Paget’s disease of bone: who to treat and why it matters

Paget's Disease of Bone
Bone diseases
Although the prevalence of Paget’s disease is declining, it remains an important clinical entity. In people with symptomatic Paget’s disease who are left untreated, there is potential for significant disease-specific morbidity. There are highly successful treatments available for this benign bone disorder, with bisphosphonates the mainstay of treatment.
- Paget’s disease is a benign bone disorder that is characterised by osteoclast activation with increased bone turnover and disorganised bone architecture.
- It is typically asymptomatic, but in some cases it may result in bone pain, deformity, pathological fracture or hearing loss.
- In asymptomatic patients, treatment is not required unless the site of disease increases the risk of future complications.
- Bisphosphonates are highly effective in suppressing bone turnover and are the mainstay of treatment. Zoledronic acid 5 mg given as a single intravenous dose is the preferred drug and usually results in sustained remission and improvement in bone pain.
Picture credit: © SPL
Paget’s disease of bone was first described as a unique clinical entity in 1877, with Sir James Paget reporting on a case of osteitis deformans thought to be related to an underlying inflammatory condition. It is now recognised that Paget’s disease is a benign bone disorder resulting from uncoupling of bone turnover and disorganised bone remodelling. In the initial (osteolytic) phase of disease, there is focally increased osteoclastic activity with consequent bone loss due to excessive bone resorption. Bone resorption is continuous, and on average an untreated resorption front progresses by 7 to 10 mm/year.1 Following the osteolytic phase, osteoblast activity increases in an attempt to fill the resorption clefts through production of new bone. The newly formed bone is structurally disorganised (woven bone) and produced in a nonuniform manner resulting in areas of bony expansion and deformity interspersed with areas of brittle bone susceptible to fracture.1
Paget’s disease is rare in people under the age of 50 years, but increases in prevalence thereafter, in some counties affecting 2 to 7% of people over the age of 80 years.2 Paget’s disease most commonly affects Caucasian people of European descent, and is rare in Asians, Africans and people from the Indian subcontinent.3 There is a slight male preponderance (see Box 1 listing the risk factors). Although there are no recent prevalence studies of this disorder in Australia, a decline in prevalence has been observed across Europe in both men and women.4 The reason for this decrease is unclear, but may be related to environmental factors with the largest decreases observed in the areas with the highest prevalence.
{kind=link}
Pathogenesis
The aetiology of Paget’s disease has not been fully elucidated, but genetic factors are important with first-degree relatives of patients with Paget’s disease having a seven to 10 times increased risk.4 The genetic inheritance pattern is autosomal dominant, but with incomplete penetrance, whereby only a subset of genetically affected individuals will go on to develop Paget’s disease. The SQSTM1 gene is particularly important and regulates the p62 protein that is involved in osteoclast signalling.5 Mutation of the SQSTM1 gene is found in 46% of patients with familial Paget’s disease and 16% of sporadic cases.5 There is some weak evidence linking Paget’s disease with viral infections (measles or canine distemper virus).1
Clinical features
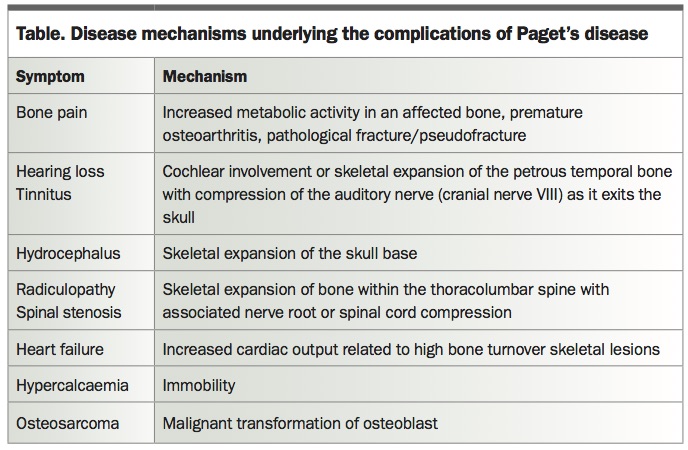
A single bone (monostotic) or multiple bones (polyostotic) may be affected in people with Paget’s disease, with the most commonly affected sites including the pelvis, femur, lumbar spine, skull and tibia. Up to two-thirds of cases are asymptomatic and are found incidentally on radiographic examination or biochemical testing. If symptomatic, bone pain is the most frequently reported symptom and is typically a dull ache that is present at rest and at night. In severe cases there may be accompanying erythema, swelling and heat over the affected bony site due to increased blood flow. Bone deformity occurs only in longstanding disease. Paget’s disease of bone is associated with pathological fractures and can result in accelerated osteoarthritis if it occurs adjacent to joints. New bone formation can result in compressive neuropathies such as radiculopathy, spinal canal stenosis with cord compression or deafness in cranial Paget’s disease. Hypercalcaemia, high output cardiac failure and osteosarcoma are very rare complications. Primary hyperparathyroidism is more common in patients with Paget’s disease.
Diagnosis
The diagnosis of Paget’s disease is usually straightforward and in most cases is made after detecting an isolated elevation in serum alkaline phosphatase (ALP) levels or finding typical Pagetic changes on a radiograph.6 The typical features include focal osteolysis with coarsening of the trabecular pattern, bone expansion, and cortical bone thickening (Figure 1).
{kind=link}
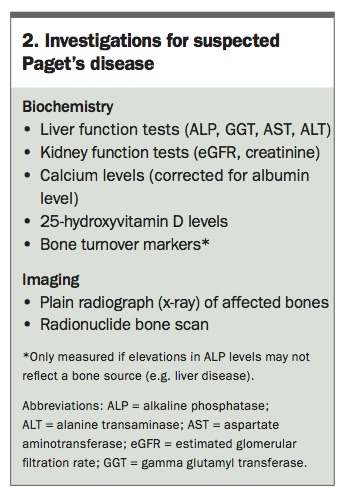
Once the diagnosis is suspected, serum calcium and 25-hydroxyvitamin D levels should be measured with an aim to maintain vitamin D above 50 nmol/L. If the serum calcium level is elevated, this should be further investigated as appropriate. Measurement of the bone turnover markers procollagen 1 N-terminal polypeptide, bone specific ALP (ostase) and urine N-terminal telopeptide (expressed as a ratio of NTx:creatinine) may be helpful if the serum ALP level is elevated in the setting of coexisting liver disease, whereby ALP elevations are not clearly related to an increase in bone turnover. Typically, turnover markers will be elevated in people with polyostotic disease, but may be normal in those with monostotic Paget’s disease, indicating a lesser disease burden. It is important to remember that bone turnover markers should be performed fasting, and may be elevated if measured in the nonfasting state. Markers may also be spuriously elevated in the setting of renal impairment, and serum creatinine levels should also be measured as part of the biochemical workup in people with Paget’s disease (Box 2).
{kind=link}
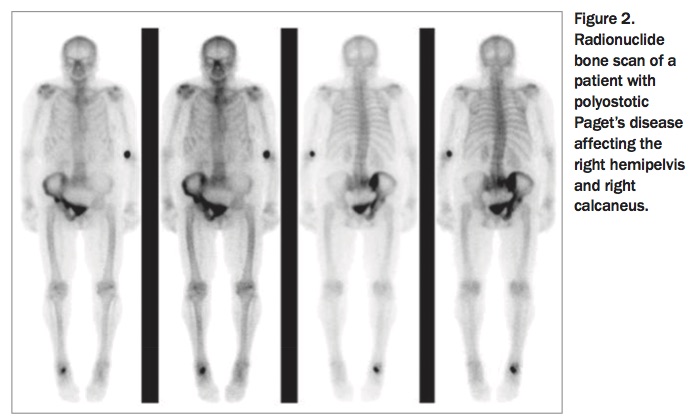
In addition to a plain film x-ray of the affected bone, a radionuclide bone scan is useful in establishing the extent of the disease (Figure 2).6 Additional imaging with CT or MRI is generally unnecessary except when investigating potential complications. The number of bones affected by Paget’s disease remains constant throughout a patient’s lifetime.
{kind=link}
How to treat
Bisphosphonates are highly effective in suppressing bone turnover and are the mainstay of treatment for Paget’s disease. However, before treatment, all patients should have their serum calcium levels checked and be made vitamin D replete (>50 nmol/L) to prevent hypocalcaemia. Risedronate, pamidronate and zoledronic acid are listed on the Pharmaceutical Benefits Scheme for symptomatic Paget’s disease of bone. However, following a landmark study showing superiority of intravenous zoledronic acid in normalising ALP levels compared with oral risedronate (89% vs 58% of patients, respectively),7 zoledronic acid given as a single 5 mg intravenous infusion is the preferred treatment and will usually result in a sustained remission without need for further treatment, depending on disease severity.3 Additionally, zoledronic acid does not have the gastrointestinal side effects that may be experienced with oral bisphosphonates. In our experience, 20 to 30% of patients will experience a flu-like illness following the infusion, which is generally short lived and unlikely to recur if further infusions are required. The maximal suppressive effect of bisphosphonates on ALP will occur after six months, but levels generally begin to decline within 10 days of treatment.3 There is limited evidence to support the use of denosumab for the treatment of Paget’s disease, and it is not approved by the Therapeutic Goods Administration or listed on the Pharmaceutical Benefits Scheme for this indication.
Following a diagnosis of Paget’s disease, specialist referral of the patient to an endocrinologist is generally recommended if the serum ALP level is elevated or if bone pain is present. Intravenous infusion of zoledronic acid can be performed through most hospital infusion units or via an outpatient infusion service.
Who to treat
The role of bisphosphonates in patients with bone pain has been well established. Therapy should be offered to all patients with bone pain or established complications of Paget’s disease (Table).6 People with asymptomatic Paget’s disease generally do not require treatment; however, if the site of the disease increases the risk of future complications (e.g. vertebral involvement leading to spinal cord compression) then treatment should be considered.6 This decision must be made on a patient-by-patient basis, as randomised controlled trial evidence has not shown treatment of asymptomatic patients to have significant benefit in terms of fractures, hearing loss, joint replacement, future bone pain or quality-of-life measures.3 In patients requiring surgery on Paget’s-affected bone, there is a role for pretreatment with bisphosphonates to reduce operative blood loss.6
{kind=link}
Monitoring
Following treatment, annual measurement of ALP levels is sufficient to monitor most patients, although more frequent monitoring may be indicated if less potent oral bisphosphonates are used. After treatment, an ALP level within the lower normal reference range is consistent with disease control, and indicates ongoing efficacy of past treatment with bisphosphonates.6 In a minority of cases, bone turnover (serum ALP) may escape suppression after five to six years, and in this setting a second 5 mg dose of zoledronic acid is usually sufficient to achieve biochemical control.6 There is no place for serial radionuclide bone scans for monitoring treatment response to bisphosphonates.
Conclusion
Paget’s disease is a benign bone disorder that most commonly affects older Caucasians. It is often asymptomatic, detected incidentally by raised serum ALP levels or on radiographs showing typical Pagetic changes; however, it can also present in a minority of patients as bone pain. Treatment with a single infusion of zoledronic acid 5mg is generally safe, long-lasting and effective in resolving bone pain and normalising bone turnover markers. ET
Further reading and references
A list is included in the online version of this article