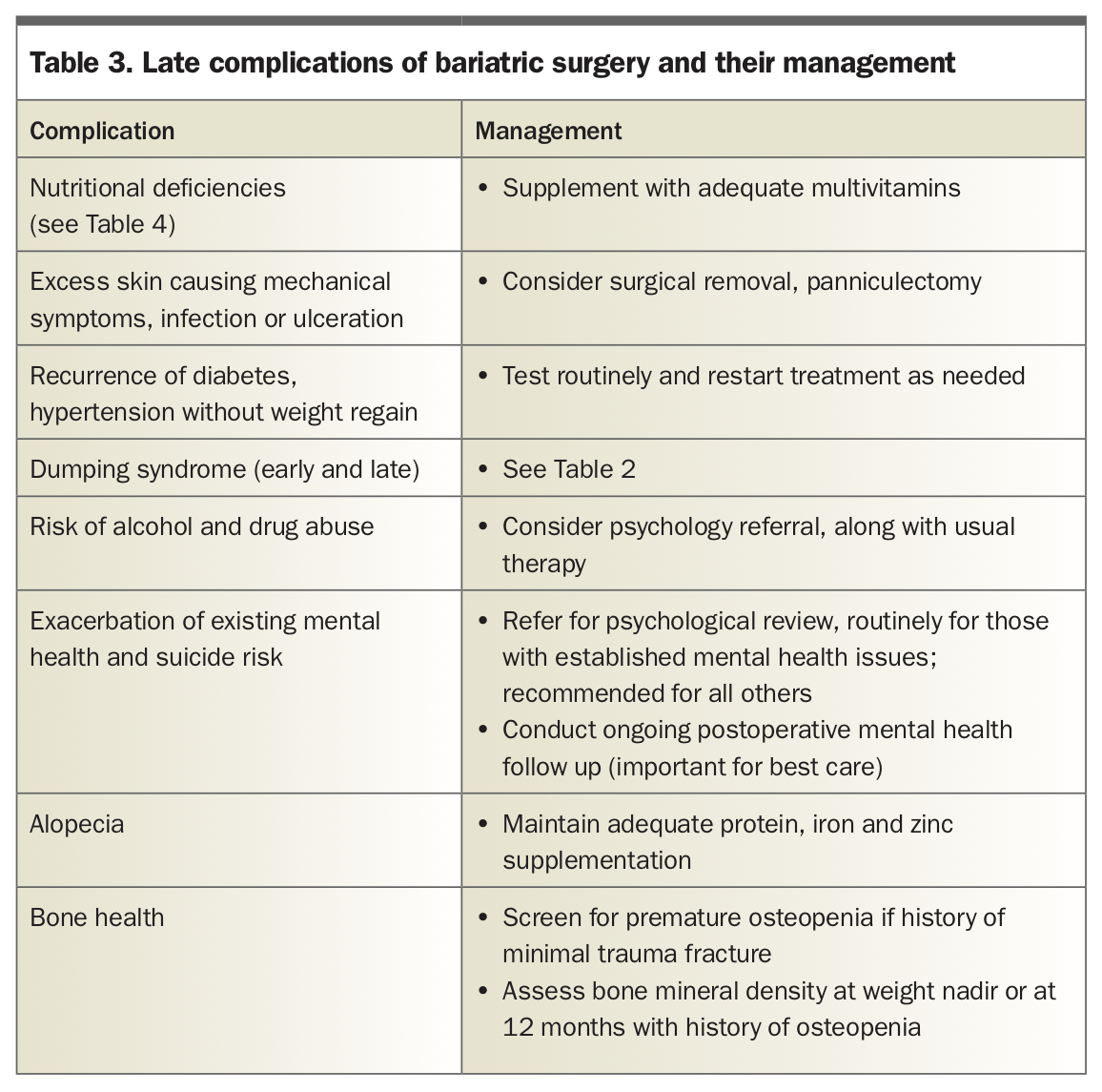
Common late complications after bariatric surgery are listed in Table 3. Patients require monitoring for the recurrence of metabolic diseases such as type 2 diabetes and hypertension, even without weight gain.
{kind=link}
Dumping syndrome is a complication mostly associated with Roux-en-Y gastric bypass but can also occur after laparoscopic sleeve gastrectomy and one anastomosis gastric bypass.17-20 Dumping syndrome is classified as the early variant if it occurs within the early postoperative period and late variant if it occurs a year or longer after surgery.
The classification of early versus late dumping syndrome is also separately applied to the timing of symptoms in relation to food. In the early timing form, symptoms occur within one hour of a meal, and in the late timing form, they occur two to three hours after a meal.21 Both forms are described in Table 1. Dietary advice may help improve symptoms. If symptoms persist, referral to a specialist with experience in managing this condition is recommended.
Patients are also at risk of exacerbations of existing or unidentified mental health issues, such as depression, other specified feeding or eating disorders and body dysmorphic disorder. A further risk is addiction transfer, such as alcohol and drug misuse. Joining a patient support group may help patients identify with others struggling with similar postoperative issues and build support networks that will reduce their risk.
Nutritional deficiencies
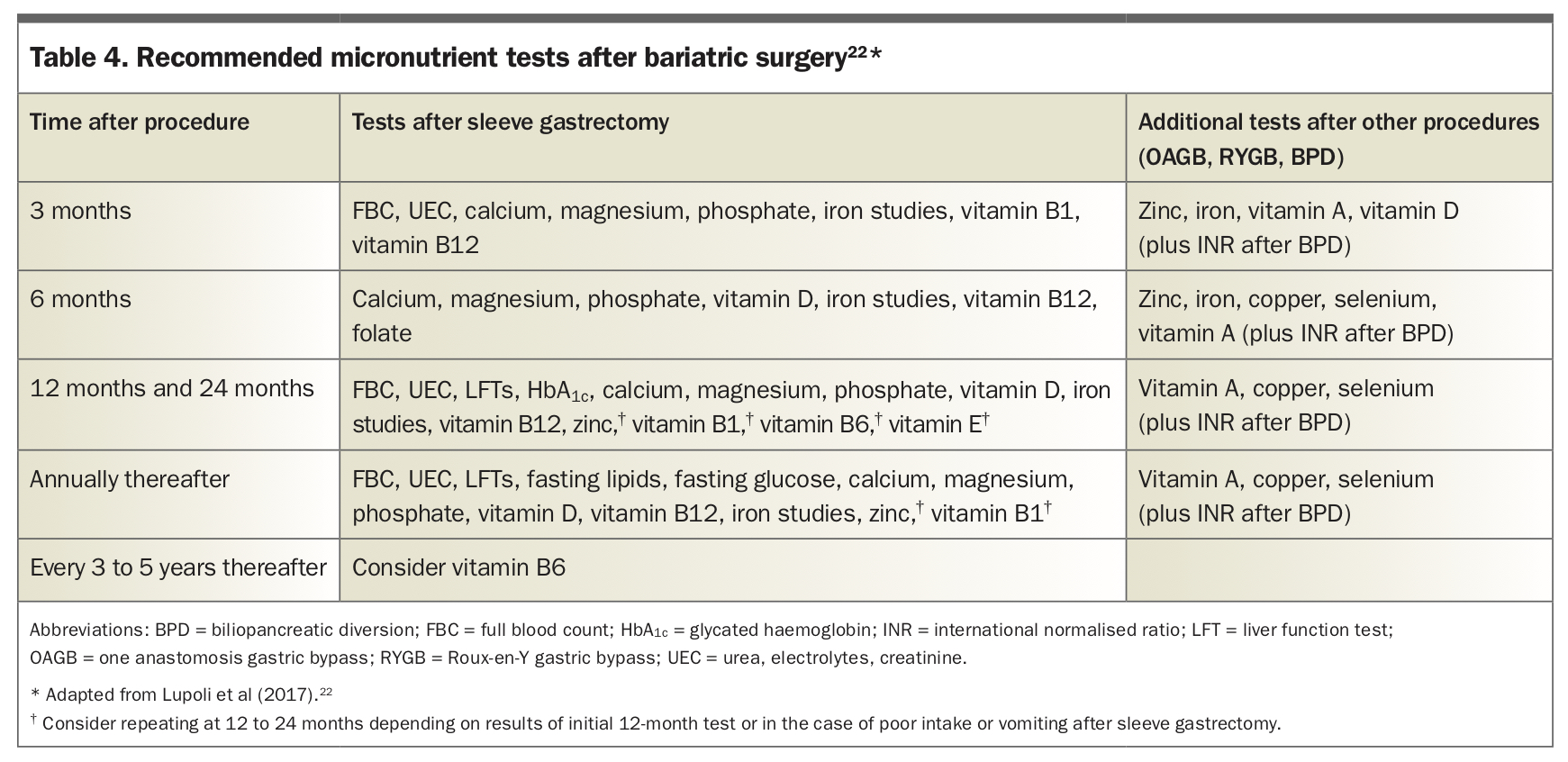
Bariatric surgery is associated with micronutrient deficiencies if the patient does not receive prophylaxis with a suitable multivitamin. In general, we recommend assessing patients for micronutrient deficiencies and correcting these preoperatively. The evidence for micronutrient testing and routine supplementation remains an area of active research. The testing we consider potentially useful and perform routinely for patients after bariatric surgery is summarised in Table 4.22 This includes routine examination and blood tests every six to 12 months and a bone mineral density study at 12 months for early identification of emerging osteoporosis.
{kind=link}
Signs of vitamin B1 (thiamine) deficiency include irritability and difficulties with short-term memory.23 Longer-term signs and symptoms include vertigo, double vision, heart failure and neuropathy. Signs of vitamin A deficiency include corneal xerosis and keratomalacia. More severe signs include opportunistic infections and visual loss. Signs and symptoms of vitamin B6 (pyridoxine) deficiency include stomatitis, seborrhoeic dermatitis, peripheral neuropathy, skin sensitivity and movement disorders or seizures.24 Vitamin B12 (cobalamin) deficiency rarely occurs in isolation and is conversely more likely to be overcorrected with appropriate supplementation.25 Vitamin D levels can be reduced after bariatric surgery. We recommend assessing vitamin D levels, as well as bone mineral density after the patient’s weight reaches a nadir or at 12 months if they have an established history of osteopenia.26
Pregnancy
Given the ongoing weight loss and risk of nutritional deficiency, we recommend that women should use reliable contraception for at least 12 months after bariatric surgery before planning their next pregnancy. This recommendation is consistent with the general consensus of guidelines from the Endocrine Society, American Association of Clinical Endocrinologists, American Society for Metabolic and Bariatric Surgery and others, although data are sparse.27-29 Similarly, long-term pregnancy outcomes after bariatric surgery are unknown, although evidence suggests a reduction in risk of gestational diabetes, pregnancy induced-hypertension and large-for-gestational age infants, but a concomitant increase in small- for-gestational age infants.30-32
Management of suboptimal long-term weight loss or weight regain
Most patients will have significant weight loss in the first 24 months after bariatric surgery. For patients who do not have adequate initial weight loss (less than 15% of total body weight), referral to a specialist medical obesity service is recommended before consideration of revisional surgery, such as conversion of sleeve gastrectomy to a gastric bypass. If eating to alleviate psychological distress is identified then referral to a clinical psychologist or psychiatrist with experience in treating bariatric surgery patients is recommended. If not a significant factor then obesity pharmacotherapy may be considered.
Up to 20% of patients experience significant weight regain (even up to presurgical weight) after two years. Our experience is that the vast majority of these patients have excess energy consumption to alleviate psychological distress rather than a complication of the surgical procedure. If this is not dealt with before revisional surgery then weight loss outcomes are likely to be less than expected.
Conclusion
Bariatric surgery is an effective and safe procedure when performed by a surgeon who specialises in this surgery in a patient who has been appropriately selected and screened. Patients should be medically and psychologically prepared and considered able to adhere to the recommended postoperative management plan. Bariatric surgery usually leads to significant weight loss and subsequent improved health outcomes. However, long-term follow up and support is needed for optimal and durable outcomes. The GP has an integral role in identifying patients who may benefit from bariatric surgery and providing long-term follow up and support. ET