What’s new in assessing fracture risk?
Bone diseases
Fractures
Opportunities for primary and secondary minimal trauma fracture prevention are often missed. Effective secondary prevention programs in hospitals and improved imaging technology can help, but awareness of the need to prioritise preventing, investigating and treating osteoporosis is key to reducing the serious impact of osteoporotic fractures on the health of patients.
- Currently in Australia, the number of patients who have sustained a minimal trauma fracture who subsequently receive treatment is low.
- Identification of patients who have sustained a minimal trauma fracture is crucial.
- Fracture liaison services have been shown to improve the number of patients receiving treatment after fracture and to reduce the likelihood of subsequent fracture.
- Trabecular bone score is useful in refining the assessment of absolute fracture risk in patients undergoing dual energy x-ray absorptiometry (DXA) scans and has been incorporated into the FRAX absolute fracture risk calculator.
- Improved scanning technology and imaging analytics can aid in detection of prevalent vertebral fractures.
- Bilateral hip DXA scanning increases identification of osteoporosis with negligible additional scanning time or radiation exposure.
- Quantitative methodologies in ultrasound and high-resolution peripheral quantitative CT, as well as three-dimensional DXA, hold future promise for assessing osteoporosis and fracture risk.
In Australia, around 60% of women and 30% of men over the age of 60 years will sustain an osteoporotic fracture in their remaining lifetime.1 The current clinical estimation of fracture risk is based on prior minimal trauma fracture and/or the measurement of bone mineral density (BMD) using dual energy x-ray absorptiometry (DXA). BMD measurement using CT scanning is also used to a lesser extent. Over the past decade, there has been a refinement in models of fracture risk assessment, and in addition there are some interesting new techniques of potential clinical utility on the horizon.
Recent developments available now
Fracture liaison services
Models of osteoporosis care using BMD results are based on the concept of primary fracture prevention, by which treatment aims to prevent the first fracture. Secondary fracture prevention is aimed at treating high-risk individuals who have already sustained an osteoporotic fracture.
In Australia in 2018, there were around 165,000 hospital fragility or minimal trauma fractures (MTFs) recorded in people over the age of 50 years. Once an individual has had an MTF, they are at higher risk of further MTFs. Currently, the number of patients who have had an MTF who subsequently receive treatment is low. The Australian and New Zealand Hip Fracture Registry reported that in 2020, of patients followed up at 120 days after presentation for a hip fracture, only 45% and 38% of patients in New Zealand and Australia, respectively, were receiving bone protection medication to reduce the risk of another fracture.2 This reflects a major missed opportunity to prevent the next fracture. The reasons for the low treatment rate of osteoporotic fractures include low public awareness, medical priority given to higher profile illnesses and the medical profession’s sometimes limited appreciation of the serious impact of osteoporotic fractures on the health of patients. Various secondary prevention programs are increasingly being implemented in public hospitals to improve the management of patients presenting with MTF.
One effective model is the use of fracture liaison services (FLS), which have been shown to improve the number of patients receiving treatment after fracture and to reduce the likelihood of subsequent fracture. Within hospitals, the model for FLS is to identify patients presenting with MTF, as well as those with previously undiagnosed MTF, often silent vertebral fractures, identified on imaging scans. FLS may organise investigations, including DXA to assess future fracture risk, and, when appropriate, initiate treatment. Existing FLS report a reduction of about 30% in the rate of any subsequent fractures and a reduction of about 40% in the rate of major new fractures compared with rates in hospitals without FLS.3 FLS have not only been shown to reduce fracture rates, but also to reduce the cost of managing osteoporosis.4
There are various models of FLS, including the following:
- Type A – identifies patients who have sustained an MTF, investigates and initiates a management plan and treatment, provides education to patients and communicates with stakeholders, including the patient and their GP
- Type B – identifies patients who have sustained an MTF and investigates them before referring the patients back to their GP with recommendations for management and treatment initiation
- Type C – identifies patients with MTF and educates them about osteoporosis, including healthy lifestyle, as well as alerting their GP, who may subsequently manage any assessment or treatment
- Type D – identifies patients with MTF and provides information and education. There is no GP involvement in this model.
In general, type A models are more effective than type B, which are more effective than type C or type D models.5 The specific model implemented depends on the health-care system in place and resources available. Active FLS in major tertiary, large regional and remote hospitals should form part of the standard of care of osteoporotic fractures. A crucial element is effective liaison with the patient’s GP.
Refinement of DXA-enhanced absolute fracture risk
Absolute fracture risk calculators such as FRAX, using DXA-derived BMD and other risk factors, are now commonly available for clinical use. FRAX predicts ‘major’ osteoporotic fractures at four sites (hip, spine, wrist and humerus). The Garvan Fracture Risk Calculator predicts all fragility fractures and uses fewer risk factors. The use of absolute fracture risk has also been incorporated into the Royal Australian College of General Practitioners and Healthy Bones Australia management algorithms.6 Absolute fracture risk assessments provided in bone density reports, for patients over the age of 50 years undergoing a DXA scan, may be useful in better assessing risk and potentially may improve management decisions.6,7
Trabecular bone score
Trabecular bone score (TBS) is a measure of grey-scale homogeneity measured directly from a DXA spine scan using specific software. TBS correlates with trabecular microarchitecture and is an independent predictor of fracture risk. TBS is being increasingly used in refining the assessment of absolute fracture risk in subjects undergoing DXA scans and has been incorporated into the FRAX algorithms. Currently, TBS software can be used in Hologic and GE Lunar densitometers. Use of TBS alone in management decision making is not recommended, but instead TBS should be used in the refinement of absolute fracture risk.8
Improved detection of vertebral fractures
Over 50% of vertebral fractures are silent, i.e. asymptomatic, not coming to clinical attention. Hence the opportunity to investigate these patients and institute treatment is missed. Several methodologies are available to improve the detection of prevalent vertebral fractures.
DXA vertebral morphometry
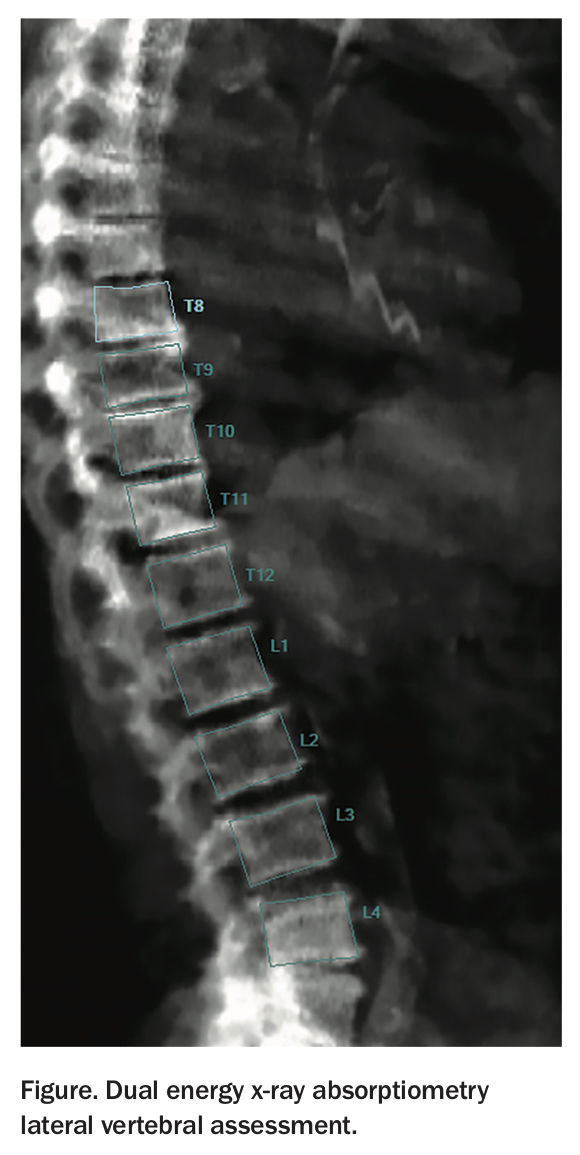
Most recent DXA scanners, with appropriate software, can now provide measurements of individual vertebral dimensions from a lateral scan of the spine (Lunar lateral vertebral assessment, Hologic vertebral fracture assessment; Figure). The use of this facility provides vertebral morphometry assessment at the time of a DXA scan at very low radiation dose, compared with a standard lateral radiograph of the spine. DXA vertebral morphometry expresses the anterior, mid and posterior vertebral heights in relation to the individual vertebral posterior height, and to the corresponding dimensions of the adjacent vertebrae. This information can be used in detecting previously silent vertebral compression fractures (VCFs) and in the monitoring of vertebral deformations to detect new fractures. The current Medicare guidelines define a VCF as a 20% or greater reduction in the anterior, mid or posterior vertebral heights in relation to the posterior height of the same vertebra or to the corresponding dimension of an adjacent vertebra. Currently in Australia, before accessing subsidised therapy on the PBS, confirmation of VCF detected on DXA vertebral morphometry is required using conventional radiography. In summary, low-radiation, DXA vertebral morphometry provides a rapid and convenient way for clinicians to identify patients with unsuspected grade 2 or 3 VCF, thereby identifying high-risk individuals and enhancing care of patients with osteoporosis.9
{kind=link}
Computer-aided diagnosis of vertebral fractures
The reporting rate of incidental VCFs by radiologists remains relatively low, with studies finding only 13 to 32% are reported. Improvement in image analytics, using machine learning and artificial intelligence algorithms, has been shown to provide accurate diagnoses from radiological images. Computer-aided diagnosis software for detection of vertebral fractures has been developed and has the potential to act as an effective screening tool in CT scans of the thorax and abdomen to improve fracture detection and reporting, thus identifying at-risk individuals for secondary prevention of fractures.10
Dual hip DXA scanning
Multiple studies have examined the utility of bilateral DXA hip scans. Most of these studies demonstrate an advantage of bilateral hip scanning. Most studies report that the diagnosis of osteoporosis, based on use of the lumbar spine BMD and a unilateral hip BMD, fails to identify about 10% of subjects with osteoporosis. Dual hip scanning can improve osteoporosis diagnosis with minimal additional time on the DXA scanner and with negligible additional radiation exposure.11,12
Future developments
Quantitative ultrasound (QUS) hips and lumbar spine
QUS utilises the speed of transmission, or the attenuation, of an ultrasound beam through peripheral bone sites (usually the calcaneus) to quantify bone mass. These peripheral measurements have only moderate correlations with axial sites and have a lower reproducibility than the radiological techniques described above. Recent developments of ultrasound now allow direct measurement of the hip and spine to estimate bone mass. This technology has generated considerable interest because of its portability and freedom from radiation. However, the role of hip and spine ultrasound methods in screening for osteoporosis is yet to be accurately defined and at this stage it remains primarily a research tool.13
High resolution peripheral quantitative computed tomography (HR-pQCT)
Microarchitectural deterioration is an integral component of the loss of bone strength with ageing. Standard measurements of bone mass do not provide information on microarchitecture. HR-pQCT allows three-dimensional (3D) bone microarchitecture and volumetric bone mineral density to be assessed in vivo at peripheral sites with low-dose radiation. The use of this technology has improved our understanding of age-related changes and sex differences in bone microarchitecture, as well as the effect of pharmacological intervention. Further longitudinal studies are required to more accurately define the role of HRpQCT parameters in fracture risk estimation and in identifying at-risk patients who will benefit from therapy.14
DXA 3D bone macrostructure
DXA can be used to generate 3D QCT-like models of the distribution of the cortical and trabecular bone mass based on a statistical 3D shape and density model, using a training set of QCT scans, registered onto DXA scans. This technique has been applied to the spine and hip. The methodology could potentially improve osteoporosis and fracture risk assessment in patients who have DXA scans of the lumbar spine and hips, without any additional examination.15 One limitation at present is the considerable additional computing time required of the DXA images.
Conclusion
Fracture risk assessment can be improved using models and techniques that are currently available. New technologies hold the promise for further improvement. ET