Bone health and prostate cancer: when should it be considered and investigated?

Prostate cancer
Bone diseases
Bone health is an important consideration in men with prostate cancer. Androgen deprivation therapy (ADT) accelerates bone loss and consequently increases fracture risk. Patients given ADT should undergo baseline assessment of risk. Antiresorptive therapy is recommended for all men who have had a fracture, and should be considered for primary prevention among men at high risk.
Prostate cancer is the most common solid organ malignancy in men in Australia, with 18,000 new diagnoses in Australia in 2016.1 In the past, the incidence of prostate cancer steadily increased owing to the ageing population and more frequent testing for serum prostate-specific antigen (PSA) levels. However, more recent evidence suggests the incidence of prostate cancer in Australia may no longer be increasing, in part due to uncertainties regarding PSA screening.2
Androgen deprivation therapy (ADT) is used in the management of patients who have locally advanced or metastatic prostate cancer. The duration of ADT varies depending on the stage of prostate cancer; generally, it is from three months to three years in patients receiving adjuvant therapy, and long term in patients who have metastatic cancer. Although intermittent ADT is increasingly used, it is important to note that endogenous testosterone secretion may not fully recover in off-treatment periods. Similarly, after a patient stops a prolonged course of ADT the average time to recovery of endogenous testosterone production is 18 to 24 months, and may be longer in older obese men with multiple comorbidities. Therefore, adverse endocrine effects may persist for some time after ADT cessation.
ADT results in profound sex-steroid deficiency (reducing both circulating testosterone and oestradiol concentrations to near zero), with musculoskeletal, cardiovascular and metabolic complications of the resultant hypogonadism. Bone loss during ADT is predominantly a consequence of the low circulating oestradiol levels. Low testosterone may have direct effects on bone structure, but is considered to increase fracture risk predominantly indirectly, via loss of muscle mass. Sarcopenia promotes loss of bone mass via reduced mechanical load and may alter secretion of muscle-secreted factors (myokines) that regulate bone remodelling.3 Sarcopenia also increases the risk of falls that may lead to fractures.4
ADT accelerates the age-related decline in bone mineral density (BMD), with a five- to 10-fold increase in the rate of bone loss at all skeletal sites.5 Annual rates of bone loss range from 2 to 8%, compared with 0.5 to 1% in men in the general population.6 Bone loss occurs within months of the initiation of ADT, is maximal within the first year and then declines with long-term ADT, highlighting the need for early preventive therapy.5
An Australian prospective study has reported that monitoring using dual-energy x-ray absorptiometry (DXA) underestimates the structural decay of bone architecture occurring during ADT: after the first 12 months of ADT, DXA-measured BMD loss was 3% and cortical bone loss measured by high-resolution peripheral quantitative CT was 12%.7
Reduced BMD and a resultant increased fracture risk have been extensively documented in men receiving ADT, highlighting the need for a structured approach to ensure the maintenance of bone health in these men.8
Bone health in ADT-naïve men
Assessment of bone health should be undertaken in all men at the time of prostate cancer diagnosis. A high baseline prevalence of osteopenia and osteoporosis has been shown in the population with newly diagnosed prostate cancer.
In an Australian cohort of men with prostate cancer, the baseline prevalences of osteopenia and osteoporosis were 40% and 11%, respectively, which was higher than in the age-matched general Australian male population.9 Bone health represents a significant concern in this population even before patients undergo ADT.
Fracture risk with ADT
A number of epidemiological studies have shown an association between ADT and an increased risk of fracture. In a retrospective cohort study of more than 50,000 patients who were followed for five years after a diagnosis of prostate cancer, 19.4% of men undergoing ADT had a fracture compared with 12.6% of men who did not receive ADT.8 ADT has been associated with a 30% increased relative risk of fracture over five years, with 30 being the estimated number needed to harm for the occurrence of one fracture.10
Baseline assessment
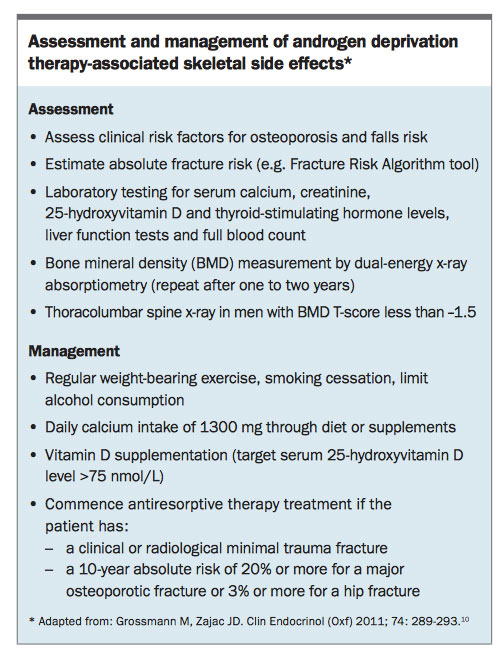
Baseline assessment of bone health should be undertaken in all men with newly diagnosed prostate cancer. This should incorporate an assessment of their clinical risk factors for osteoporosis, in particular a previous history of minimal trauma fracture. Other secondary causes of osteoporosis, including cigarette smoking, excess alcohol intake and a history of glucocorticoid use, and other relevant medical comorbidities should be assessed and optimised.11 An assessment of falls risk should be undertaken in all men.
Absolute baseline fracture risk may be estimated through online tools such as the WHO fracture risk assessment tool (Fracture Risk Algorithm [FRAX]; www.shef.ac.uk/FRAX) or the fracture risk calculator from the Garvan Institute (www.garvan.org.au/bone-fracture-risk).6 It should be noted that neither algorithm has been validated for men with prostate cancer who are receiving ADT, and a cross-sectional study found the use of FRAX for fracture prediction to be limited in this population.12
Routine laboratory testing should include measurement of serum calcium, phosphate, creatinine, 25-hydroxyvitamin D and thyroid- stimulating hormone levels, liver function tests and a full blood count.10 Baseline BMD should be measured by DXA. In men with a BMD T-score of --1.5 or less, thoracolumbar x-rays should be undertaken to exclude asymptomatic vertebral fractures.6
Nonpharmacological management
Although high-level evidence specific for nonpharmacological management of men receiving ADT is not available, all men should receive general lifestyle advice for maintaining bone health, including advice to stop smoking and to limit alcohol intake to less than two standard drinks per day. Regular weight-bearing exercise should be encouraged. Although exercise interventions in men receiving ADT have failed to demonstrate an improvement in BMD, a recent systematic review has concluded that exercise improves muscle strength and hence potentially reduces falls and the risk of fractures.13
Local recommendations from Osteoporosis Australia recommend a daily calcium intake through diet of 1300 mg.14 If dietary intake is inadequate, calcium supplementation should be used, unless the patient has a previous history of renal stones. Vitamin D supplementation should be commenced, as necessary, to ensure a target serum 25-hydroxyvitamin D level of 75 nmol/L or more.15
Pharmacological management
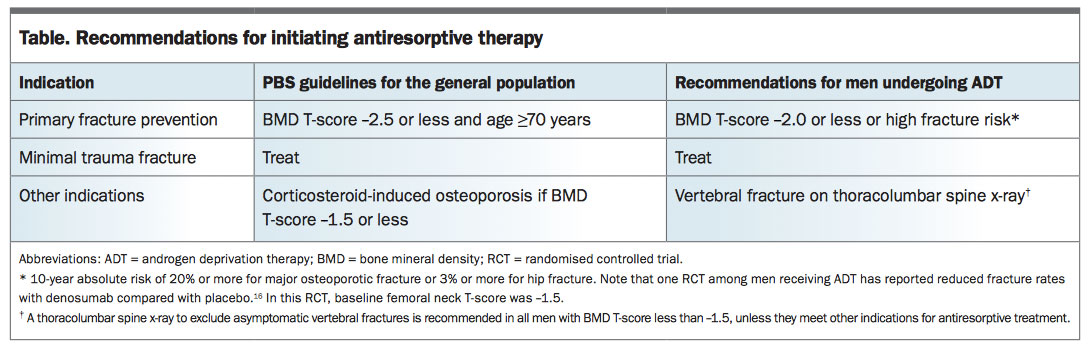
Antiresorptive therapy should be commenced in all men with prostate cancer receiving ADT and who have a history of minimal trauma fracture, unless contraindicated.6 Antiresorptive therapy should be commenced in all men with prostate cancer receiving ADT and who have a history of clinical or radiological fracture, unless contraindicated. There are insufficient data in men with prostate cancer who are receiving ADT to make recommendations regarding commencement of bisphosphonate therapy for primary fracture prevention. Current US National Osteoporosis Foundation guidelines for the general male population recommend pharmacological therapy in men over 50 years of age who have a BMD T-score of --2.5 or less, or a 10-year absolute risk of 20% or more for major osteoporotic fracture or 3% or more for hip fracture.15 However, fracture benefits may be seen at less stringent levels than these recommendations.16
Several randomised, placebo-controlled trials have demonstrated efficacy of bisphosphonates in preventing loss of bone mass in men receiving ADT.17 Current Australian consensus guidelines recommend institution of bisphosphonate therapy for primary fracture prevention in men receiving ADT if their BMD T-score is --2.0 or less.6 However, this recommendation is not aligned with Australian PBS guidelines (see Table). Bisphosphonates are recommended for primary fracture prevention at a BMD T-score of --1.5 or less in patients with corticosteroid-induced osteoporosis, but there is insufficient evidence to recommend this cut-off for men receiving ADT. Implementation of standardised management guidelines including commencement of bisphosphonate therapy (as outlined in the Box) has been shown to maintain a stable BMD despite ADT.9
{kind=link}
{kind=link}
To date, denosumab is the only antiresorptive agent with demonstrated efficacy for fracture prevention in men receiving ADT for prostate cancer, with a significant reduction in new vertebral fractures over 36 months (1.5% vs 3.9% with placebo; relative risk, 0.38).16 This benefit was seen despite a baseline median femoral neck BMD T-score of --1.5, significantly higher than the treatment threshold based on the National Osteoporosis Foundation guidelines. It should be noted that use of denosumab for this indication is not aligned with current PBS guidelines.
The selective oestrogen receptor modulator (SERM), toremifene, has been shown to prevent bone loss and reduce the incidence of new vertebral fractures over 24 months in men receiving ADT for prostate cancer.18 However, its use has been abandoned in this setting due to a higher frequency of venous thromboembolic events.17
Although both bisphosphonates and denosumab have been associated with improvement in BMD, there are no head-to-head trials comparing fracture outcomes between the two agents. Therefore, treatment should be individualised based on patient preference and the side effect profile.
Ongoing monitoring
BMD should be monitored yearly during the initial two years of ADT; thereafter, the monitoring frequency should be individualised. Bone health should be re-evaluated after cessation of ADT, as the gonadal axis may recover in some men. Younger men (<65 years) and those who received a shorter duration of ADT (<24 to 30 months) have a more rapid recovery.6
Conclusion
Plans for commencement of ADT in men with prostate cancer should prompt baseline assessment of bone health in all patients, and the initiation of general measures to maintain bone health. Treatment with antiresorptive therapy is required in a subset of men based on risk factors for osteoporosis and baseline assessment of fracture risk. Further clinical trials are needed to provide a larger evidence base for more definitive recommendations for antiresorptive therapy in men with osteopenia.ET
COMPETING INTERESTS: Dr Nolan: None. Professor Grossmann has received rsearch funding from Bayer Schering, Novartis, Weight Watchers and Lilly and speaker’s honoraria from Besins Healthcare.
References
- Australian Institute of Health and Welfare (AIHW). Prostate cancer. Canberra: AIHW; 2016. Available online at: http://www.aihw.gov.au/cancer/prostate (accessed March 2017).
- Prostate Cancer Foundation of Australia and Cancer Council Australia PSA Testing Guidelines Expert Advisory Panel. Clinical practice guidelines PSA testing and early management of test-detected prostate cancer. Sydney: Cancer Council Australia; 2017. Available online at: http://wiki.cancer.org.au/australia/Guidelines:PSA_Testing (accessed March 2017).
- Karsenty G, Olson EN. Bone and muscle endocrine functions: unexpected paradigms of inter-organ communication. Cell 2016; 164: 1248-1256.
- Vandenput L, Mellstrom D, Laughlin GA, et al. Low testosterone, but not estradiol, is associated with incident falls in older men - the International MrOS Study. J Bone Miner Res 2017; 30 Jan (Epub ahead of print).
- Greenspan SL, Coates P, Sereika SM, Nelson JB, Trump DL, Resnick NM. Bone loss after initiation of androgen deprivation therapy in patients with prostate cancer. J Clin Endocrinol Metab 2005; 90: 6410-6417.
- Grossmann M, Hamilton EJ, Gilfillan C, Bolton D, Joon DL, Zajac JD.
- Bone and metabolic health in patients with non-metastatic prostate cancer
- who are receiving androgen deprivation therapy. Med J Aust 2011; 194: 301-306.
- Hamilton EJ, Ghasem-Zadeh A, Gianatti E, et al. Structural decay of bone microarchitecture in men with prostate cancer treated with androgen deprivation therapy. J Clin Endocrinol Metab 2010; 95: E456-E463.
- Shahinian VB, Kuo YF, Freeman JL, Goodwin JS. Risk of fracture after androgen deprivation for prostate cancer. N Engl J Med 2005; 352: 154-164.
- Cheung AS, Pattison D, Bretherton I, et al. Cardiovascular risk and bone loss in men undergoing androgen deprivation therapy for non-metastatic prostate cancer: implementation of standardized management guidelines. Andrology 2013; 1: 583-589.
- Grossmann M, Zajac JD. Androgen deprivation therapy in men with prostate cancer: how should the side effects be monitored and treated? Clin Endocrinol (Oxf) 2011; 74: 289-293.
- Ebeling PR. Clinical practice. Osteoporosis in men. N Engl J Med 2008; 358: 1474-1482.
- Neubecker K, Adams-Huet B, Farukhi IM, Delapena RC, Gruntmanis U. Predictors of fracture risk and bone mineral density in men with prostate cancer on androgen deprivation therapy.
J Osteoporos 2011; 2011: 924595. - Ostergren PB, Kistorp C, Bennedbaek FN, Faber J, Sonksen J, Fode M. The use of exercise interventions to overcome adverse effects of androgen deprivation therapy. Nat Rev Urol 2016; 13: 353-364.
- Osteoporosis Australia. Resources. Calcium consumer guide. 2nd ed. Sydney: Osteoporosis Australia; 2013. Available online at: http://www.osteoporosis.org.au/resources?cta=Osteoporosis (accessed March 2017).
- Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporos Int 2014; 25: 2359-2381.
- Smith MR, Egerdie B, Hernandez Toriz N, et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med 2009; 361: 745-755.
- Cheung AS, Zajac JD, Grossmann M. Muscle and bone effects of androgen deprivation therapy: current and emerging therapies. Endocr Relat Cancer 2014; 21: R371-R394.
- Smith MR, Morton RA, Barnette KG, et al. Toremifene to reduce fracture risk in men receiving androgen deprivation therapy for prostate cancer. J Urol 2013; 189(1 Suppl): S45-S50.
Single article purchases are temporarily unavailable due to site maintenance.
If you would like to purchase an article during this time, please email us at [email protected] with the article details and we'll assist you directly. We'll also let you know when online purchasing is available again.
Thank you for your patience and understanding.